
Abstract
Introduction
Biofilms' colonization of indwelling or implanted devices is particularly problematic in medicine. As indwelling medical devices, both permanent and temporary, are increasingly utilized, the number of infections with biofilms causing local or systemic chronic infections also rises. The implications of biofilm-related device infections range from low morbidity to severe systemic infections ending in mortality. These infections are directly correlated to the length of time of device implantation. Otolaryngological indwelling devices include tympanostomy tubes, middle-ear prosthesis, nasal/laryngeal stents, tracheal tubes cannulas, and metallic hardware. 4
The eradication of biofilms from MD is a major healthcare concern. Our goal was to explore one possible solution to this problem. We do not intend to destroy the biofilm but to render it detectable and therefore treatable with antibiotics.
In a preliminary study, it was demonstrated that a Q-shock laser could be used to disrupt Pseudomonas aeruginosa biofilms from polyethylene terephthalate (PET) sutures. 5 In the present study, the potential for laser disruption of biofilm removal from various devices with an emphasis on orthopedic and cardiovascular devices using stainless steel screws and nickel titanium alloy (NiTinol) stents as representative devices was assessed. In addition, the removal of biofilm over time was quantified to determine the time scale of treatment.
Methods
Laser
A small Q-switched Nd-YAG laser (ARC Laser, Nuremberg, Germany and Valam, New York) to generate a “shockwave” (SW) was used. The probe was coupled to a 300-micron optical fiber at one end and a probe with a small opening at the distal end. The hand probe was comprised a titanium target at the tip absorbing the laser energy, causing plasma effect to be emitted later by stress pulses. Titanium was chosen as a target material to generate plasma because of its excellent biocompatibility and high absorption coefficient with respect to the laser wavelength. Another important advantage of solid titanium is its thermal conductivity compared with other metals. The Q-switched Nd-YAG laser was set for a frequency of one pulse per second, each pulse lasting 4 ns at a wavelength of 1064 nm for this experiment, while the output energy was between 8 and 12 mJ, yielding 2 or 3 MW respectively. By exposing a small area to this intense power, an ionic state of matter, known as electrical plasma, was created. The biofilm was exposed to 10–20 laser generated pulses of shockwave. The pressure generated at the tip of the probe is estimated at 2 kbar. Pressure of 2 kbar corresponds to measurements of the laser parameters taken by shadow photography with the fiber–target distance set at 1.5 mm with a linear concordance. The measurement of 2 kbar represents a mean pressure due to possible fiber–target distance variations during the experiment. The pressure (and speed of the wave emitted at the fiber tip) was calculated by shadow photography with a high shutter speed. With the well-known geometry data, the calculated average speed of the precursor shockwave from the target surface to the needle's opening is between 1550 and 1600 m/s. With applying the theory of Raikinon and Huginot, this measured speed of the shockwave corresponds to a pressure of <2.5 kbar at the fiber opening. 6,7 As plasma is retained within the probe tip, the shockwave leaves the probe without any temperature change. The circumference of the surface area affected with one shockwave pulse is measured as 7 × 7 mm. Standardization of laser activation was set as follows: for the high power setting, the laser was activated up to 20 s, while for the lower power setting, the laser was activated for a total of 30 s. The pulse rate was set at f = 1 Hz.
Bacteria and medical devices
Biofilms of the Pseudomonas aeruginosa strain, PittDYFP, which has been constructed to expresse constitutively yellow fluorescent protein (YFP) and has gentamicin as a selective marker, were incubated in 1/10th strength in Luria-Bertani broth. Various medical devices, made from different materials, were then infested with biofilm. Plastic devices included fluoroplastic tympanostomy tube (Medtronic-ENT, Jacksonville, FL) and Shiley tracheostomy tubes (Mallinckrodt Pharmaceuticals, Hazelwood, MO). Metal devices included endovascular stainless-steel wallstent (Boston Scientific/Scimed, Inc., Maple Grove, MN) and coated and uncoated NiTi (nickel-titanium) stents (JNJ-Cordis Corporation, Brunswick, NJ), 316 L stainless steel orthopedic screws (Synthes, Paoli, PA). Polyethylene terephthalate (PET) implantable sutures (Medtronic-ENT) concluded the synthetic materials. The cultures were incubated at 37°C in a humidified 5% CO2 atmosphere on a shaker table at 100 rpm. The medium was replaced daily, and the growth period was 3 days.
