
Abstract
Introduction
Given this situation, the need to find an alternative treatment for methicillin-resistant Staphylococcus aureus (MRSA) infections has received great interest. However, variations in the clinical course of osteomyelitis as a result of micro-organism virulence, host resistance, and the reaction to inflammation of bone and periosteum, have made it difficult to compare treatment approaches. Moreover, the wide range of surgical techniques and adjuvant therapies used to treat the disease, as well as the high potential for relapse, has made a comparison between studies problematic. 5,10
Light therapy has been proposed as an effective treatment for a variety of human conditions. 11,12 Laser therapy plays an important role in healing by inhibiting the development of bacteria in infected wounds, 13 and both in vivo and in vitro studies have demonstrated that light at a wavelength of between 405 and 880 nm has a bactericidal effect on S. aureus. 8,9,11,13 –15 The increasing use over the past 15 years of Gallium-Aluminum-Arsenide (GaAlAs) diode lasers, which have a higher depth of penetration than other types of lights used in light therapy, offers the clinician a penetrative tool of great efficiency. 16
Although the use of laser therapy accompanied by an exogenous photosensitizer to treat osteomyelitis has been previously described, 17 our review of the literature found no studies examining the use of laser therapy alone. This study was intended to investigate whether a laser light wavelength of 808 nm at different energy densities might be effective in the treatment of chronic osteomyelitis induced experimentally in the rat tibia.
Methods
Animal material
The study was conducted with 39 male Wistar albino rats ∼4 months in age and weighing an average of 220 g (range: 200–250 g). All procedures were performed in accordance with an approved protocol reviewed by the Atatürk University Faculty of Veterinary Sciences Ethical Committee for Animal Care and Use, and in full compliance with the Helsinki Declaration of Animal Rights. Rats were placed in pairs in cages in a room with a 12-h daylight/darkness cycle and an ambient temperature of between 23°C and 28°C. Rat chow and water were provided ad libitum.
Bacteria
We used a clinical isolate of a MRSA bacterium sensitive to vancomycin and resistant to methicillin. Bacteria were incubated in a Staphylococcus medium (Oxoid, CM145) broth at 37°C for 24 h. Colonies were transferred directly from the plates to a spectrophotometer (Ultraspec 2000, Pharmacia, Cambridge, Great Britain) and diluted with 0.85% NaCl until a McFarland 0.5 standard was obtained. Inoculates of 1 × 105 colony-forming units (CFU)/100 μl were prepared from the bacterial suspension and used for intramedullary administration. 18,19
Induction surgery
Chronic osteomyelitis was induced in rat tibias following the method described by Zak et al. 20 While the rats were under general anesthesia with xylazine (5 mg/kg) and ketamine (75 mg/kg), their left legs were shaved, and skin disinfection was performed using povidone iodine. A 1-cm longitudinal incision was made in the anteromedial aspect of the tibia. After subcutaneous and periosteal dissection, a twist drill (1.0-mm diameter) was used to prepare an intramedullary cavity in the pattello-tibial tendon to a depth of approximately 1 cm, with the entry point between the tibial plateau and the tibial tuberosity. Subsequently, 10 ml of 5% sodium morrhuate (Scleromate, Glenwood, USA), a sclerosing agent, was injected into this opening to induce local irritation. 21 Next, 100 μl of 1 × 105 CFU S. aureus and 0.2 ml of a 0.9% NaCl solution were injected into the medullar cavity, and the fascia and skin layers were surgically closed. Animals were closely monitored after surgery, but their functional activity was not restricted, and no systemic or local antibiotics were administered. Osteomyelitis was allowed to develop over the 3-week period following inoculation surgery.
Treatment groups
Once intramedullary cavities had been prepared in the left tibias of all rats, Group 1 (sham, positive control group), consisting of 5 rats chosen at random, was established. This group was injected with 0.1 ml saline solution alone to the tibia defect. Osteomyelitis was induced in all remaining rats, and subjects were randomly assigned to one of 5 groups. No treatment was administered to Group 2 (negative control, non-treated infected group) (n = 6). Debridement surgery alone was performed on Group 3 (n = 7). Debridement surgery plus laser irradiation of exposures of 60 secs (6 J at 7.64 J/cm2: n = 7), of 120 secs (12 J at 15.29 J/cm2: n = 7), and of 180 secs (18 J at 22.93 J/cm2: n = 7) was performed on Groups 4, 5, and 6, respectively (Fig. 1).
