
Abstract
Introduction
Early reports regarding LLLT speculated that clinical effects were induced by increased temperature, although some authors claimed that the effects of LLLT radiation were induced by athermic physiological processes. 2–3 More recently, research suggests that LLLT effects are produced by photochemical and photobiological processes. 4 –6 However, in order to induce these therapeutic processes, light energy must not be completely absorbed by the skin and needs to reach subcutaneous tissue. Energy is transformed and stored as heat during the process of absorption and the amount of heating is inversely related to the penetration ability of the light.
Interestingly, there is a lack of research into the thermal effects from commonly used LLLT devices. A search with the terms “thermal effect”, “human skin,” and “laser” in PubMed, Embase, Cinahl, and ScienceDirect (October 2009) yielded no references for class 3B lasers.
Skin color may affect absorption and skin temperature during laser irradiation. Nussbaum 7 found a tendency for infrared LEDs (Light-Emitting Diodes) to produce higher temperatures in human skin folds of participants with dark skin than in those of participants with light skin. Whether skin color influences skin temperature from therapeutic infrared class 3B lasers has not been previously investigated.
The structure, appearance, and biophysical properties of human skin differ between individuals according to their age, sex, and race. The ageing process leads to loss of collagen and elastin fibers, and reductions in the size of epidermal, dermal, and subcutaneous layers contribute to fragility, loss of laxity, and a dry, fine, wrinkled appearance of the skin. 8 –11 Genetic and hormonal influences affect the sun-sensitivity of skin. Females have greater sun-sensitivity than males. 12–13 After menopause, female skin thickness decreases due to lower levels of estrogen. 14–15
Skin color evolved in relation to the amount of sun irradiation in different parts of the world, with populations living close to the equator having darker skin than populations living close to the poles. Human skin color is determined by type and amount of melanin in the skin 16 –19 which has a central role in skin photoprotection. 17,20 Thus, differences in skin color and properties are factors that may influence absorption and production of heat in human skin during LLLT irradiation.
Human skin temperature can be precisely and reliably measured with thermographic cameras. 21 –25 The advantages of thermographic cameras are that they are non-invasive and can be used without being in contact with the skin. The aim of this placebo-controlled study was to investigate the effect on skin temperature in healthy volunteers of differing skin color, age, and gender during irradiation with doses recommended in the World Association for Laser Therapy (WALT) guidelines from two commercially available therapeutic infrared class 3B lasers. A second purpose was to investigate whether irradiation from therapeutic infrared class 3B lasers can produce thermal effects in human skin.
Ethical approval
The study was given ethical approval by REK Vest in Norway (Ref.no: 091.08). Informed consent was obtained from all participants.
Methods
Subjects
A sample of 40 healthy adult volunteers was recruited and divided by gender, age, and skin color. Participants were stratified according to skin color using Von Luschan's chromatic scale, 26 which ranks color from 1 ( = lightest skin) to 36 ( = darkest skin). Three arbitrary categories were used: 1 to 15 = “light” skin, 16 to 28 = “medium” skin, and 29 to 36 = “dark” skin. Participants were also stratified according to age as under 40 years of age, between 40 and 60 years of age, and over 60 years of age on the basis of changes in skin optical properties. 11, 27 Individuals with a history of skin disease were excluded.
Instruments
Skin temperature was measured by a thermographic camera (Flir System, ThermaCAM S65HS, Boston, MA) and ancillary software (ThermaCAM Researcher Pro 2.8 SR-1). This software includes tools to quantify the recorded temperature. The camera measures temperatures with a precision of 50 mK at 30°C, and has an accuracy of ± 2% (Prod. information). The Flir ThermaCAM S65HS used in this study is calibrated once a year against a blackbody, emissivity ɛ = 0.99, distance = 1 meter. Calibration is based on the International Temperature Scale (ITS-90) 28 and performed at the Swedish National Testing and Research Institute. Two commercially available therapeutic lasers were used for irradiation as follows: (a) 810 nm wavelength laser (Thor-DD, London, UK), operated in continuous mode with a mean output power (MOP) of 200 mW, spot size of 0.0314 cm2 and power density of 6.37 W/cm2, (b) 904 nm wavelength laser (Irradia, Stockholm, Sweden) operated in pulsed mode with a peak power of 20 W, pulse width of 200 ns (10−9 s), and frequency of 700 Hz; and with an MOP of 60 mW, spot size of 0.0364 cm2, and power density of 1.67 W/cm2.
Experimental procedure
In order to acclimatize skin temperature, participants remained in the laboratory for 15 min before the experiment started. Participants were instructed that during irradiation they should report to the investigator (a) if they felt any heat sensation in the irradiated area, and (b) if the heat sensation became so uncomfortable that they wanted laser irradiation to be ceased. During the experiment participants sat with their hands on a towel placed on a table (Fig. 1).