Imaging
After 3 days, the devices were rinsed with Ringer solution (Oxoid, Cambridge, UK) to remove loosely adhered bacteria, and gently blotted dry on one side before being fixed to the bottom of a separate 35-mm Petri plate with epoxy glue. The side to be imaged was kept moist with sterile Ringers, and after a 10-min curing period, the Petri plate was flooded with Ringers to immerse the device fully. A small area of the surface, compatible with the area immediately affected by the laser (∼1 mm × 1 mm) was imaged before, during, and after laser application using the time-lapse function of a Leica TCS SP2 AOBS confocal upright DMRXE7 microscope (Leica Microsystems, Exton, PA) with either X10 air objective or a long working distance X63 0.90 NA water immersion lens. The biofilm was imaged by fluorescence of the YFP, and the device was imaged simultaneously by either reflected confocal microscopy or by transmitted light microscopy using the 488-nm laser line. To determine the precise time development of the plasma, the exposure time of the camera dependent on the laser pulse was detected by an oscilloscope and recorded with a personal computer. This allowed the camera exposure to be set in concordance with each laser pulse and the aftershock that followed. The sequence interval for the picture was 20 ns at a camera exposure time of <10 ns.
The difference between remaining and cleared biofilm was represented as the difference between the total area and the area of the medical device on images taken on Imaris confocal microscopy at each time frame. This was achieved by using ImageJ (Rasband, W.S., ImageJ, U. S. National Institutes of Health, Bethesda, MD,
Results
As the experiment was carried out three times on each device at different places on the same sample, only mean, median, and SD values are presented. Due to this fact, we term our experiment observational. We describe in length the particular results for stents and orthopedic screws. Other devices yielded similar results.
Calculation of the pressure waves in the immediate vicinity of the hole and visualization of the vibration of the titanium was achieved. The measured speed of the shockwave, at the probe opening, corresponds to a pressure of ∼2 kbar. Late