
Abstract
Introduction
Cryosurgical treatment uses freezing temperatures to achieve specific effects on tissues. 14 The technique of cryosurgical treatment causes rapid cooling, slow thawing, and the repetition of the freezing process to maximize tissue destruction. 14 –16 Cryosurgical treatment can be recommended for high-risk surgical patients, such as patients with a pacemaker, the elderly, and those with a coagulopathies, 15 and tends to be the method of choice in cases of multiple and large lesions, areas of difficult surgical access, and areas where aesthetics are deemed important. 15 Prior studies have demonstrated the success of cryosurgical treatment in treating OL. 6,7,10 –13 In addition, mild to moderate post-surgical pain has commonly been reported by patients after cryosurgical treatment. 9,11 –13
The analgesic use of nonsteroidal anti-inflammatory drugs is often recommended after oral surgery to abolish postoperative pain, but some of these drugs may cause side effects, such as gastrointestinal irritation, systemic bleeding, and allergic reactions. 17 These observations justify efforts to find a method of postoperative pain control that does not produce side effects. In this setting, the use of low-level laser therapy (LLLT) may be promising. 18 Several studies have demonstrated the beneficial effects of LLLT in the reduction of post-surgical pain. 18 –20 LLLT has been recommended for pain relief due to its well-known biological effects found in the interaction between laser energy and injured tissues. 20,21 The possible mechanisms include the acceleration of the anti-inflammatory and analgesic effects, as well as the process of repair. 19
Considering the efficiency of cryosurgical treatment of OL, one of the most common side effects of which is postoperative pain, together with the anti-inflammatory and analgesic properties that LLLT bring to this picture, the goal of this preliminary study was to investigate the ability of LLLT to alleviate pain caused by the cryosurgical treatment of OL.
Material and Methods
Patients
This study was approved by the Ethics Committee of Universidade Federal de Minas Gerais n° 36/08, and informed written consent was obtained from all patients. Eighteen patients were recruited from the Oral Medicine Clinic, School of Dentistry, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil, from October 2007 to March 2009. Diagnosis of OL was in accordance with that reported by Warnakulasuriya et al. 1 Patients' age, gender, and smoking status, as well as the location, size, and microscopic features of OL, were recorded. No patient presented any local or systemic diseases that made them ineligible for treatment with cryosurgical treatment. The selection of the patients included: patients who presented multiple and/or large OL (>20 mm), patients with areas of difficult surgical access, cases in which aesthetics were important, and high-risk surgical patients. Patients currently using anti-inflammatory or analgesic medications were excluded from this study. Patients were randomly assigned to one of two groups: non-LLLT and LLLT. In the non-LLLT group (n = 10), the patients were submitted to cryosurgical treatment, whereas in the LLLT group (n = 8), they were submitted to cryosurgical treatment associated with LLLT. Cryosurgical treatment was performed by one calibrated trained medical oral examiner (ASR). Another double-blinded medical oral examiner performed the LLLT and took photographs of the OL (RAM). Clinical evaluation during each visit was performed by an ASR and a TAS, who were also blinded to the patient's status.
Cryosurgical treatment technique
Following local anesthesia (Alphacaine 100–Lidocaine 2% plus epinephrine 1:100.000, DFL Indústria e Comércio S.A., Rio de Janeiro, Brazil), cryosurgical treatment was performed by means of an application of liquid nitrogen using a CryAc® apparatus (Brymill Cryogenics Systems, Ellington, CT). This method was carried out using either a spray or a closed system, depending on the surface and surgical access. The time of application was 10 s for the spray system 22 and 60 s for the closed system. 12 OL were delimited within a 10 mm2 area and exposed to two consecutive, freeze-thaw cycles, beginning at the center of the lesion and moving out to the borders until the entire area appeared white. After the ice ball produced during freezing had completely thawed, the next freezing was performed. Thawing occurred spontaneously after 30–60 s. Lesions with a diameter of larger than 10 mm were treated in two or more sessions. The second treatment was performed 1 month after the first treatment. Patients were examined at 1, 2, and 4 weeks, and 6 months after cryosurgical treatment and were subsequently recalled every 6 months thereafter.