Laboratory setup. Thermographic camera placed approximately 25 cm over the subject's hand, with the participant sitting at a table with both hands on a towel.
Recommended irradiation doses according to WALT guidelines are 2 J for 904 nm lasers and up to 6 J for 810 nm lasers. 29
Laser irradiation was performed on the proximal phalanx of the index finger. A neighboring area on the proximal phalanx of the same index finger was used as the control area (Fig. 2).

Thermographic picture (original picture is in color) of the hand after laser irradiation with a dose of 12 joules. Increasing whiteness corresponds to increasing temperature.
One investigator (JHD) operated the thermographic camera, and another investigator (JJ) administered laser irradiation. Each experiment lasted 55 min, with a total of 13 measurements of skin temperature taken from each participant. The first measurement was taken before any irradiation (i.e., baseline). This was followed by six measurements during treatments with different doses of irradiation from the 904 nm laser followed by six measurements during treatments with different doses of irradiation from the 810 nm laser. The sequence of the doses was the same for both lasers, as follows: (a) 2 Joule (J) = 33 s duration from a 60 mW, 904 nm laser and 10 s duration from a 200 mW, 810 nm laser; (b) placebo = 33 s duration from an inactivated 60 mW, 904 nm laser and 10 s duration from an inactivated 200 mW, 810 nm laser (i.e., same duration as 2 J); (c) 6 J = 100 s duration from a 60 mW, 904 nm laser and 30 s duration from a 200 mW, 810 nm laser; (d) 9 J = 150 s duration from a 60 mW, 904 nm laser and 45 s duration from a 200 mW, 810 nm laser; (e) 12 J = 200 s duration from a 60 mW, 904 nm laser and 60 s duration from a 200 mW, 810 nm laser; (f ) placebo = 200 s duration from an inactivated 60 mW, 904 nm laser and 60 s duration from an inactivated 200 mW, 810 nm laser (i.e., same duration as 12 J). Placebo irradiation was delivered using the same laser device as the active interventions but the laser was not switched on. Participants were not aware of this fact. During irradiation, the laser probe was held in a position approximately 10 degrees from vertical, and it was stationary in contact with one spot of skin overlying the dorsal side of the proximal phalange of the index finger. Between each laser irradiation there was a 3 min pause. Participants and the operator of the thermographic camera were blinded to active or placebo treatment condition.
Thermography was recorded during the final 5 s of each irradiation dose and continued for 1 min after the end of irradiation (i.e., a total of 1 min and 5 s). The maximum temperatures from the irradiated area and a control area ulnar to the irradiated area on the same index finger were simultaneously registered by ThermaCAM (Fig. 2).
Main outcome measure
The difference in skin temperature between the irradiation surface area and the control area was calculated for each irradiation dose and each laser.
Statistical analysis
Microsoft Excel (Microsoft Office Excel 2007) was used for statistical analysis and graphics. Student's pairwise T-tests and ANOVA were used for comparison of statistical differences with a significance level set at p < 0.05. Pearson's correlation coefficients were calculated to determine relationships between irradiation doses and skin temperature.
Results
Forty volunteers expressed interest in taking part in the study, provided written consent, and were included (Table 1).
The baseline skin temperature after acclimatization was 30.7°C (SD ± 2.8) in the proximal part of the index finger.
Placebo irradiation with a treatment time corresponding to the 2 J conditions changed mean skin temperature in the irradiated area by − 0.9°C (SD ± 0.7) for the 60 mW, 904 nm laser, and − 0.2°C (SD ± 1.2) for the 200 mW, 810 nm laser. Placebo irradiation corresponding to the 12 J treatment conditions changed mean skin temperature by 0.4°C (SD ± 1.2) for the 60 mW, 904 nm laser, and 0°C (SD ± 1.1) for the 200 mW, 810 nm laser. There were no significant temperature differences between the irradiated and control areas on the index finger (no p value less than p < 0.05).
The tip of the laser probe was in skin contact during laser irradiation, and the probe tip temperature was also measured immediately after irradiation. The probe tip temperature ranged from 31.8°C (SD ± 1.8) to 32.6°C (SD ± 2.0) for the 200 mW, 810 nm laser and from 30.1°C (SD ± 2.2) to 33.7°C (SD ± 3.4) for the 60 mW, 904 nm laser for the irradiation doses from 2 to 12 J (Table 2).
All participants completed the six irradiation doses with the 60 mW, 904 nm laser. Participants with light and medium skin completed six irradiation treatments with the 200 mW, 810 nm laser. However, 8 of 13 participants with dark skin withdrew consent to continue the experiment because they felt uncomfortable heating in the irradiated area with the 200 mW, 810 nm laser. Two of these participants withdrew consent during a 6 J irradiation dose (as recommended by WALT), four withdrew consent during a 9 J irradiation dose, and two withdrew during a 12 J irradiation dose.