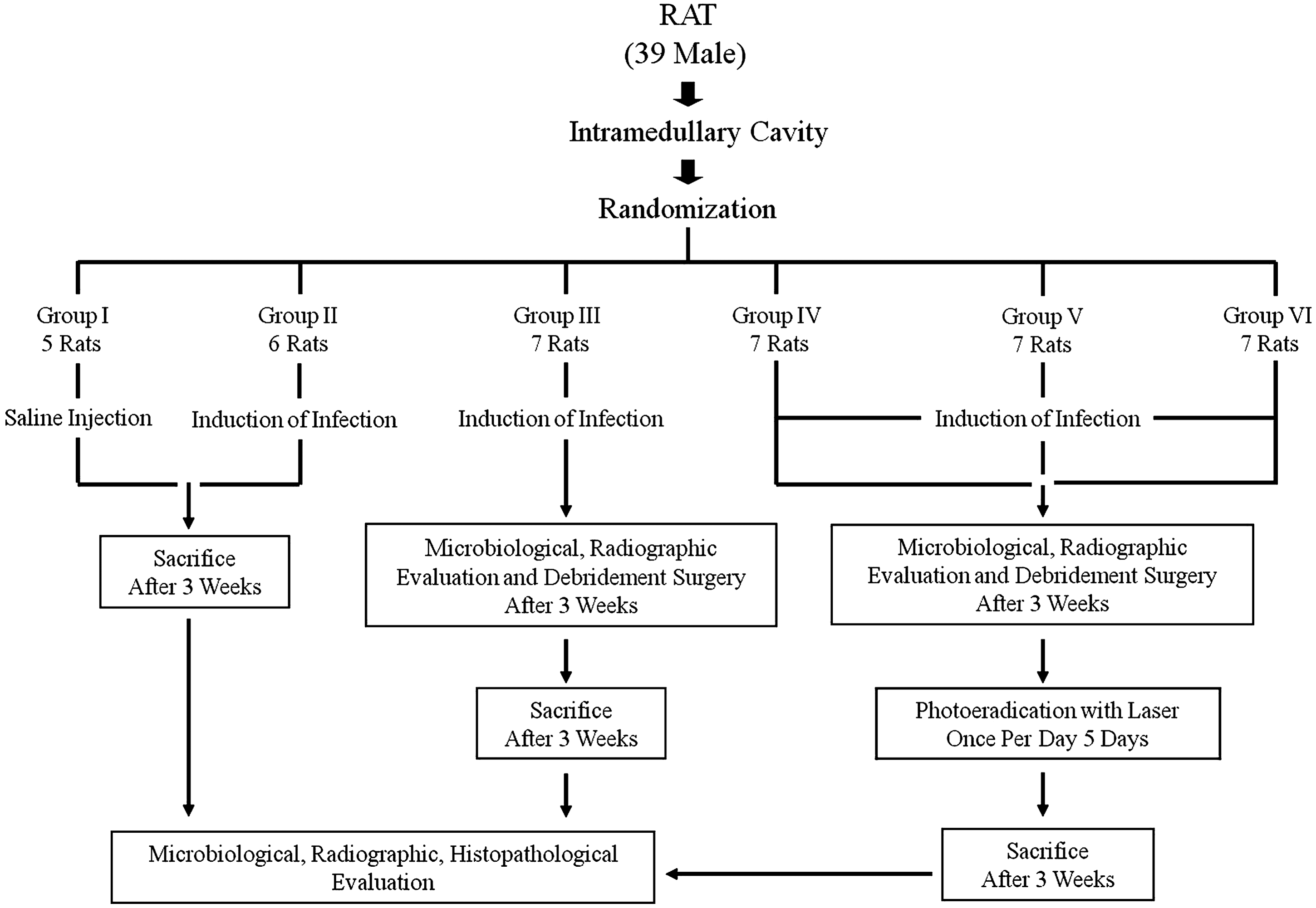
Experimental design.