Laser application
Laser irradiation of patients in the LLLT group was performed using a 50 mW 660 nm continuous wave Gallium Aluminum Arsenide (GaAlAs) laser (‘Whitening Lase II’, DMC LTDA, Sao Carlos, Brazil). Energy was delivered via optical fiber to the treatment site, with a resulting spot size at the tissue surface of 0.0286 cm2 (irradiance = 1.75 W/cm2). Three points within an area of 1 cm2 around the cryosurgical site were irradiated in contact mode for 28 s per point (1.4 J at 49 J/cm2 per point). Irradiation was carried out immediately following cryosurgical treatment, and again at 48 and 72 h postcryosurgical treatment. Both patients and medical oral examiner used specific protective glasses during the treatment.
Measure of pain
The pain assessment instrument used in this study was a self-reported numerical rating scale (NRS). 24 Self-reporting of pain involves asking the patients to rate subjectively the intensity of the pain they feel, from 0 to 10 points (an 11 point scale), with the understanding that 0 represents no pain and 10 represents the extreme of pain intensity (unbearable pain). The patients were verbally asked about the pain 1 week after the first session of cryosurgical treatment performed by an ASR. Regarding the edema, patients were asked, in terms that could be easily understood, whether the edema was present or not.
Postoperative care
Patients were instructed regarding oral hygiene; care with hot, hard, and acid foods during the healing period; and the observance of pain and edemas associated with the treatment.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL) version 15.0 for Windows was used to perform the statistical analysis. A descriptive analysis of each variable was carried out. The association between the different qualitative variables was established using the Chi-Square and Fisher's exact tests. The relationship between the treated groups and pain parameter was assessed for statistical significance by the Mann–Whitney test. A p value of < 0.05 was considered statistically significant.
Results
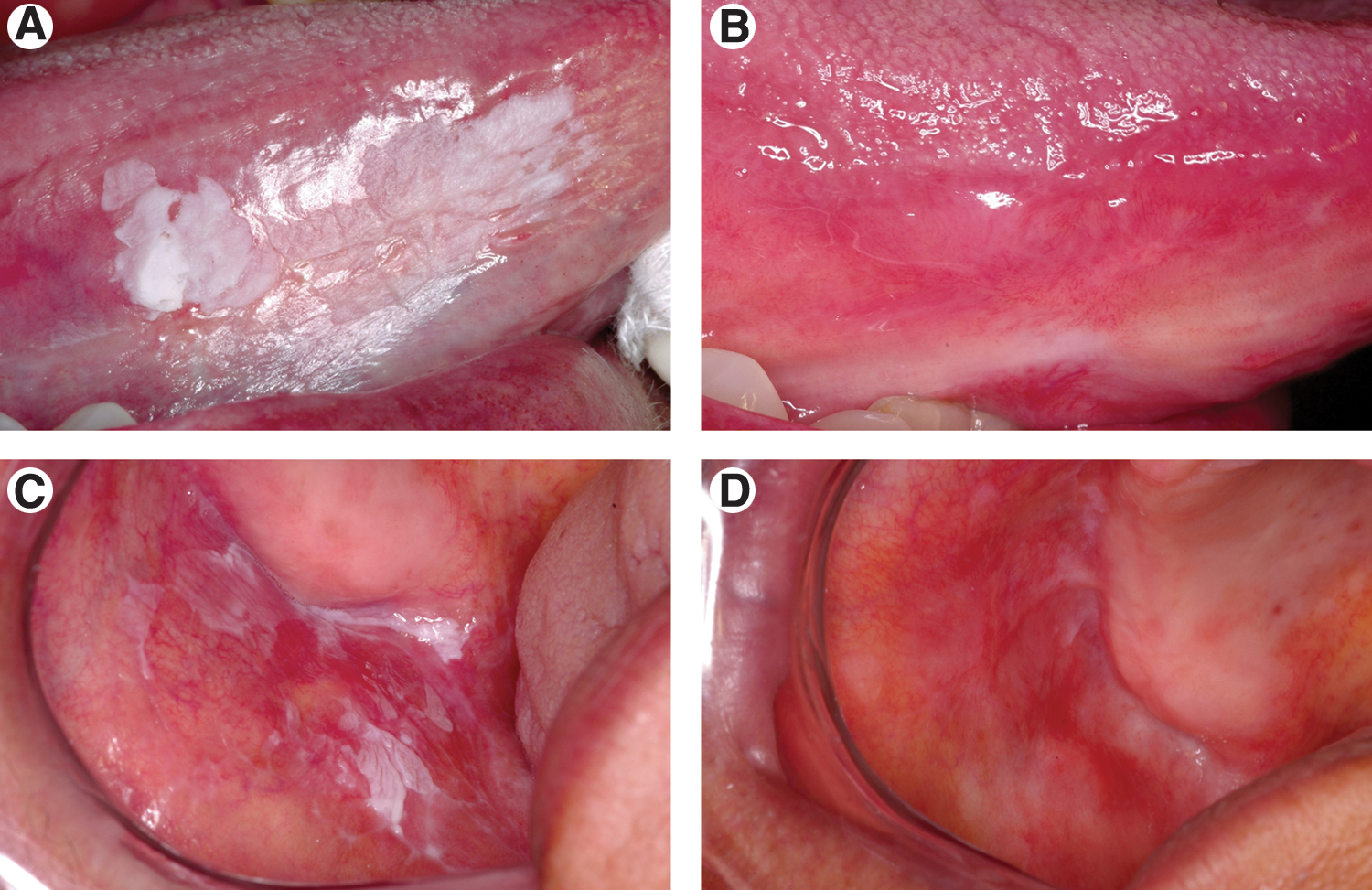
The patients included 15 women and 3 men, ranging from 35 to 85 years of age (mean of 64.67 ± 11.31). Four patients were smokers (Table 1). The clinical features of OL appeared as asymptomatic white plaques of the homogenous type with uniform, flat, thin, surfaces containing many fine cracks or fissures (Figs. 1A and C). The gingiva (n = 6) was the most common site, followed by the buccal mucosa (n = 5), the tongue (n = 5), the alveolar mucosa (n = 1), and the hard palate (n = 1). The area containing OL lesions varied from 5 to 50 mm (mean of 23.11). Histopathology demonstrated that 12 OL contained epithelial dysplasia (7 in the non-LLLT group and 5 in the LLLT group): 7 contained mild epithelial dysplasia (5 in the non-LLLT group and 2 in the LLLT group), and 5 contained moderate epithelial dysplasia (2 in the non-LLLT group and 3 in the LLLT group). Six patients presented no epithelial dysplasia (3 in the non-LLLT group and 3 in the LLLT group) (Table 1). There were no significant differences in the distribution of the groups when considering gender, age, presence/absence of epithelial dysplasia, smoking status, location, and size of OL (chi-square tests, p > 0.05).