Skin temperature at the time of withdrawal showed a large variation between participants. The participant with the highest measured increase in skin temperature (relative to the control area) during irradiation with the 200 mW, 810 nm laser was a male with dark skin aged 45 years. The skin temperature increased by 11.2°C during a dose of 2 J, and 22.3°C during a dose of 6 J (irradiation was interrupted by the investigators and he was not irradiated with doses of 9 and 12 J). The subject and experimental data related to withdrawals are summarized in Table 3.
Participant completed irradiation with the 6 J dose (and did not start the 9 J dose).
There was a positive correlation between increasing irradiation doses and increased skin temperature for both lasers and all skin color groups (Pearson's r = 0.98 – 0.99, withdrawals omitted from analysis).
For light and medium skin, no significant thermal effects (p ≥ 0.16 for any comparisons) were observed when irradiating at doses recommended in the WALT guidelines 29 (i.e., 2 J for 904 nm, and 6 J for 810 nm), with temperatures increasing less than 1.5°C regardless of laser type. However, highly significant increases (p < 0.0001) in skin temperature were observed when irradiating dark skin: 6.1°C (SD ± 3.2) for the 2 J dose and 9.2°C (SD ± 4.5) for the 6 J dose, using the 200 mW, 810 nm laser. Also, irradiation with a 2 J dose using the 60 mW, 904 nm laser induced a lower but nevertheless significant (p = 0.043) increase in skin temperature, 1.9°C (SD ± 1.8), in dark skin (Figs. 3 and 4).
Doses in joules plotted against temperature change in the three skin color groups during irradiation with the 60 mW, 904 nm laser (n = 40). The change in temperature was defined as the difference between temperatures in the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD). *Significant differences between the light-skin group and the dark- and medium-skin groups (p < 0.01). †Significant differences between light- and medium-skin groups and the medium- and dark-skin groups (p < 0.05).

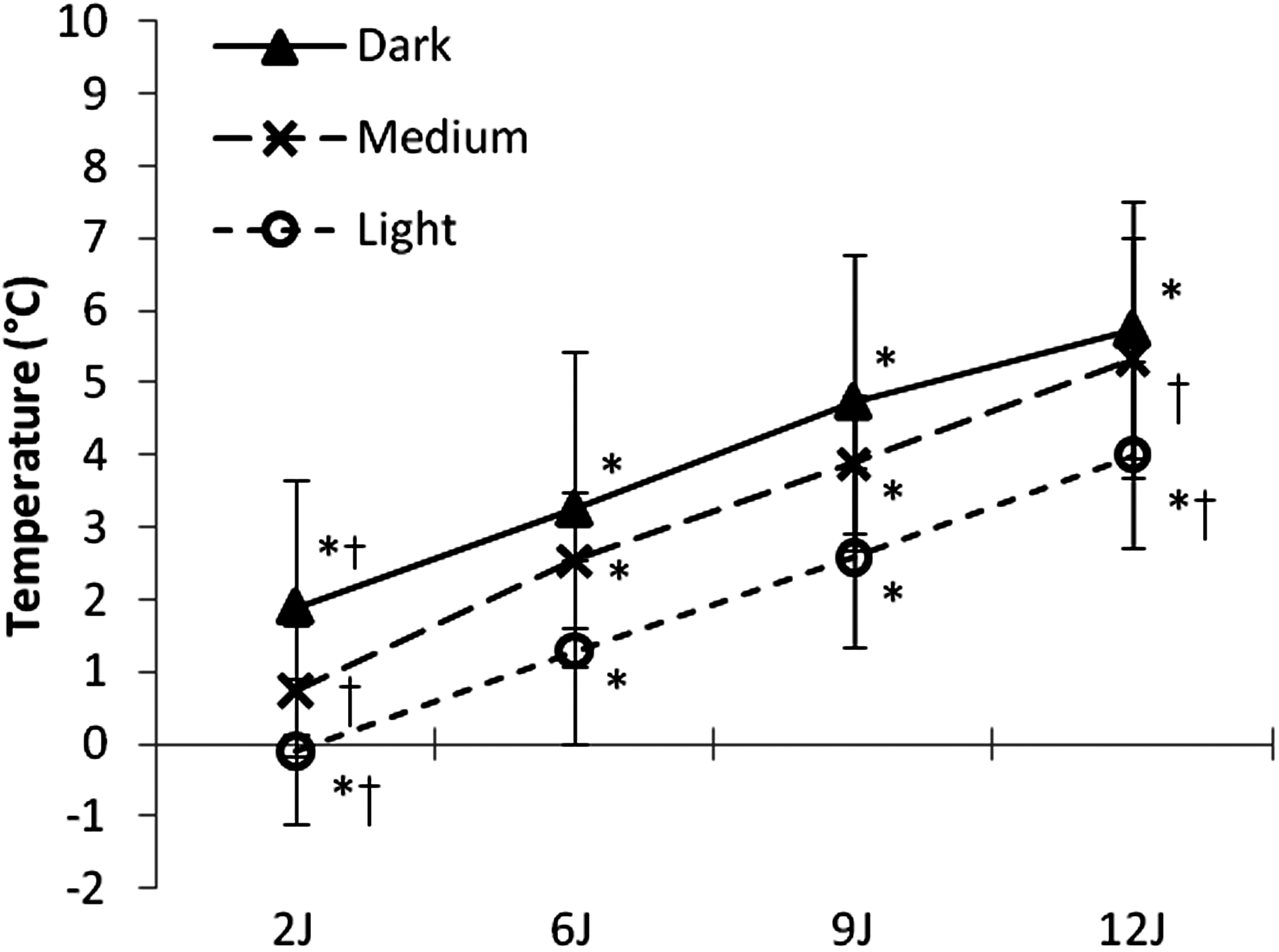
Doses in joules plotted against temperature change in the three skin color groups during irradiation with the 200 mW, 810 nm laser (n = 40). The change in temperature was defined as the difference between temperatures in the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD). * Significant differences between the dark-skin group and the medium-and light-skin groups (p < 0.01). † Significant differences between the medium-skin group and the light-skin group (p < 0.05). a) Six and b) eight of thirteen participants with dark skin withdrew because of uncomfortable heating in the LLLT-spot area.
