
Abstract
Introduction
Methods
Clinical history
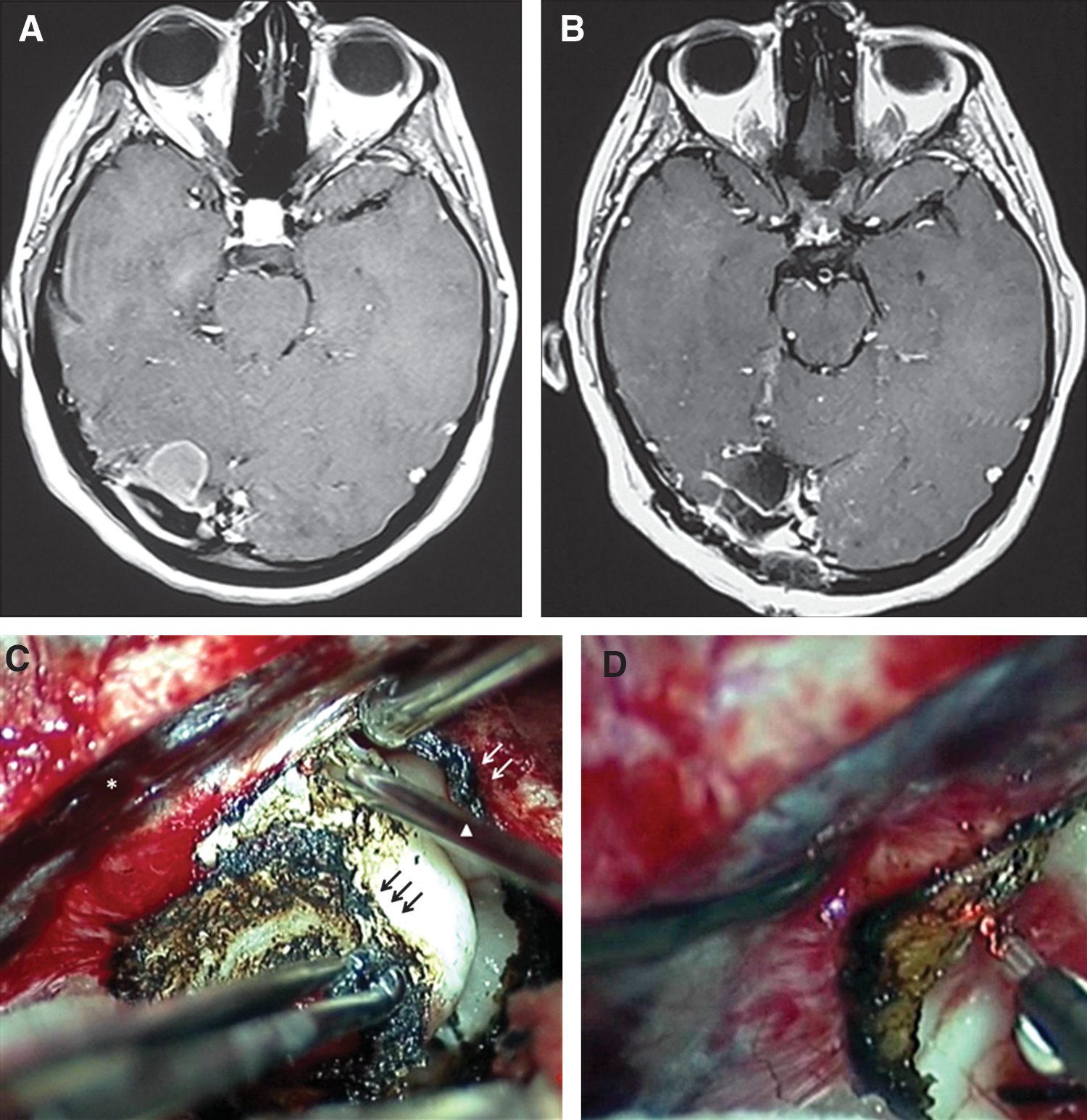
A 31-year-old woman presented with a lypotimia in 2005. Magnetic resonance imaging (MRI) of the brain was performed at that time, and a small right tentorial lesion near the right transverse sinus was found incidentally. The mass enhanced diffusely following intravenous gadolinium injection, and the dural tail sign was positive, suggesting the diagnosis of tentorial meningioma. The neurological examination was normal, and the patient did not have a history of any systemic disease or trauma. Her blood biochemistry was within normal limits. Surgery was deferred because of the small dimensions of the lesion, and the patient was monitored with MRI exams once a year.
