
Abstract
Introduction
Bond strength to enamel can be reestablished to standard values up to 1–3 weeks after bleaching. An elapse time is needed for oxygen release. 5,8,9 Therefore, several authors have proposed methods to reverse this side effect and enable replacement of composite restorations as soon as possible. 2,3,5,6,8
Because it has a wavelength of 2.94 μm, the use of Er:YAG laser may promote chemical and/or morphological alterations on enamel surface. 10,11,12 Its wavelength coincides with the water absorption spectrum and results in thermal energy and surface temperature rise. 13 It has been reported that Er:YAG irradiation with 26.9 J/cm2 decreases enamel solubility without severe morphological enamel alteration. 14
Er:YAG laser at a low-energy setting can chemically and structurally change enamel surface. 12 Carbonate is already lost beginning at a temperature of 100°C 15 with complete removal near the melting point. 12 Laser irradiation raises the temperature to 150°C at a fluence of 4 J/cm2 and to ∼300–400°C near the ablation process. 12
An effective adhesion to enamel irradiated by Er:YAG laser depends upon the structural alteration induced by the laser. Laser etching produces rough surfaces similar to acid etching. However, Gurgan et al. reported decreased shear bond strengths after enamel etching of bleached teeth with Er,Cr:YSGG laser. 16
Hydrogen peroxide and free oxygen are highly reactive and an increase in temperature produced by enamel laser irradiation in subablative parameter (4 J/cm2) could possibly release them. 17 In this case, Er:YAG laser irradiation could possibly accelerate the removal of residual oxygen from bleached enamel surfaces, decreasing the elapsed time following bleaching to performing enamel adhesive restorations.
As treatment with Er:YAG laser after enamel bleaching prior to adhesive restorative procedures has not been evaluated so far, the aim of this study was to assess the effects of two Er:YAG laser irradiation parameters on the microtensile bond strength to bleached enamel. The tested null hypothesis was that bond strengths of resin composite to bleached and unbleached enamel surfaces is not affected by Er:YAG laser irradiation.
Material and Methods
Sixty bovine incisors stored in 0.1% thymol solution at 4°C were used. Blocks with 7 × 3 × 3 mm3 were sectioned from the buccal surface with double-faced diamond disks (no. 7020; KG Sorensen, Barueri, São Paulo, Brazil) used at low speed (Kavo, Joinville, São Carlos, Brazil) and under water irrigation. Samples were randomly distributed into six experimental groups according to the bleaching and laser treatment performed: G1 - bleaching and Er:YAG laser irradiation with 25.52 J/cm2(LA); G2 - bleaching and Er:YAG laser irradiation with 4.42 J/cm2 (LB); G3 - bleaching; G4 - Er:YAG laser irradiation with 25.52 J/cm2; G5 -Er:YAG laser irradiation with 4.42 J/cm2; G6 - control, no treatment.
Bleaching procedures
Bleaching was performed for 21 days in groups G1 to G3 using a home bleaching protocol. An individual tray for each block was made from a 0.4-mm-thick ethyl vinyl acetate polymer (EVA, Bio Art Equipamentos Odontológicos Ltda., São Carlos, Brazil) in a vacuum forming machine. A 16% carbamide peroxide gel (0.04 ml) (Whiteness Perfect 16%, FGM, Joinville, Brazil) was applied over the blocks, which were covered by the individual custom tray, and left undisturbed for 6 h/day. During the bleaching regimen, blocks were stored in 14 ml of artificial saliva at 37°C that was changed daily. The artificial saliva contained calcium and phosphate in a degree of saturation known to mimic the remineralizing properties of natural saliva (50 mmol/l KCl, 1.5 mmol/l Ca, 0.9mmol/l PO4, 20 mmol/l tri-hydroxymethil-aminomethan, pH 7.0). 18 –22
In an attempt to simulate cavity preparation procedures and obtain flat standardized surfaces for the microtensile bond strength test, enamel surfaces were abraded with 600-grit silicon carbide paper for 10 sec by a single operator calibrated from a pilot study (Carburundum Abrasivos Ltda., Vinhedo, Brazil) using a polishing machine (PL02 RB LAB Com. Técnica Ltda., São Paulo, Brazil).