Debridement surgery
Figure 2 shows a view of rats after induction and before debridement surgery. Rats in Groups 3–6 underwent debridement surgery 21 days post-induction. Using the initial surgical approach, the area of the defect was exposed, and swab cultures were taken to confirm the successful induction of osteomyelitis. This was also confirmed radiographically. Infected and necrotic soft tissue was removed to the maximum extent possible, and the canal was flushed with 100 ml 0.9% saline solution to remove any loose debris and remaining bone marrow. Fascia and skin layers were surgically closed and disinfected.

Clinical appearance of a rat with induced osteomyelitis, immediately before debridement surgery. Sinus formation, pus discharge and soft-tissue inflammation in the tibia are visible.
Laser treatment
Photoeradication of bacteria was undertaken utilizing an 808 nm, 100 mW continuous-wave GaAlAs diode laser (‘Doctor Smile’, Lambda Laser Products, Vicenza, Italy). Laser irradiation was applied perpendicularly at a distance of ∼1 cm to a single point on the surface of the wound, resulting in a 0.7854 cm2 circular beam spot (irradiance = 127.3 mW/cm2). Laser treatment commenced immediately after debridement surgery and was applied daily for 5 consecutive days. Irradiation durations were 60 secs (6 J at 7.64 J/cm2: n = 7), 120 secs (12 J at 15.29 J/cm2: n = 7) and 180 secs (18 J at 22.93 J/cm2: n = 7).
Animal sacrifice
Rats in Groups 1 and 2 (sham and negative control groups) were killed 21 days post-induction surgery and rats in Groups 3–6 at 42 days post-induction, using a lethal dose of thiopental (200 mg/kg) administered intraperitoneally (200 mg/kg). 22 Left tibias were then harvested for histopathological and bacteriological examination.
Radiographic analysis
Mediolateral (M/L) and anterioposterior (A/P) radiograms (Diagnox Floatex Model, Meditronics, Mumbai, India) of the left tibia were taken 21 days post-induction surgery and 21 days post-debridement surgery, the following parameters being assessed: (1) periosteal reaction; (2) diaphyseal widening; (3) osteolysis; (4) sequestrum formation; and (5) bone deformation. Parameters 1–3 were graded from 0–3 (0 absent, 1 mild, 2 moderate, 3 severe). Parameter 4 was graded as either 0 or 1 (absent or present). 23 Bone deformation was graded from 0–4 according to percentage of deformed bone area to normal bone area (0, normal, no change compared with right tibia; 1+, elevation and/or disruption of the periosteum; soft-tissue swelling; 2+, 10% disruption of normal bone architecture; 3+, 10–40% disruption of normal bone architecture; and 4+, 40%+ disruption of normal bone architecture). 24
Microbiological analysis
Bone specimens taken under aseptic conditions from all animals after death and during debridement surgery were placed in sterile tubes and weighed by a microbiologist blinded to the specimen groups. Following weighing, 10 ml of saline solution was added to each specimen and mechanically homogenized inside a sterile bag using a stomacher. Specimens were serially diluted and prepared with the tryptic soy agar plating technique. After incubation for 24 h at 37 °C, bacteria multiplying on plates were identified, and a colony count (CFU/g) was performed.