Four years later, the patient's most recent MRI showed that the lesion had grown 3 mm in one year (Fig. 1A). Given the young age of the patient and the growth of the tumor compared to prior MRIs, surgical intervention was planned.
Surgical technique and laser settings
A suboccipital supratentorial surgical approach was performed with a small craniotomy of about 4 cm. The right occipital lobe was gently retracted, and a well-encapsulated tumor mass implanted on the tentorium was exposed. The macroscopic appearance of the tumor suggested a meningioma. The tumor was excised with the aid of a 2-μm continuous-wave thulium laser (Revolix® Laser JR 15 W). Energy was administered with a 0.73 mm diameter microfiber (Percufib®) inserted in a curved hand piece (Surgilas®) designed for maneuvers under microscope magnification. All of the tentorium tissue surrounding the lesion was cauterized and cut with the 2-μm thulium laser in continuous mode at 8 W (Fig. 1C). No injuries to the underlying cerebellar parenchyma were observed during the tentorial resection. The implant was cauterized near the transverse sinus with the laser in continuous mode at 6 W (Fig. 1D). No injuries of the sinus were noted. The energy administered was 3160 J during debulking and 1433 J during cauterization of the meningioma implant. Complete removal with coagulation of the dural attachment near the transverse sinus was achieved at the macroscopic level.
Histological examination confirmed the diagnosis of meningioma (grade I WHO). The postoperative course was uneventful, and the patient was discharged 5 days post-intervention. Postsurgical MRI 1 month after treatment showed no residual mass (Fig. 1B). Six months after surgery, the neurological examination was normal, and a control MRI showed no signs of recurrence and patency of the transverse sinus.
Discussion
As Ryan et al. have noted in their review, 9 the use of lasers in neurosurgery was first tested in the 1960s, and the first resection of a glioblastoma using a CO2 laser was performed in 1966 by Stellar and colleagues. 10 After that, many laser prototypes, including argon and Nd:YAG lasers, were developed and used widely in neurosurgery, but their use remained anecdotal. The systematic use of lasers as part of neurosurgical instrumentation started in the 1970s and 1980s, when the first studies using lasers on animals 11 –13 and in the treatment of human pathologies (mainly intracranial tumors 14 –17 ) were reported. Selected reports also used lasers in treatment of intracranial aneurysms, AVMs, spinal cord tumors, fenestration of arachnoid cysts, and cerebrovascular bypass. 3 –5 Enthusiasm for the use of lasers in neurosurgery waned during the 1990s, when authoritative neurosurgeons claimed the importance of microdissection and bipolar cautery for treatment of intracranial masses. 18 Additionally, some ergonomic problems of lasers, such their footprint in the operative room and the use of nonflexible fibers, remained unresolved. 9 However, some surgeons continued to use lasers in large series. 19,20 Recently, the development of flexible fibers and less bulky devices have rekindled interest in the use of lasers during neurosurgery for microsurgical and endoscopic procedures. 20,21
Thulium lasers have been used widely in urological surgery, mainly for bladder neck incisions 6 and vaporesection of the prostate, 7,8 where they have been demonstrated as safe and minimally invasive. Our survey of the English literature (Pubmed) showed just one report about the use of thulium lasers in neurosurgery. 22 Our group recently initiated occasional use of a thulium laser (Revolix Jr®), along with the cavitron ultrasonic surgical aspirator (CUSA) and bipolar forceps, for the resection of benign intracranial masses, such as meningiomas and neurinomas. The laser has mainly been applied for debulking and shrinking of the lesions, coagulation and vaporization of the margins and the basal implant. Working in an aqueous medium, the laser's effect on the tissue is restricted to less than 2 mm in front of the tip of the fiber. Any tissue further than 2 mm from the fiber is shielded by the medium and is unaffected by the thulium laser. This property of the laser eliminates the risk of unintentional tissue damage during microsurgery.