During the four active irradiation doses from LLLT, the temperature change in dark skin was significantly higher than that in light skin for all irradiation doses, regardless of laser type (p < 0.01). During these four doses, delivered with the 60 mW, 904 nm laser, the mean temperature difference between the irradiated area and the control area ranged from − 0.1°C (SD ± 1.0) to 4.0°C (SD ± 1.3) in light skin, from 0.7°C (SD ± 0.9) to 5.3°C (SD ± 1.7) in medium skin, and from 1.9°C (SD ± 1.8) to 5.7°C (SD ± 1.8) in dark skin (Fig. 3). During irradiation with the 200 mW, 810 nm laser, thermal effects were small in light skin, ranging from 0.3°C (SD ± 0.8) to 1.5°C (SD ± 1.2), and moderate in medium skin, ranging from 0.7°C (SD ± 1.4) to 3.3°C (SD ± 1.2). In dark skin, thermal effects were substantial, from 6.1°C (SD ± 3.2) to 9.8°C (SD ± 2.3) across doses from 2 to 12 J (Fig. 4).
When equivalent irradiation doses, of 6 J or more, were administered to light and medium skin, there were larger increases in skin temperature for the 60 mW, 904 nm laser when compared with the 200 mW, 810 nm laser (p < 0.05) (Table 4).
Significant (p < 0.05) differences during use of different lasers.
Significant (p < 0.01) differences during use of different lasers.
Due to the high withdrawal rate (62%) of participants in the dark-skin group during irradiation with the 200 mW, 810 nm laser, comparison of skin temperature for the two lasers was problematic in this group.
In contrast to the results in light and medium skin, identical doses of laser irradiation resulted in significantly higher skin temperatures in dark skin (p ≤ 0.001) for the 200 mW, 810 nm laser. Irradiation doses of 2 and 6 J with the 200 mW, 810 nm laser induced a threefold increase in temperature in dark skin when compared with the 60 mW, 904 nm laser (Figs. 3 and 4).
There were no significant differences in skin temperature between males and females during laser irradiation when using doses at or above those recommended by WALT (no p-value lower than p ≥ 0.24). Adjusting for skin color by removing dark-skin data from the analyses did not affect this result (Figs. 5 and 6).

Doses in joules plotted against temperature change in males and females during irradiation with the 60 mW, 904 nm laser (n = 27). The change in temperature was defined as the difference between temperatures between the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD).