Histopathological analysis
Tissue samples were fixed in 10% buffered formalin. These were then decalcified in a hydrochloric acid/formic acid working solution 20 times their own volume. A fresh solution was provided each day until decalcification was complete. This process took 96 h. Specimens were next thoroughly washed under running tap water and routinely embedded in paraffin. Sections 5 μm thick were placed on polylysine-coated slides and stained with hematoxylin and eosin (H&E). Slides were randomized and examined at x40 magnification under a light microscope (Olympus BX51; Olympus Corp., Tokyo, Japan) by a pathologist blinded to the specimen groups. Disease severity was assessed according to the technique described by Smeltzer et al. 25 , by scoring intra-osseous acute inflammation (IAI), intra-osseous chronic inflammation (ICI), periosteal inflammation (PI), and bone necrosis (BN) using 0–4 scales. IAI classification was: 0, not present; 1, minimal-to-mild inflammation with no intramedullary abscess; 2, moderate-to-severe inflammation with no intramedullary abscess; 3, minimal-to mild-inflammation with intramedullary abscess; and 4, moderate-to-severe inflammation with intramedullary abscess. ICI classification was: 0, not present; 1 minimal-to-mild chronic inflammation with no significant intramedullary fibrosis; 2, moderate-to- severe chronic inflammation with no significant intramedullary fibrosis; 3, minimal-to-mild chronic inflammation with significant intramedullary fibrosis; and 4, moderate-to-severe chronic inflammation with significant intramedullary fibrosis. PI classification was: 0, not present; 1, minimal-to-mild inflammation with no subperiosteal abscess formation; 2, moderate-to-severe inflammation with no subperiosteal abscess formation; 3, minimal-to-mild inflammation with subperiosteal abscess formation; and 4, moderate-to-severe inflammation with subperiosteal abscess formation. BN classification was: 0, no evidence of necrosis; 1, single focus of necrosis without sequestrum formation; 2, multiple foci of necrosis without sequestrum formation; 3, single focus of sequestrum; and 4, multiple foci of sequestra. Samples with a total Smeltzer score (SS) of at least 4 out of a maximum of 16 were considered positive for osteomyelitis.
Statistical analysis