Laser irradiation
The Er:YAG laser (KaVo KEY Laser II, KaVo, Biberach, Germany), which presents a wavelength of 2.94 μm, and pulsed duration of 250–400 μs, was used to irradiate the enamel surfaces with the handpiece no. 2055, fiber 50/10 with beam diameter of 0.47 mm, input energy of 100 mJ, and repetition rate fixed at 2 Hz with a transmitting factor of 0.54 without refrigeration in all specimens. The output energy was 82 mJ. It was measured with a power meter (Coherent, Newport, Rhode Island). The externally supplied water has a significant influence on the effectiveness of the ablation process. Without an external water spray, the efficiency of ablation process is decreased using the Er:YAG laser on dental enamel. 23
Blocks of groups G1 and G4 were irradiated in “contact mode” with 25.52 J/cm2. Enamel surface was irradiated uniformly for 40 sec by a single operator calibrated from a pilot study. The operator moved the laser handpiece in a sweeping fashion by hand in a grid pattern.
In G2 and G5 the handpiece was positioned 3 mm away from the target to decrease the energy density at the surface, and it was irradiated in “non-contact mode” resulting in an irradiation energy density of 4.42 J/cm2. Energy density was determined from five measurements of the laser beam diameter at non-contact mode in a carbon paper. The spot was measured with a digital caliper. The calculated spot diameter was 0.113 cm. The standardization of the distance was achieved with an endodontic K-file fixed to the laser handpiece.
Microtensile bond strength test
After surface treatment, a two-step etch-and-rinse adhesive system (Adper Single Bond 2, 3M/ESPE, Irvine, CA) was used according to manufacturer's instructions. Table 1, lists composition, lot number, and application instructions of the selected materials. Enamel surfaces were etched with 37% phosphoric acid for 15 sec, rinsed with water, and dried with an air stream. After application of the adhesive system with disposable microbrush tips, excess solvent was evaporated with a gentle air stream for 5 sec, and the adhesive was light-cured for 10 sec. Afterwards,, a 4-mm-high composite buildup was made with a micro-hybrid resin composite (Filtek Z250, A2, 3M/ESPE ). Light activation of adhesive and resin composite was performed with a quartz-tungsten halogen lamp with a 700 mW/cm2 output (Optilux, Demetron/Kerr, Danbury, CT). Restored specimens were placed in relative humidity at 37°C for 24 h.
bis-GMA; bisphenol glycidyl methacrylate; bis-EMA; bisphenol A polyethylene glycol diether dimethacrylate; UDMA; urethane dimethacrylate; DMA; dimethacrylates; HEMA; 2-hydroxyethyl methacrylate.
Specimens were serially sectioned into 1-mm-thick slabs using a diamond saw (IsoMet 1000; Buehler Ltd, Lake Bluff, IL) under water cooling. The adhesive interface was trimmed at the interface to an hourglass shape with a cross-sectional bonded area of ∼1 mm2, which was tested in tension in an universal testing machine (EZ Test, Shimadzu, Kyoto, Japan) operated at a crosshead speed of 1 mm/min. Specimens were attached to a microtensile apparatus, using a cyanoacrylate adhesive (Loctite Super Bond Gel; Henkel, Düsseldorf, Germany). Dimensions of each side of the debonded specimen were measured using a digital micrometer (Mitutoyo Co., Tokyo, Japan) and the μTBS values were expressed in MPa. Five slabs were tested for each enamel block, and the mean bond strength value was considered. Bond strength values were statistically analyzed by two-way ANOVA at the 95% confidence level.