stages of shockwave propagation show much faster movement than the original waves, reaching pressure amplitude in the range of 8–10 kbar. A small and cold portion of this plasma was seen spreading in the direction of the probe opening but not leaving the probe, thereby avoiding the potential of creating heat damage on the host surface. Biofilm detachment was distance related. With distant pulses (probe distance >10 mm), there was only shaking of the biofilm. However, when the distance between the probe to the biofilm remained around 5–10 mm, some of the biofilm was disrupted immediately, whereas the rest detached with an increasing number of pulses (i.e., 10–20 shockwaves).
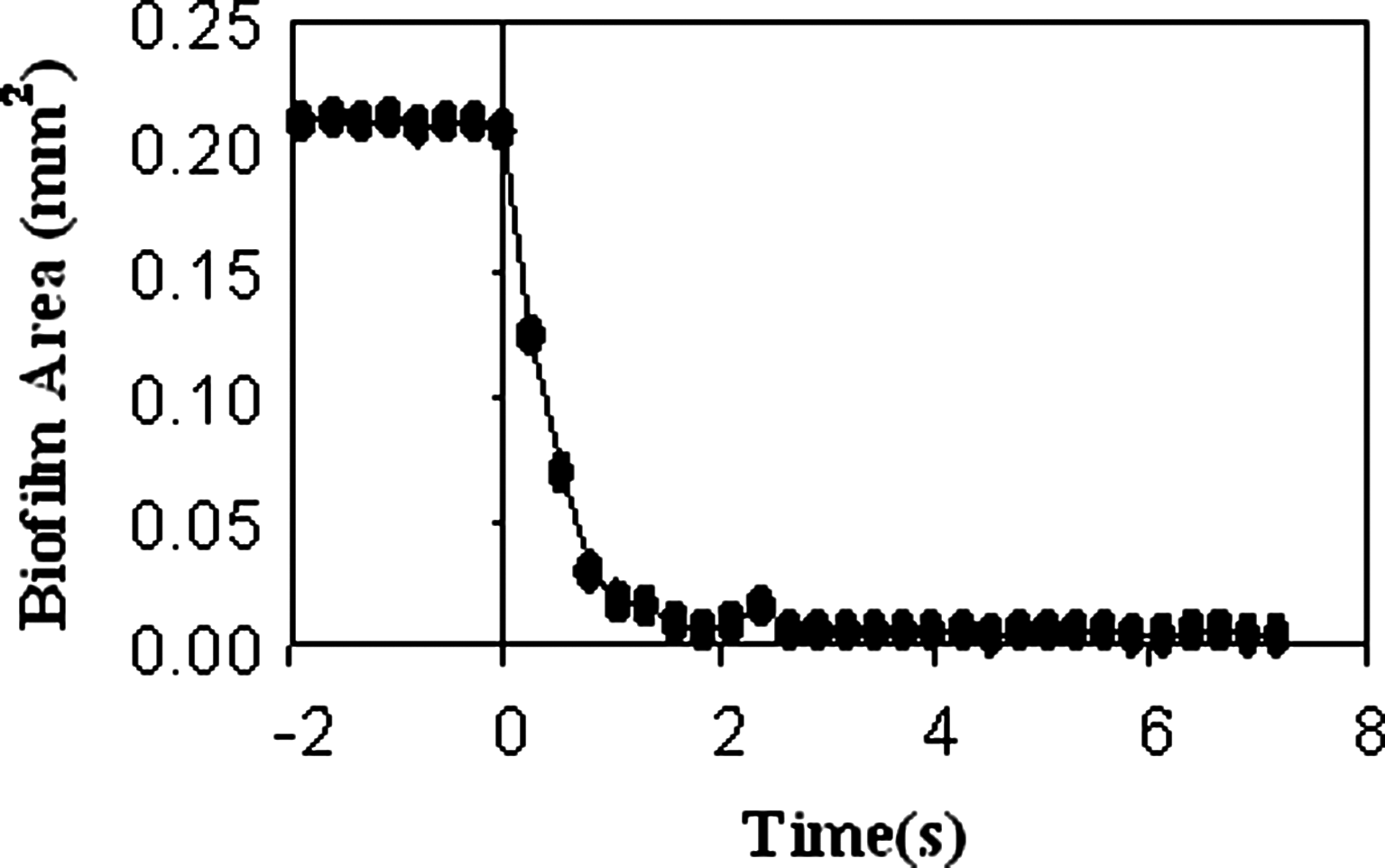
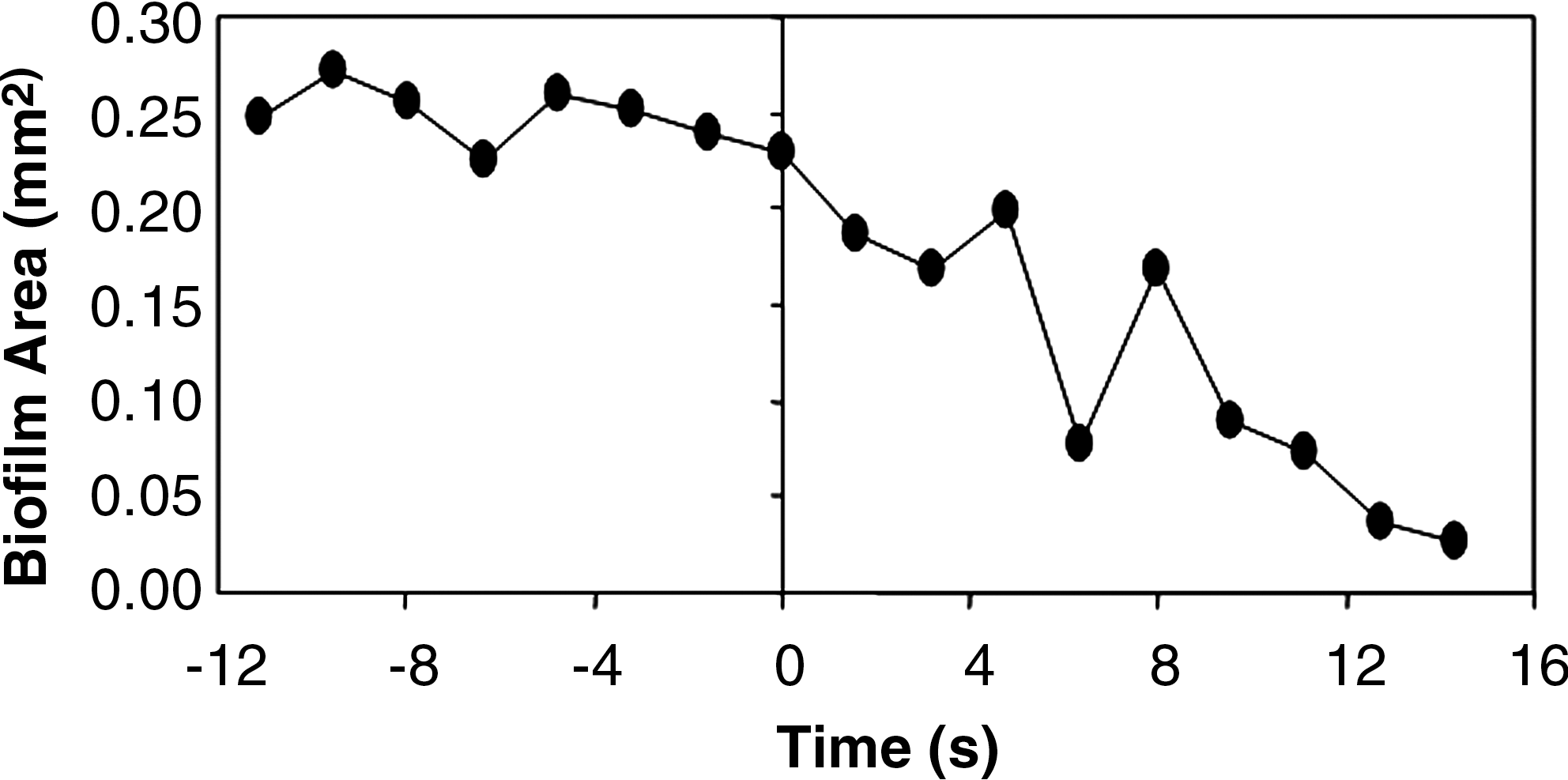
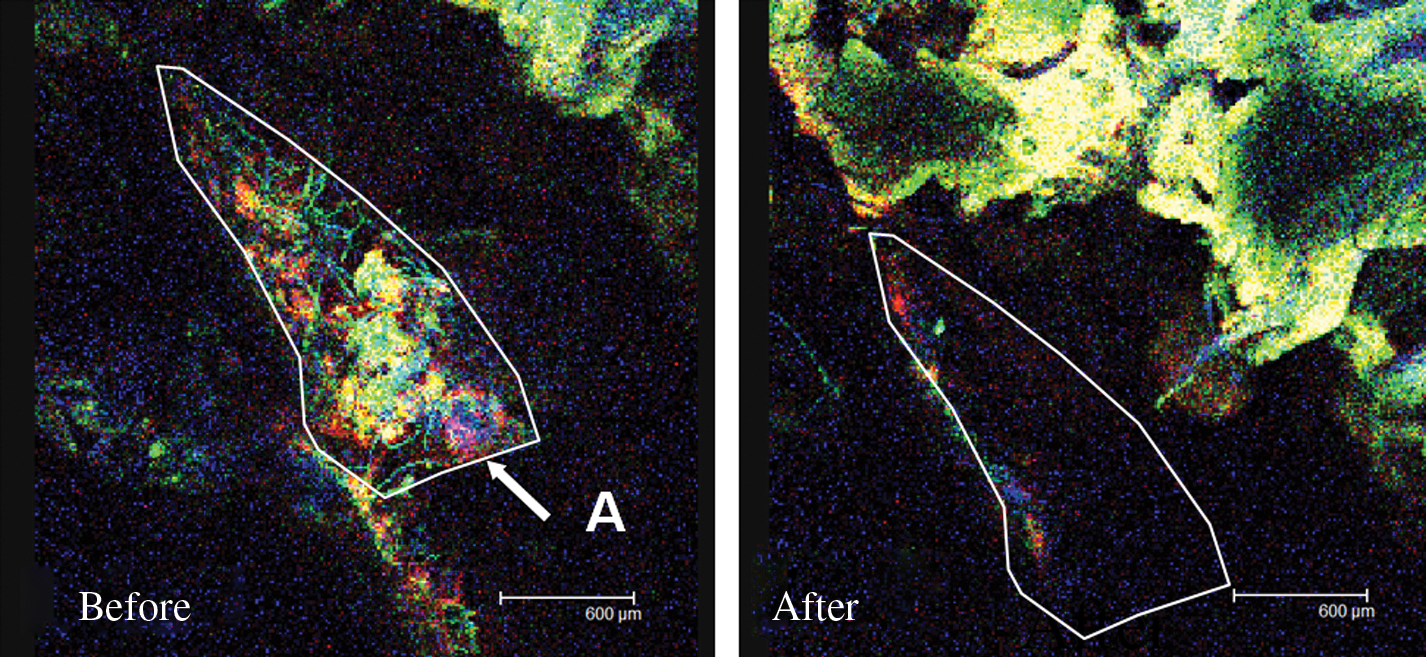
For a low power setting (8 mJ), clearance of the biofilm from a lined stent was seen after a median of 12 s, that is, 12 pulses. When a higher setting of 12 mJ was employed, a median of 9 s was needed. Lined stents receiving high power laser treatment were clear of biofilm after only 1.75 s. Clearance of biofilm from a