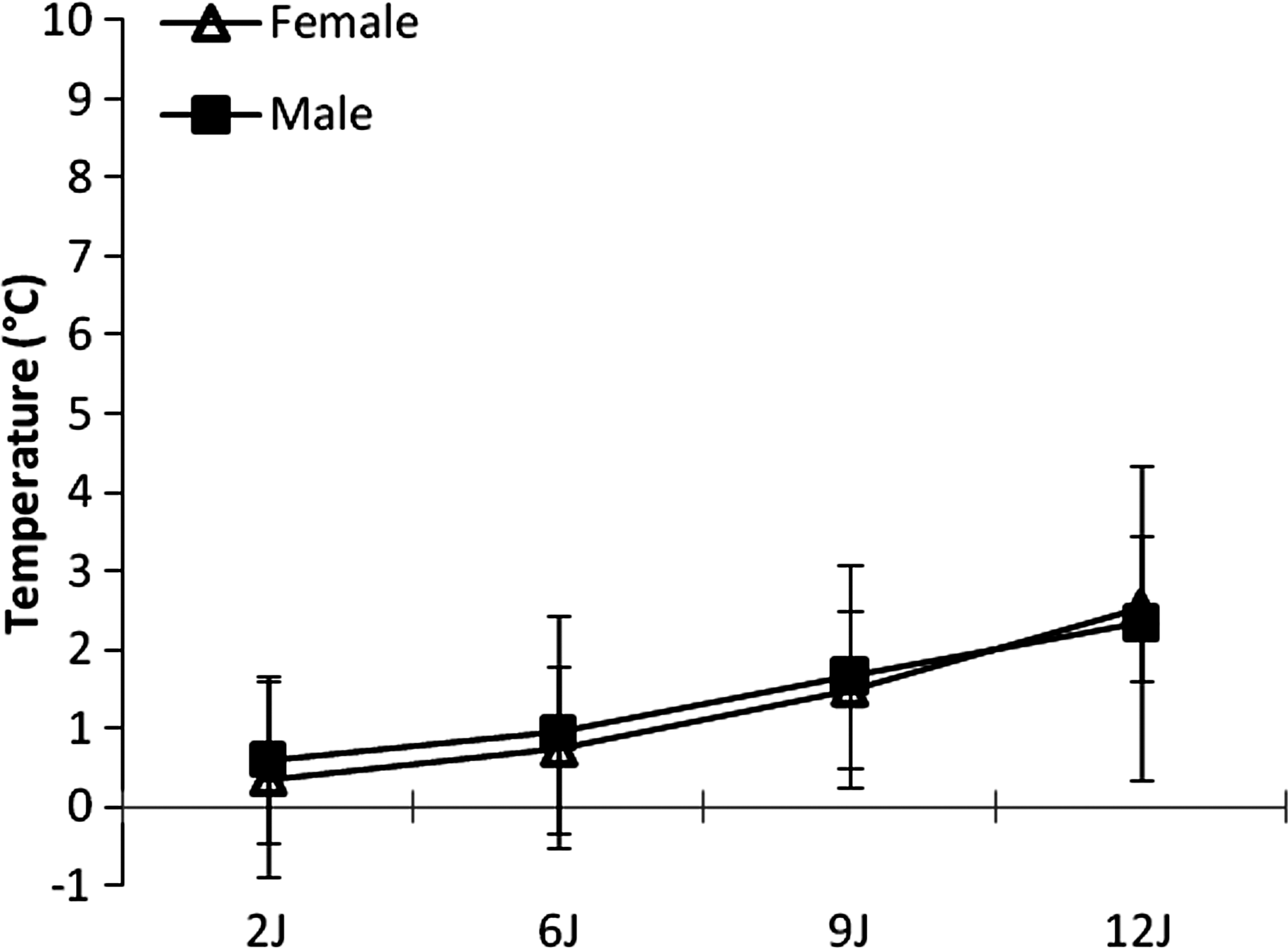
Doses in joules plotted against temperature change in males and females during irradiation with the 200 mW, 810 nm laser (n = 27). The change in temperature was defined as the difference between temperatures in the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD).
There was a tendency toward higher skin temperatures in the irradiated area in younger participants (under 40 years of age) for both lasers, although comparisons with older participants just failed to reach statistical significance (p ≥ 0.06). There was evidence that there were larger differences for higher doses with the 200 mW, 810 nm laser than for doses recommended by WALT, and that the differences persisted when dark-skin data were removed from the analysis (Figs. 7 and 8).