Failure mode was observed in a stereomicroscope 24 at a 100 × magnification (PanTec, Panambra Ind. e Técnica SA, São Paulo, Brazil) and scored according to one of three failure modes: 25 cohesive failure in enamel (CE), adhesive failure between enamel and composite (AD) and cohesive failure in composite resin (CR). Instead of classifying failure as mixed, the area percentage of each type of failure in each fractured specimen was recorded.
Scanning electron microscopy (SEM) analysis of enamel surface
One treated block of each group was used for SEM analysis and one fractured specimen representative of each group was selected during failure-mode analysis. For enamel surface observation, specimens were cleaned in an ultrasonic bath for 10 min and fixed in Karnovsky solution for 1 h. Afterwards they were rinsed with distilled water and then dehydrated in a graded series of alcohol solutions [70, 90, and (3x) 100%] for 10 min at each concentration. Specimens were sputter-coated with gold and examined with a scanning electron microscope (FEI; Quanta 600F, Eindhoven, The Nederland, NE). Photographs were taken at 200, 500, and 2,000x magnifications (Figs. 1 –6).
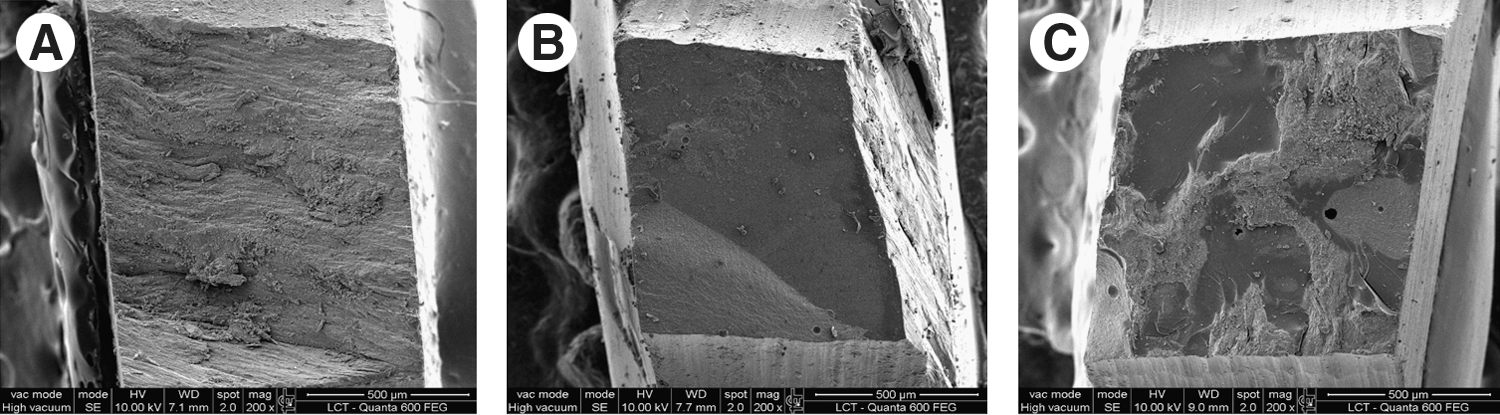
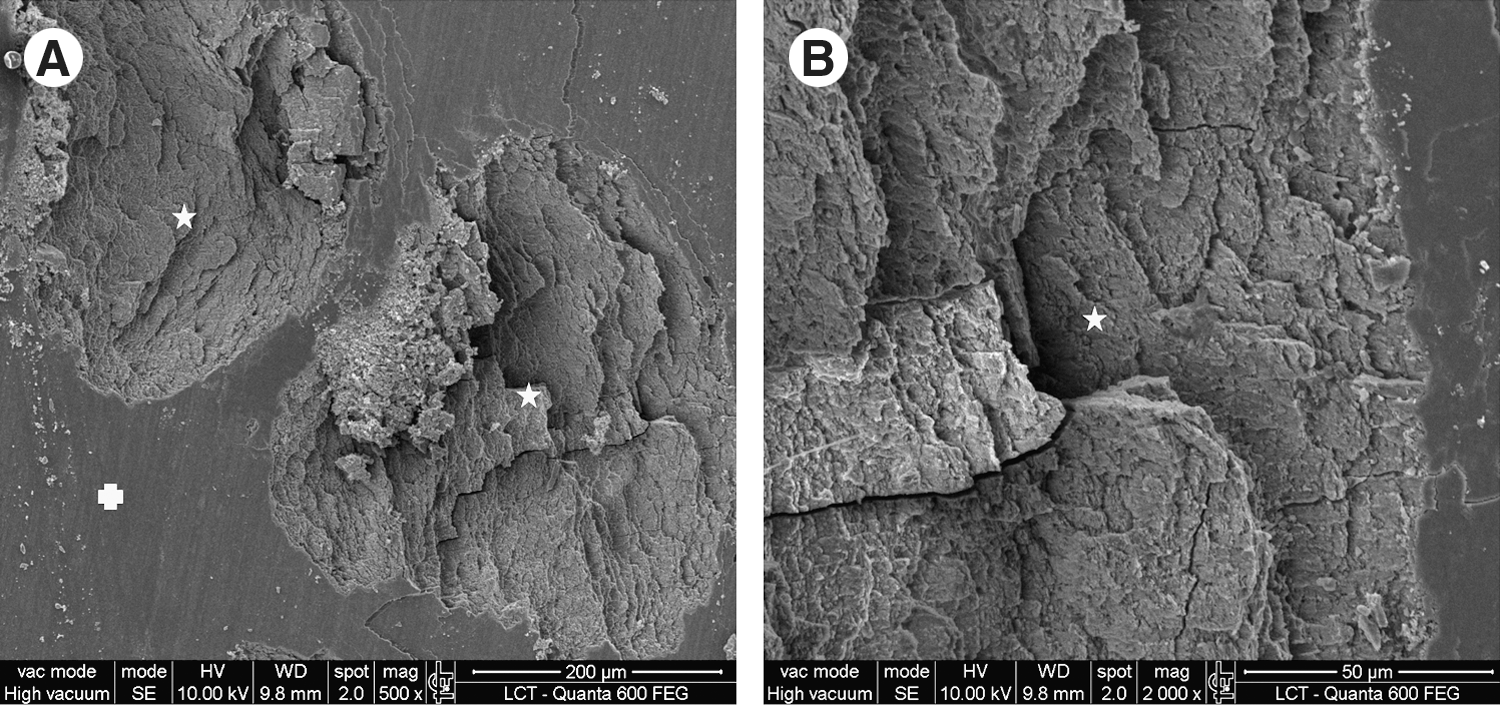
Scanning electron micrographs (SEMs) of the three representative failure types (

Scanning electron micrographs (SEMs) of enamel surface of bleached teeth irradiated in contact mode with 25.52 J/cm2 (Group 1). (

Scanning electron micrographs (SEMs) of bleached enamel irradiated in non-contact mode with 4.42 J/cm2 (Group 2). (

Scanning electron micrographs (SEMs) of the surface of bleached and prepared enamel (Group 3) demonstrate (
Scanning electron micrographs (SEMs) of unbleached enamel irradiated with 25.52 J/cm2 (Group 4). (

Scanning electron micrographs (SEMs) of the unbleached and non-irradiated enamel (Group 6). (
Results
Microtensile bond strength test
Table 2 presents mean μTBS values of each experimental group, standard deviation, and pre-test failures. No statistically significant differences were observed for the factor “bleaching” (p > 0.08), for the factor “laser treatment” (p > 0.20), or for the interaction between factors (p = 0.13). The distribution of failure modes among groups is shown in Fig. 7.