lined stent with 12 mJ is shown in Fig. 1, with biofilm removal kinetics shown in Fig. 2. Clearance of biofilm from an orthopedic stainless screw is shown in Fig. 3. Calculation of the total area cleared from an orthopedic screw was possible after measuring the subtracted clean screw area from the infested screw, as shown in Fig. 4 and illustrated in Fig. 5. The data including the area of biofilm removed are presented in Table 1. Sinus mucosa infested with biofilm and possibly fungus is shown in Fig. 6. The fraction of biofilm that was removed after 10 s was calculated at 89.5%. To assess statistically the effect of the laser on biofilm reduction, we compared the mean area of biofilm per mm2 in the field of view before and after 20 s of exposure to the laser using a two-tailed t-test assuming equal variance and assuming no difference between the means as the null hypothesis.
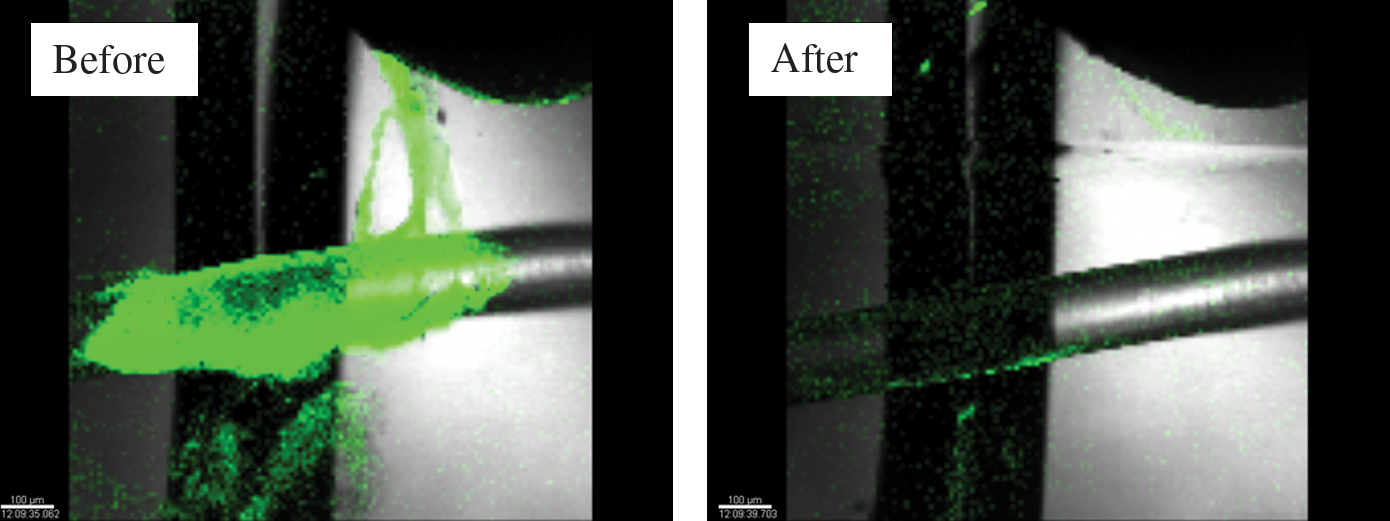
Clearance of biofilm from lined stent with power set at 12 mJ (superimposed fluorescence image on bright field microscopy).
Graph showing biofilm breakage from a lined stent with a power of 12 mJ.