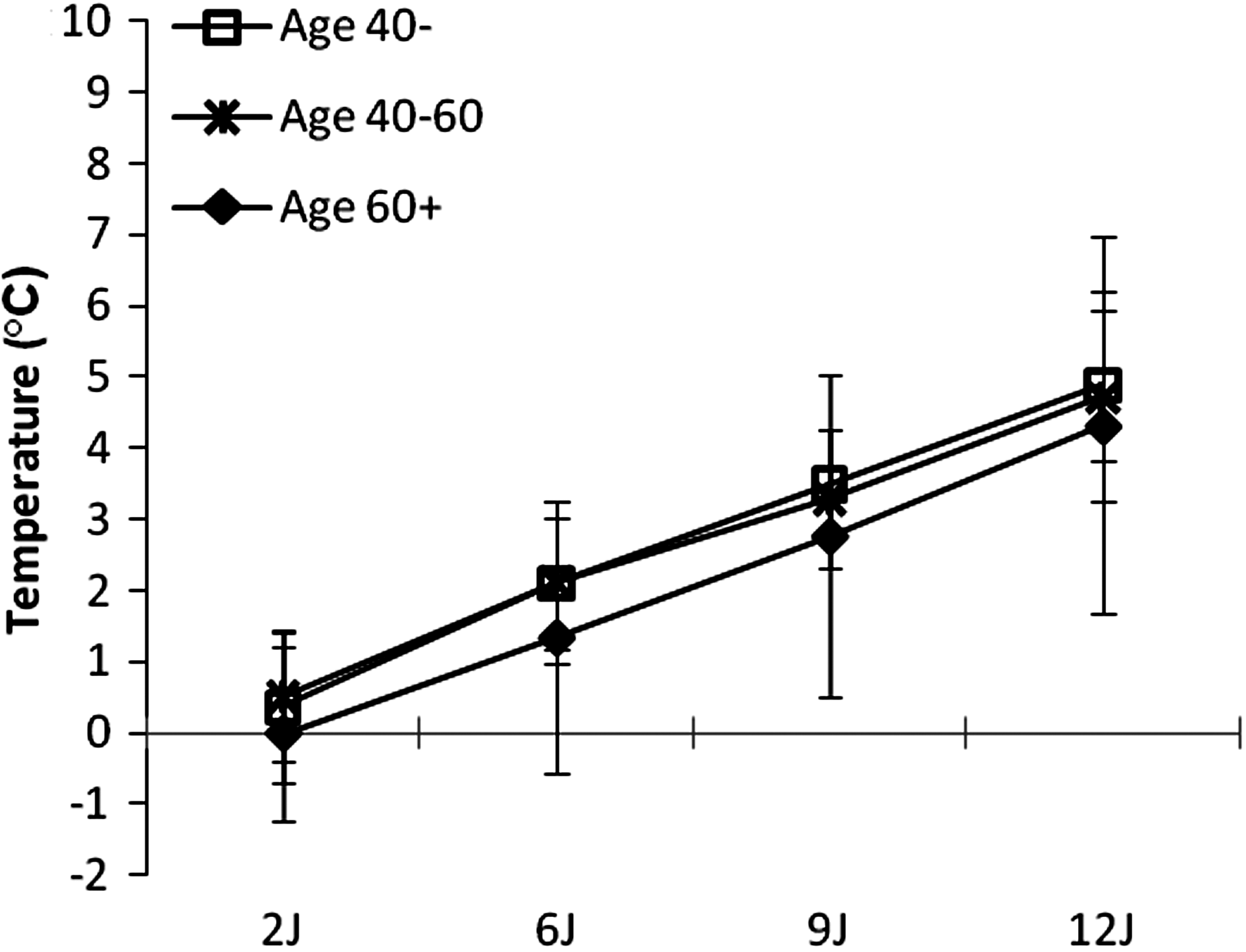
Doses in joules plotted against temperature change in the three age groups during irradiation with the 60 mW, 904 nm laser (n = 27). The change in temperature was defined as the difference between temperatures in the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD).
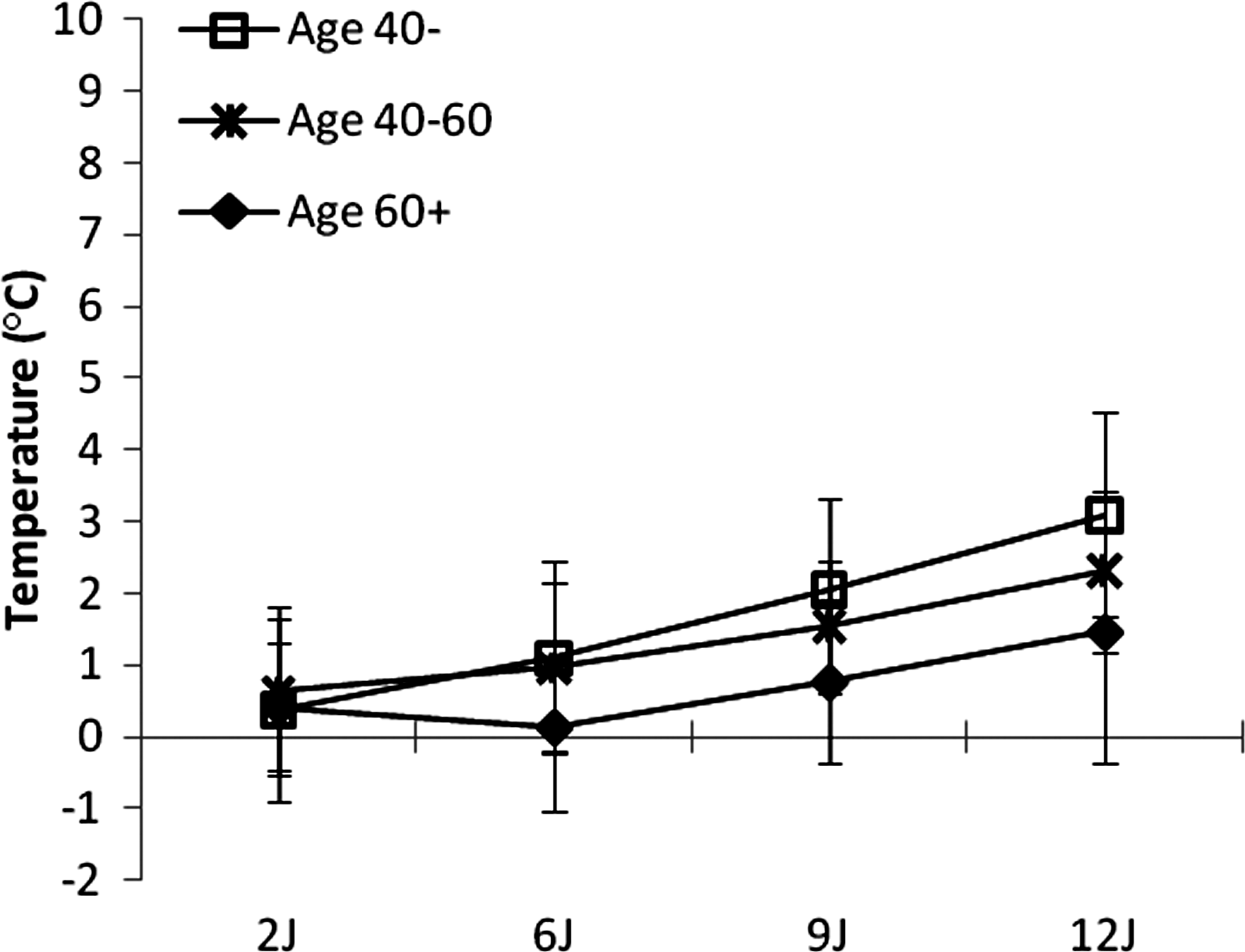
Doses in joules plotted against temperature change in the three age groups during irradiation with the 200 mW, 810 nm laser (n = 27). The change in temperature was defined as the difference between temperatures in the irradiated area (laser spot) and a control area 1 cm ulnar on the same index finger (error bars ± SD).
Discussion
In this study, we investigated the effects of irradiation using two commercially available class 3B lasers on human skin temperature for subjects of different skin color, age, and gender. In the early days of LLLT, it was speculated that treatment effects were of thermal origin and similar to heat therapy. 30 However, research in the 1980s supported claims that doses used in clinical practice were too low to produce noticeable thermal and biological reactions in the human body. 31 Subsequent research in the 1990s into the biophysical properties of LLLT irradiation suggested that the therapeutic effects of LLLT irradiation resulted from non-thermal mechanisms. 32 In recent years, more powerful class 3B laser devices have arrived on the market, with laser manufacturers claiming that “more powerful is better”.
Thermoregulation of the skin is mainly controlled by the hypothalamic nuclei. Heating of small areas of skin by conduction results in activation of skin thermoreceptors and leads to the release of nitric oxide which acts directly on blood vessels to dilate the vessels and thereby regulate body temperature. 33 –36 Central thermoregulation acts to regulate changes in larger areas of the body, such as the entire index finger, and cannot result in local temperature differences like those we found between the two measurement areas on the proximal phalanx of the index finger.