In the present case, although complete instrumentation (including the CUSA and bipolar forceps) was prepared in the operative room, the thulium laser was almost exclusively used for both debulking of the tumor and resection of the basal implant. The CUSA allows for optimal tumor debulking but does not coagulate tumor vessels; when performing surgery with the CUSA, it is necessary to stop frequently and use bipolar forceps. The thulium laser is capable of vaporizing and coagulating at the same time, keeping the surgical field clear of blood. As other authors have noted, the thulium laser works at a wavelength of 2013 nm, which is close to the absorption peak of water. 7,22 The depth of tissue penetration is 0.8 mm, halfway between a Nd:YAG laser (20 mm), which can produce deep lesions in tissue free of hemoglobin, and a CO2 laser (0.05 mm), which only superficially penetrates tissue. This feature of the thulium laser permits safe surgical resection. Moreover, unlike other prototypes, the thulium laser is conveyed through a flexible optical fiber, which minimizes the dispersion of the laser beam. Settings of the laser can be changed during surgery and adapted for specific maneuvers (e.g., debulking near important vascular/nervous structures); the laser can be adjusted from 1 to 15 W.
In our case, we performed coagulation and vaporization of the visible surface of the tumor and the immediately surrounding tentorial tissue. During this procedure, a small fenestration was generated on the tentorium and the underlying cerebellar tissue was seen. In the majority of patients, the human tentorium consists of two layers that contain a venous plexus that bleeds easily and must be cauterized during surgical procedures requiring its opening. This step can increase the duration of surgery due to intraoperative bleeding. 23 In the present case, resection of the tentorial basal implant was performed with a RevoLix laser, which allows simultaneous cutting and coagulation of the tentorial surface, minimizing intraoperative bleeding and shortening the time of resection, a procedure that is longer and more demanding with traditional methods. The gross total resection of the mass with complete coagulation of the margins was achieved in about 30 min. No surgical damage to the underlying cerebellar parenchyma was noted. Regarding laser settings, the energy administered was 3160 J during debulking and 1433 J during cauterization of the meningioma implant. The meningioma and tentorium tissues were cauterized and cut with the 2-μm thulium laser in continuous mode at 8 W (Fig. 1C); cauterization of the implant near the transverse sinus was performed with the laser in continuous mode at 6 W (Fig. 1D). Using these settings, no injuries to the cerebellum or the transverse sinus were noted. A 0.73-mm diameter flexible fiber, inserted into a curved hand piece (Surgilas®) that is useful for maneuvers under microscopic magnification, permitted performance of all procedures without any hindrance to the surgeon.
Although the use of the laser in the present case displayed many advantages, some details must be provided. First, by using the settings described, bleeding from submillimeter vessels can be perfectly controlled, but it is intuitive that bleeding from medium or greater vessels (>1 mm in diameter) cannot be controlled without other instrumentation. Moreover, radiological and anatomical features of the present case made the resection possible using the laser technique alone. Although debulking, shrinking, and coagulation of the basal implant of larger tumors can also be eased by the use of laser techniques, the importance of the CUSA, bipolar forceps, and microdissection techniques cannot be ignored.
Conclusion
Two-micron thulium lasers can be used in neurosurgery for surgical removal of benign intracranial tumors under microscopic magnification. These lasers are a useful tool in addition to, but not as a substitute for, traditional neurosurgical instruments. However, additional studies must be carried out to define fully the role of thulium lasers during neurosurgical procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.