Results were analyzed using SPSS version 17.0. Histopathological and radiological differences among groups were analyzed using the Mann–Whitney U test. Bacteria counts were subjected to log transformation for normalization and then analyzed using the Mann–Whitney U test. p < 0.05 was regarded as statistically significant.
Results
Histopathological results
In Group 2 (negative control group), dense polymorphonucleated leukocytes (PNL), macrophages, degenerated cells, necrotic cells, apoptotic cells, vascular congestion, periosteal inflammation, and bone necrosis were observed, together with a low level of plasma, lymphocyte, and vascular proliferation. In Group 3 (debridement, no laser treatment), decreases in PNL and vascular congestion and increases in plasma, lymphocyte, and macrophage levels were observed relative to the negative control group. In Groups 4, 5, and 6, numbers of lymphocytes and vascular congestion levels decreased as laser doses increased, and vascular proliferation, newly formed bone, and fibrous tissue were observed (Fig. 3).
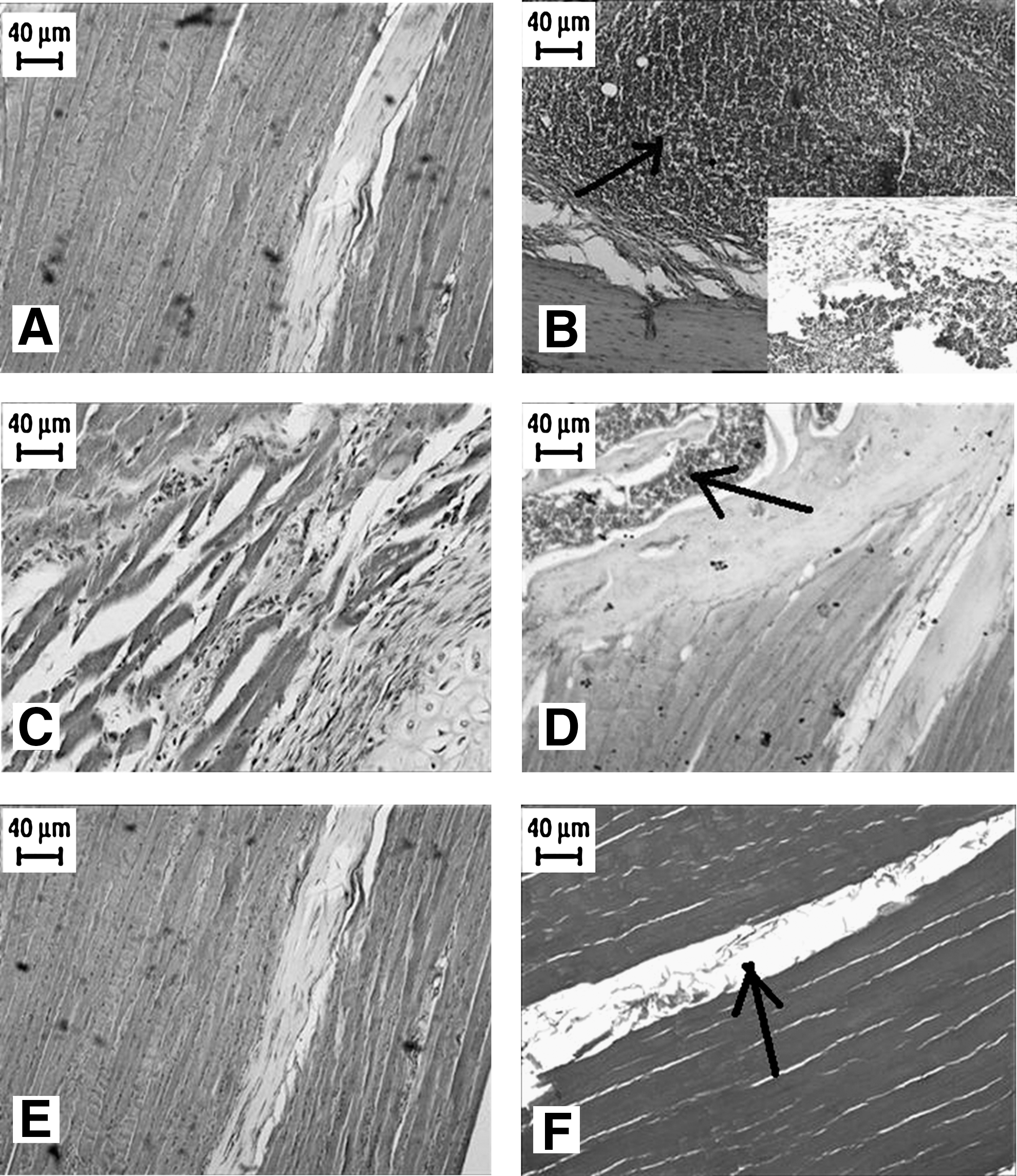
Light micrographs of rat's left tibia.
Statistically significant differences between the sham and negative controls were observed for IAI, PI and BN (p = 0.003) and for SS (p = 0.004). However, there was no significant difference between the sham and negative controls for ICI (p = 0.80). Compared to the negative control group, IAI, PI, BN, and SS in Group 3 (debridement, no laser treatment) decreased by 59% (p = 0.002), 69% (p = 0.001), 65% (p = 0.002), and 37% (p = 0.004), respectively, whereas ICI increased by 257% (p = 0.017). Increasing doses of laser light in addition to debridement caused a linear decrease in values for all parameters, reducing them to the levels of the positive control (sham) group (0.0 vs. 0.86 for SS). In Group 4, IAI, PI, BN, and SS decreased by 67% (p = 0.001), 73% (p = 0.001), 92% (p = 0.002) and 67% (p = 0.002), respectively, whereas ICI increased by 43% (p = 0.128) in comparison to the negative control group. In Group 5, IAI, ICI, PI, BN, and SS decreased by 80% (p = 0.002), 14% (p = 0.642), 81% (p = 0.002), 100% (p = 0.001), and 81% (p = 0.002), respectively, in comparison to the negative control group. In Group 6, IAI, ICI, PI, BN, and SS decreased by 93% (p = 0.001), 37% (p = 0.942), 100% (p = 0.000), 100% (p = 0.000), and 93% (p = 0.001), respectively, in comparison to the negative control group (Fig. 4).