We observed a consistent thermal effect of laser irradiation, which was strictly limited to the area of the irradiation spot. Skin temperature decreased to that of the surrounding areas within 15 s after irradiation had ceased. We interpret this effect as laser light absorption and subsequent heating of the skin, because it was clearly limited to the area of irradiation and did not spread to the control site, which was 1 cm away from the irradiated site on the same index finger. We also observed an increase in skin temperature which started proximally in the hand and then spread to the fingers in several participants following irradiation with 6 J (100 s) or more from the 904 nm laser. Interestingly, the temperature difference noted between the irradiation spot and the control area was statistically significant despite the increase in background temperature across the entire hand. We infer from these observations that laser irradiation initiates central thermoregulatory mechanisms that affect skin circulation in the skin surrounding the area of irradiation. Slow-onset circulatory effects lasting more than 120 s after irradiation have been reported in humans following 2 min of irradiation with 74 mW, 810 nm laser 37 and 20 min of irradiation with a 30 mW, 632 nm laser 38 and in rabbits after 10 min with a 10 mW, 904 nm laser. 39 Evidence also suggests that equal doses below 10 J delivered over a longer period of time stimulates cell activity and modulates inflammation to a greater extent than lasers with higher MOP using shorter irradiation times. 40–41
Thermal effects in the human skin need to reach a threshold magnitude before they are perceived by individuals. Recent studies have shown that there is spatial summation of warming sensation thresholds in the human hand ranging from 35.4°C (±1.0) when large areas (9 cm2) are heated to 42.3°C (±3.0) when small areas (2 cm2) are heated. 42 During irradiation, heat could either stem from the absorption of laser light or transfer of heat energy from the laser probe to the skin by conduction as the laser probe heats during production of the laser beam. Our measurements of the temperature of the laser probe tips immediately after irradiation suggest that the probe tip was not responsible for elevations in skin temperature; probe temperatures were below 34°C with doses of 12 J, and below 32°C with doses recommended by WALT. 29 The thermal effects for doses recommended by WALT were below the warmth sensitivity thresholds for human skin for the respective lasers. This is particularly important because the sensation of warmth can compromise blinding of active and placebo laser units in research studies.