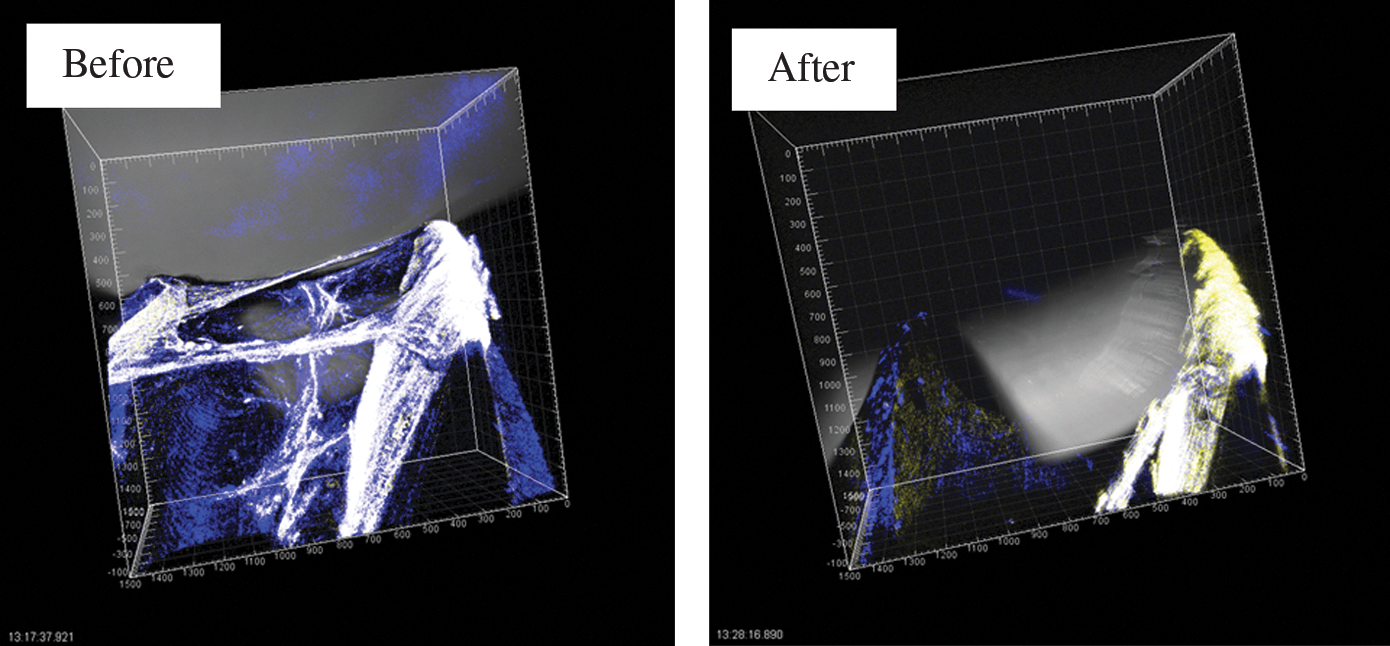
Clearance of biofilm from an orthopedic stainless screw (superimposed fluorescence image on bright field microscopy).
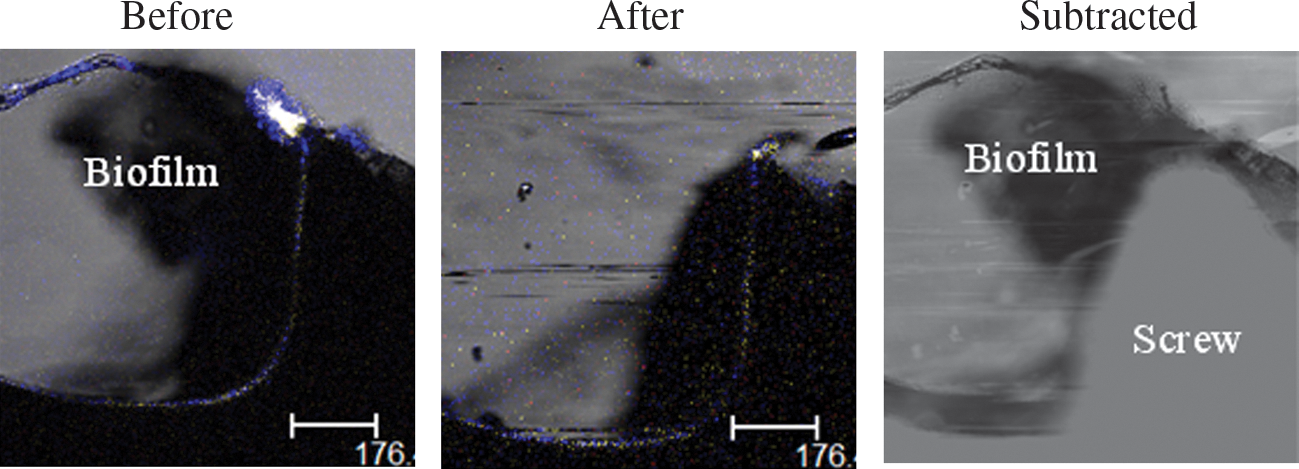
Orthopedic screw showing the subtracted clean screw area from the infested screw (superimposed fluorescence image on bright field microscopy).