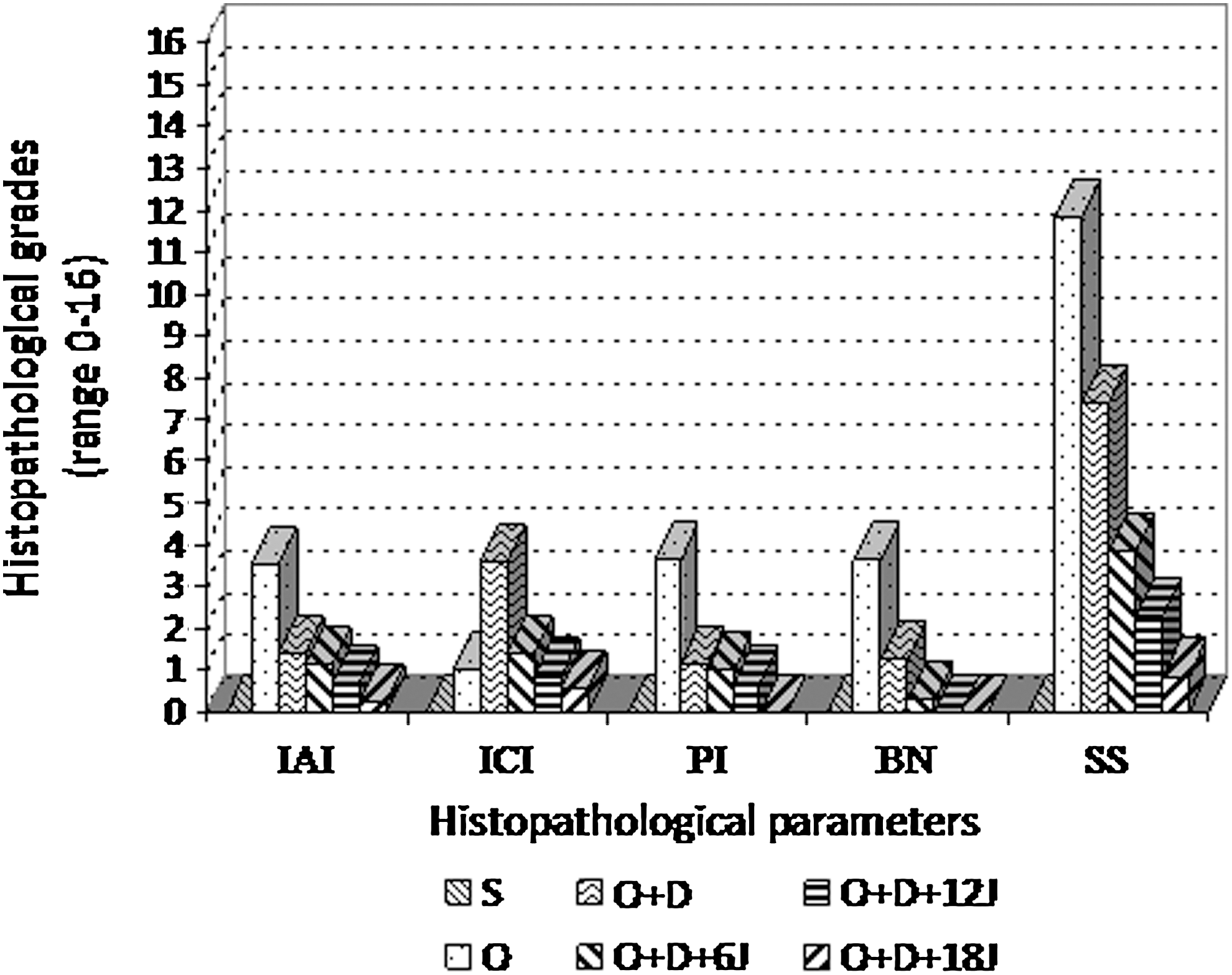
Histopathological data as scored using the score of Smeltzer et al. 25 The maximum scores are 4 for IAI, ICI, PI, and BN and the maximum score at Smeltzer score (SS) is 16. IAI, intra-osseous acute inflammation (SEM = 0.22); ICI, intra-osseous chronic inflammation (SEM = 0.27); PI, periosteal inflammation (SEM = 0.13); BN, bone necrosis (SEM = 0.14); SS, Smeltzer score (SEM = 0.35); S, sham; O, osteomyelitis; D, debridement; J, joule.