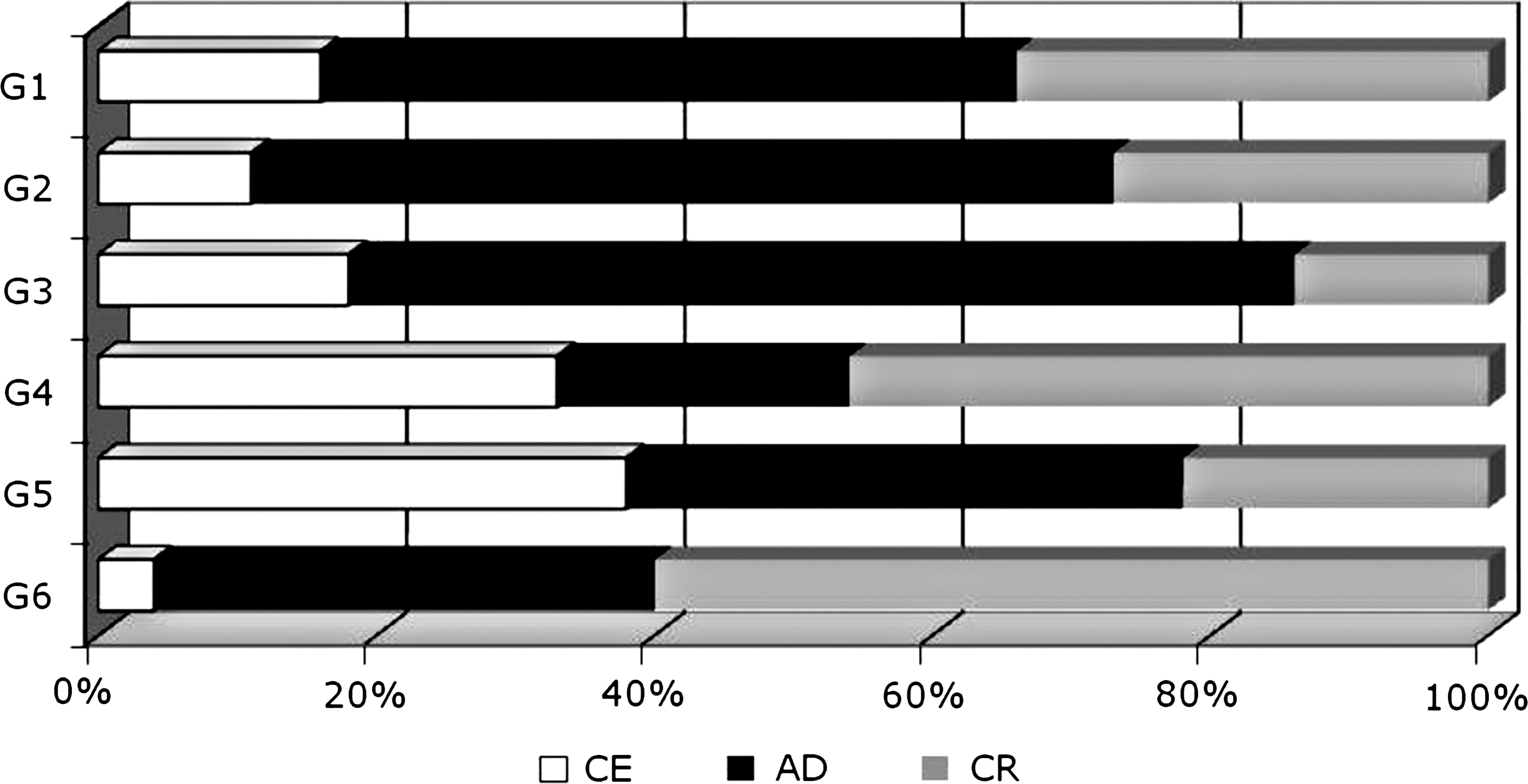
Distribution of failure modes within groups. CE, cohesive failure in enamel; AD, adhesive failure between enamel and adhesive; CR, cohesive failure in resin composite.
Means followed by the same capital letters in the column indicate no statistical difference (p > 0.05), n = number of samples.