Graph showing biofilm breakage from a lined stent with a power of 8 mJ.
Clearance of biofilm from sinus mucosa.
Discussion
Attempts to eradicate biofilm-induced infections have primarily resorted to antibiotics and disinfectants (such as Wang's study with gentian violet 8 ) with mixed results. Antibiotics delivered either systemically or locally with concentrations as high as 1000-fold of moxifloxacin were needed to eradicate Staphylococcal aureus biofilm, 9 while other experiments failed to show Pseudomonas eradication with a concentrated solution of tobramycin. 10 For staphylococcal infections, rifampin combinations are the most evaluated. 1 Other treatments available target biofilm quorum sensing inhibition, 11 introducing enzymes that will degrade the biofilms' matrix, thus enhancing antibiotic penetration, bacteriophages that are strain specific and possess lytic ability, and Gallium compounds acting as antimicrobial potentiator via disruption of iron metabolism. 1,12
Different topical solutions were investigated. Desrosiers showed a pressure irrigation system containing sterile water, citric acid, and caprylyl sulfobetaine to be effective in biofilm reduction. 13 Topical treatment, though semi-mechanical, depend on substance delivery and have long-term material safety issues yet to be demonstrated.
The strategy for implantable medical device infections is somewhat different. Whenever possible, prevention is the first step, including the use of different coatings, such as antibiotic coating mainly with rifampin and minocylcine combinations, or antiseptic coatings with silver or chlorhexidine combinations. Catheter locks follow the same principle with antibiotic or antiseptic locks for prevention. 4,14
Bacterial eradication follows when prevention fails. Electrical treatment (long exposure to direct electrical current), 15,16 sonication with or without vortexing, and ultrasonic external sonic shocks include some of the biofilm disruption and detection strategies. 17
With that in mind, the focus was on a tool that can be useful clinically for a time-limited medical system yet that would stay safe, repeatable, and enhance biofilm detection rate and killing. First proof for biofilms disruption in a cultured plate and raising the possibility for disrupting biofilms from a medical device was performed. 5 This current study showed quantification of biofilm disruption on various and common medical devices in time. Employing a Q-switch laser technology allows us to control energy deliverance with complete accuracy. Dislodgement of 97% of bacteria from different medical devices, made from different materials, such as vascular stents and orthopedic screws was undertaken. Specifically, removing 97.9 ± 0.4% (mean ± 1SD, n = 3) of the biofilm from the surface of a Nitinol (NiTi) stent ranged from 4 to 10 s. This experiment represents the clinical applicability of the time taken and amount of biofilm disrupted from a medical device. Compared with other methods, this method requires a very short albeit focused approach. Moreover, almost all of the biofilm is cleared. However, the dislodged bacteria were not assayed. As a result, one of the drawbacks of our experiment was the lack of surveillance of the remaining biofilm and its ability to “regroup” and create another biofilm matrix, an issue that has not been addressed in previous experiments either. As the biofilm depends on its structure to keep antibiotics from penetrating, securing the dormant bacteria at its core and allowing quorum sensing to break the 3D structure will revert the bacteria to their planktonic shape. It is assumed that, upon disruption, the biofilm ceases to exist. Yet, while in its planktonic form, it is both detectable and amenable to conventional treatment. Future work could focus on the exact parameters of the minimum energy needed to disrupt a specific area of biofilm and which settings are optimal for biofilm disruption.
Conclusion
A Q-switch laser is capable of generating non-thermal mechanical energy deliverance in the form of a shockwave. This pressure is much higher than acoustic pressure and is also much more precise. Biofilms previously attached to implantable medical devices can be exposed and detached by shockwaves generated from a flexible 300-micron diameter fiber. This method may provide a potential solution for treating biofilm-contaminated medical devices by disrupting the protected microorganisms by converting the biofilm bacteria to its planktonic form.
Footnotes
Acknowledgments
This paper was presented orally at the annual 2009 ASLMS meeting in Baltimore, MD.
Author Disclosure Statement
Yosef P. Krespi is a Director at Valam Corp.