Microbiological results
Rates of infection clearance were confirmed microbiologically. The highest bacteria count (5 × 105) was observed in Group 2 (negative control). A 26% (1.6 × 104, p = 0.01) reduction in bacteria count was observed in Group 3 (debridement only), whereas reductions of 54% (4.3 × 102, p = 0.003), 70% (5.5 × 101, p = 0.003), and 91% (3.3 × 100, p = 0.002), respectively, were observed in Groups 4 (debridement plus laser irradiation with 7.64 J/cm2), 5 (debridement plus laser irradiation with 15.29 J/cm2) and 6 (debridement plus laser irradiation with 22.93 J/cm2). No statistically significant differences were observed in bacteria count between Group 1 (sham) and Group 6 (p = 0.11) (Table 1). No MRSA was isolated in four rats in Group 6.
CFU, Colony-forming units; S, Sham; O, Osteomyelitis; D, Debridement; J, Joule; Log (BC), Logarithm (Bacteria count).
Radiographic results
Analysis of radiographs taken 21 days post-induction revealed areas of bone lucency, diaphysis deformation, periosteal reaction, diaphyseal widening, and osteolysis in the cortex of the affected area that were attributed to the osteomyelitic process. No significant differences were observed between the post-induction (21 days) and post-treatment (42 days) radiographs (Table 2) (Fig. 5).

O, Osteomyelitis; D, Debridement; J, Joule; %, percentage of deformed bone area to normal bone area; PR, Periosteal reaction; OL, Osteolysis; DW, Diaphyseal widening; BD, Bone deformation; t 1, Day 21 post-osteomyelitis induction; t 2, day 42 post-osteomyelitis induction (day 42 post-debridement surgery).
Discussion
This study clearly demonstrates the ability of laser therapy to successfully treat MRSA chronic osteomyelitis in rats. Antibiotic treatment of osteomyelitis is still a challenge to the physician. 26 S. aureus encodes the penicillin-binding protein PBP2a in the presence of the genetic element known as staphylococcal cassette chromosome mec (SCCmec), thus reducing the affinity of β-lactam antibiotics to MRSA. 27,28 Some studies have reported that MRSA is resistant even to vancomycin, which is considered a proven line of defense against bacteria. 8,29 The continuing genetic development of MRSA hinders effective pharmacological treatment of osteomyelitis 8 and increases the need for an alternative. 8,9,30 In addition to its other therapeutic characteristics, 10 –13 light therapy's bactericidal effect may represent grounds for hope in the treatment of infected wounds that resist pharmacological treatment.
A variety of in vitro and in vivo studies have reported positive results using laser therapy for the eradication of MRSA. Enwemeka et al. 8 investigated the effects of 470-nm laser light on MRSA and reported that energy densities of 3, 7, and 35 J/cm2 eradicated, respectively, 30%, 60%, and 80% of bacteria, suggesting that low-dose laser treatment may be a practical and inexpensive alternative to pharmacological treatment. In a study using a wavelength of 660 nm and energy densities between 18-180 J/cm2, Lipovsky et al. 30 showed that an energy density of 180 J/cm2 reduced S. aureus colony numbers by 99.8%. De Simone et al. 14 investigated the bactericidal effect of laser light on MRSA at wavelengths of 632-nm (energy densities between 0.1–0.4 J/cm2) and 670-nm (energy densities between 2.5–10 J/cm2) and established a bactericidal effect at even the lowest doses for both wavelengths, with the effect rising in line with increasing doses. Guffey and Wilborn 11 combined 405- and 880-nm lasers in their study of MRSA, reporting a bactericidal effect at all energy densities between 1 and 20 J/cm2, with the maximum effect observable at 20 J/cm2.