The predominant fracture in the control group G6 (60%) and G4 (46%) was cohesive in composite resin. However, G6 and G4 presented 4% and 35% of cohesive failures in enamel, respectively. In the other groups, the predominant fracture mode was adhesive between enamel and resin (G1, 50%; G2, 62%; G3, 68%; and G5, 40%). On the other hand, the least predominant fracture mode for G1 (16%) and G2 (11%) was cohesive in enamel, and G3 presented cohesive failures in composite resin as the least predominant in 14%.
SEM evaluation
Representative SEMs of each failure mode are presented in Fig. 1. The morphological features of each experimental group surface are presented in Figs. 2 –6. Contact Er:YAG laser irradiation promoted ablation of enamel surface for bleached (Fig. 2) and unbleached teeth (Fig. 5). Non-contact Er:YAG laser irradiation prior to adhesive procedure promoted no ablation of bleached and unbleached enamel surfaces (Fig. 3). There were no morphological alterations on enamel surface of bleached and flattened teeth (Fig. 4) compared with control, which was covered by smear layer (Fig. 6).
Discussion
Vital dental bleaching is a conservative and safe procedure to treat discolored teeth. 22,26 The clinical use of 10% carbamide peroxide has been described by Haywood and Heymann and it is widely used in modern dentistry. 27 This agent is effective for bleaching, 21 and the use of peroxides with higher concentration has increased. 16,28 Residual oxygen from bleaching agents can reduce bond strength of composite resin restorations to enamel and dentin. 6,8,20,21,29,30
Our study demonstrated no significant differences among groups. Therefore, the null hypothesis was not rejected. The absence of differences in μTBS values may be the result of the selected study design model, which simulated 21 days of bleaching treatment. According to a review of bleaching studies, “in vitro” studies are performed from 14 days until 42 days . 22 The present study used the time interval of 21 days at-home bleaching procedure. It can be speculated that a 42-day regimen could have left residual peroxide in an amount that could have impaired μTBS values.
Also, in the present study model, bleaching treatment was performed on enamel surface and bonding procedures were performed on the inner enamel, which was abraded after bleaching procedures. Therefore, the resin-enamel bond strength test was performed not on the uncut enamel bleached surface, but on the cut enamel subsurface, as would be expected to occur in the clinical situation.
Because of the low molecular weight of peroxides, penetration of the bleaching agent into the inner enamel was expected. 31 Depending upon the clinical conditions, there is evidence that different concentrations of peroxide can reach the pulp chamber. 31,32 After the 21-day bleaching regimen, enamel was worn in an attempt to simulate a cavity preparation covered with smear layer (Fig. 4). Therefore, the accumulation of residual peroxide and free oxygen in the area abraded for the bond strength test could be smaller than at the external surface, directly exposed to the bleaching agent. That could possibly explain why no significant differences were observed among μTBS values.
However, the differences observed in the failure mode analysis suggest that the bleaching procedures might have presented an effect on the resin-enamel interfaces, even with no differences in μTBS values. Residual oxygen from bleaching agents impairs bond strength of composite resin restorations to enamel 6,20,21,29,30 and higher adhesive failures in the bleached group (G3) than in the control group (G6) were observed. Bleached group (G3) presented 68% of adhesive failures and control group (G6) presented 36% of adhesive failures. Adhesive failure can represent a weak link between composite and enamel surface, probably because of polymerization inhibition of the adhesive system by the residual oxygen from the bleaching procedure.
The group bleached and treated with Er:YAG laser in contact mode (G1) showed no difference in μTBS values compared with the group treated with non-contact mode (G2), and both groups presented a predominant adhesive failure mode compared to the group bleached and not irradiated (G3). After Er:YAG irradiation, the laser energy must have been absorbed by enamel and changed into thermal energy. It has been reported that Er:YAG at a fluence of 4 J/cm2 produces 150°C of enamel temperature increase. 12 This thermal energy may change enamel chemical composition even in subablative parameter (4 J/cm2) or by temperature diffusion in ablative energy densities 33 that reach ∼300–400°C. 12,31 Even though the μTBS was not significantly different among bleached and control groups; a high percentage of cohesive failures in enamel was observed in Er:YAG laser-irradiated groups, probably because of the thermal effect of Er:YAG irradiation.