Guinot 12 found that female skin is more sun-sensitive than male skin, but we did not find any significant differences in skin temperature between males and females during infrared laser irradiation. Structures and entities of the human skin do change with age and this change could result in modified skin sensitivity to laser irradiation. Even though there was a tendency to more heat production in younger skin (under 40 years of age) than in older skin, we did not find significant differences in skin temperature according to age.
Our results showed that the heat induced in human skin during LLLT irradiation is strongly related to skin color. Skin temperature was higher at all irradiation doses for participants with dark skin than for those in other skin color groups, regardless of laser type. Skin temperature differences for the 60 mW, 904 nm laser were moderate (about 4°C) during irradiation doses from 2 to 12 J, and increased according to dose in a linear manner for all skin color groups. While the dose-temperature profile was linear for light- and medium-skin groups with the 200 mW, 810 nm laser, the induced thermal effects were higher in darker skin. One study using LEDs with an 840 nm infrared wavelength found no significant differences between participants with different skin colors but there were few participants with the darkest skin color in the sample and the power density for the LED source was low and only 1–2% of the power density used in the present study. 7
The significant heating of dark skin by the 200 mW, 810 nm laser has implications for irradiation safety and clinical practice. There was a three- to sixfold increase in skin temperature in dark skin, reaching 42–43°C, when compared with light and medium skin. This temperature corresponds to the threshold for painful thermal stimuli 43 and was achieved even at small laser irradiation doses.
Both lasers used in this study were classified as class 3B, and their irradiation spot sizes were almost identical, 0.0364 cm2 (60 mW, 904 nm) and 0.0314 cm2 (200 mW, 810 nm). The authors see no reason why such a small spot size difference would affect temperature to any appreciable degree. Therefore, it is necessary to consider differences in wavelengths, MOP, and irradiation mode (continuous vs. pulsed) between the lasers as possible causes of the study results. Infrared wavelengths penetrate human skin more readily than red wavelengths. 1, 44 However, there are only minor differences (<20%) in rat skin penetration for wavelengths within the near-infrared spectrum, with 810 nm penetrating slightly more than 904 nm wavelengths. 45 The observed differences in our study seem to exceed what can reasonably be explained by wavelength differences. We expected that the largest increase in skin temperature would occur using the 200 mW, 810 nm laser because its MOP is approximately three times greater than the 60 mW, 904 nm laser, and it has a shorter irradiation time. However, skin temperature increased more in light and medium skin during irradiation with the 904 nm laser. It seems unlikely that a physiological response such as more rapid removal of excess heat should occur during and after irradiation with the stronger 810 nm laser than the 904 nm laser. Future studies are required to investigate in greater detail the influence of MOP and irradiation mode (pulsed vs. continuous) in heat production on human skin during laser irradiation.
There is strong clinical evidence, reflected in the WALT guidelines, that pulsed 904 nm lasers have lower optimal dose ranges in musculoskeletal disorders than continuous 810 nm lasers, possibly because less energy is lost in the skin barrier with the pulsed 904 nm laser. 46 Our results from light and medium skin may be seen as contradictory to this suggestion because equal doses yielded significantly higher skin temperatures with the pulsed 904 nm laser than with the continuous 810 nm laser.
During LLLT in which the thermal effect on the skin is small, the irradiated energy facilitates other photoprocesses in the local tissue. Infrared irradiation stimulates photobiological reactions through photoacceptors that take part in metabolic reactions in the cells. 47 –54 As the purpose of irradiation during LLLT is to reach structures beneath the skin layers, the significant thermal response in dark skin raises a question as to whether sufficient energy reaches subdermal target tissue. Our results suggest that the 200 mW, 810 nm laser should probably not be used clinically with doses at or above 6 J in persons with dark skin.
Conclusion
The thermal effects of LLLT at doses recommended in the WALT guidelines for musculoskeletal and inflammatory conditions are negligible (<1.5°C) in light- and medium-colored skin. However, at higher irradiation doses delivered with a strong class 3B laser (200 mW), LLLT is capable of increasing skin temperature significantly, and these photothermal effects may exceed the thermal pain threshold for humans with dark skin. The thermal effects in dark skin were most pronounced during irradiation with the 200 mW MOP, 810 nm laser; 62% of participants withdrew because of uncomfortable heating in the irradiated spot area. There were no significant differences between age groups or between gender groups in skin temperature during laser irradiation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.