Gad et al. 31 evaluated the bactericidal effects of laser light on MRSA in experimentally induced soft-tissue infections in rats. Using a diode laser at a wavelength of 660 nm (energy densities between 10 and 160 J/cm2), they reported that the bactericidal effect rose in line with increasing energy densities, with a reduction of >99% in bacteria colony numbers at an energy density of 160 J/cm2. 31 However, in another study in which 405-nm was applied, the authors reported a non-linear increase in bactericidal effect, with an increase in energy density from 1.0 to 15 J/cm2 resulting in a greater increase in bacteria death than with an increase in energy density from 15 to 60 J/cm2. They suggested that consecutive small doses might be more effective than a single large dose. 9 Whereas some researchers have suggested that the increase in bactericidal effect is not linear after 15–20 J/cm2, 8,9 others have reported a linear increase at higher energy densities, as well. 30,31 In our study, bactericidal effect rose linearly as doses increased; however, as we were limited to maximum exposures of 180 secs (18 J at 22.93 J/cm2), it was not possible to estimate the effect of higher doses. Further studies are needed in order to arrive at a definitive judgment.
Differences in the designs and irradiation regimes employed make it difficult to compare findings among studies. Due to variations in such factors as spot diameter, exposure time, operating mode (continuous vs. pulse) and the condition of the target organism, it is only possible to compare the effects of total energy delivered. 15 Rather than attempting to define the maximum cell kill attainable using higher doses, as described by some investigators, we chose modest light-dose regimens to identify the extent of cell kill that could be expected with relatively low-level irradiation. 17,30,31
Identifying the precise mechanism governing how light kills bacteria is beyond the scope of this study. According to Gates, 32 the thymidine and cytosine pyrimidine bases of DNA are able to absorb light energy, so that irradiation of a base opens its bond, allowing it to react with nearby bases to bring about structural changes; when the level of DNA damage exceeds the level of repair, the cell exposed to the laser dies. Another study suggested that light may be absorbed by the porphyrin produced by bacteria or cause an increase in free radicals, 33 which could then affect the cytoplasmic membrane proteins and DNA 34 or directly impact on the photolabile pigments in bacteria. 35
Some in vitro studies have used staining to increase the light-sensitivity of cells, thus establishing a bactericidal effect at lower doses. 14 However, the artificial chemical agents used tend to be highly cytotoxic, limiting their clinical application. 15 Like many other studies, we did not use staining. Bisland et al. 17 reported successful treatment of S. aureus-induced osteomyelitis both in vivo and in vitro using a 75 J/cm2 dose of 635 ± 10 nm laser light laser in conjunction with an exogenous photosensitizer, a method that is sometimes referred to as “photochemotherapy” or “photodynamic therapy”. 14 Treatment efficiency in the study was evaluated using bioluminescence. 17
In our study, microbiological analysis exhibited a linear decrease in bacteria as dosages increased, with only three animals in Group 6, with irradiation of 180 secs (18 J at 22.93 J/cm2), testing positive for MRSA. Histopathological analysis revealed tibial infection to be partly suppressed in Group 4, with irradiation of 60 secs (6 J at 7.64 J/cm2), an optimal level of healing being obtained in Group 6. Whereas disease severity scores were at mid-level in Group 3 (debridement, no laser treatment), they decreased to <1 in Group 6. Moreover, the fact that SS was <4 in all three laser groups indicates that the total amount of light applied was sufficient, even at exposures of 60 secs (6 J at 7.64 J/cm2) (Table 1).
Conclusion
Our findings show that daily laser irradiation with an 808 nm, 100 mW continuous wave diode laser and a beam spot size of 0.7854 cm2 (irradiance = 127.3 mW/cm2) for 5 consecutive days immediately following debridement surgery is effective in treating experimental chronic osteomyelitis in a rat model. Efficacy was demonstrated with irradiation durations of 60 secs (6 J at 7.64 J/cm2) and 120 secs (12 J at 15.29 J/cm2), the greatest effect being observed with an irradiation duration of 180 secs (18 J at 22.93 J/cm2). In the light of these results, laser phototherapy within these parameters may be considered a promising adjunct and/or alternative to pharmacological agents in the treatment of chronic osteomyelitis, and further pre-clinical studies are warranted.
Footnotes
Acknowledgments
This study was supported by the Atatürk University Scientific Research Projects Fund (Project number: 2008/192). We thank Dr. Armağan Hayırlı and Dr. Ömer Cevdet Bilgin for their assistance with the statistical analysis.
Author Disclosure Statement
No conflicting financial interests exist.