SEM revealed that the contact mode irradiation with 25.52 J/cm2 led to total removal of the smear layer, creating a non-homogeneous surface with evidence of ablation with cracks and melted enamel (Fig. 2) and is in accordance with Bevilácqua et al.'s report that enamel morphological alterations with Er:YAG laser with 25.47 J/cm2. 11 The Er:YAG laser irradiation with 4.42 J/cm2, promoted no ablation or melting on enamel surface (Fig. 3).
In contrast to groups irradiated in contact mode, bleached and unbleached groups (G1 and G4), presented different failure patterns. The bleached group showed less cohesive enamel failure (16%) than unbleached group, which showed 33% of cohesive failures in enamel. This is probably because of subsuperficial structural alterations promoted by Er:YAG laser irradiation. Structural defects on enamel can be responsible for the occurrence of cohesive failures in enamel, because Figs. 2 and 5 showed morphological alterations with evidence of ablation. It is also important to note that group 4 recorded the largest number of pre-test failures (36%), probably because of the structural defects after Er:YAG laser irradiation with 25.52 J/cm2. For this reason, Er:YAG laser irradiation with 25.52 J/cm2 should not be recommended.
Also, Chuang et al. reported decreased microtensile bond strength values after bleaching with 10% carbamide peroxide 8 h/day for 14 days. 1 However, in that study, the adhesive procedure was performed without flattening the enamel surface. 1 Direct adhesion on bleached enamel surface is a protocol that would represent a clinical situation of orthodontic bracket bonding or distemas closure procedures, which do not require cavity preparation. Therefore, our study protocol of enamel surface abrasion tried to simulate cavity preparation with dental burs during composite restoration replacement. In the present study, the purpose of flattening the enamel was to create a clinical condition of restoration replacement, and the removal of superficial enamel was found to be favorable to enamel bond strength. In the same way, Gurgan et al. reported decreased shear bond strength of a self-etching adhesive system applied to unabraded enamel after bleaching with 16% carbamide peroxide, compared with unbleached enamel and Er,Cr:YSGG laser treatment. 16
Bleaching agents lead to changes in the enamel matrix as a result of an unspecific oxidation of enamel. It can result in a clinical reduction of enamel microhardness. 34 Studies simulating the in-office bleaching treatment with aplication of hydrogen peroxide based materials within the pulp chamber did not find alterations in enamel bond strength or increase in microleakage agreeing with the present results. 35,36 There are no comparable studies analyzing the influence of Er:YAG laser irradiation in subablative energy density on the μTBS to enamel after dental bleaching.
In summary, no significant differences were observed in μTBS values to enamel after bleaching treatment. Surface treatment with Er:YAG laser irradiation in contact and non-contact mode had no effect on μTBS to bleached and unbleached enamel. Contact mode laser irradiation promoted ablation of enamel surface observed under SEM.
Conclusions
Adhesive procedures can be performed in margins of prepared cavities soon after vital dental bleaching, with no reduction of microtensile bond strength, as long as enamel is abraded and subsurface enamel is exposed. Er:YAG laser irradiation with 25.52 J/cm2 prior to adhesive procedures had no influence on μTBS and promoted ablation of enamel surface and could not be recommended as morphological alterations were observed. On the other hand, Er:YAG laser irradiation with 4.42 J/cm2 did not promote ablation and had no effect on adhesion to enamel.
Footnotes
Acknowledgments
The authors thank Ms. Mariane Brumatti (LCT POLI-USP- Technology Characterization Laboratory, University of São Paulo, Brazil) for technical support with electron microscopy. This work was supported by FAPESP (São Paulo Research Foundation) Grant FAPESP no. 2007/06083-4 and Grant FAPESP no. 2004/01175-4.
Author Disclosure Statement
The authors have no interest in any of the companies or products mentioned in this article.