Clinical aspects of oral leukoplakia before cryosurgery
H, hyperkeratosis; M, mild epithelial dysplasia; Mo, moderate epithelial dysplasia.
Necrotic tissue could be observed in the treated area 1 week after cryosurgical treatment. The necrotic tissue slough separated spontaneously after approximately 2 weeks, leaving a fully epithelialized surface and healed mucosal tissue. Total clinical healing of OL could be observed in all patients after 30 days (Figs. 1B and D). No bleeding, no loss of tissue, no scarring, and no infection in the treated sites for either groups could be observed. In the non-LLLT group, seven patients (70%) reported pain, while in the LLLT group, 4 patients (50%) reported pain. Moreover, patients from the LLLT-group tended to report a lesser intensity of pain than did those from the non-LLLT group (p = 0.249; Fig. 2). Seven patients reported no pain (3 in the non-LLLT group and 4 in the LLLT group). In relation to the edema, no statistically significant difference between the groups could be observed (p = 0.342). Eight patients reported edemas (3 in the non-LLLT group and 5 in the LLLT group) within 24 h after treatment. Patients underwent follow-up examinations for 6–12 months (mean of 9 months) (Table 1); no recurrence of OL was found in any of the patients.

Intensity of pain in patients submitted to cryosurgical treatment (the non-LLLT group, n = 10) and patients submitted to cryosurgical treatment associated with low level laser therapy (the LLLT group, n = 8).
Discussion
The current study is the first of its kind to compare the ability of LLLT to alleviate pain caused by the cryosurgical treatment of OL in a blinded randomized clinical trial. The main findings included: (1) the cryosurgical treatment protocol proved to be clinically effective regarding OL resolution and (2) the LLLT reduced post-surgical pain.
The current results demonstrate that each of 18 cases of OL submitted to cryosurgical treatment presented a total clinical healing with no evidence of tissue loss, scarring, bleeding, or infection in follow-up examinations. These results are in accordance with previous studies. 5 –10,12
OL is usually treated by conventional surgery. However, this may cause delayed healing due to tissue contraction, trans-surgical bleeding, and post-surgical pain. 4,25,26 Cryosurgical treatment presents a good alternative to surgical excision, considering that the destruction of the pathologically changed tissue is possible, that it can allow the mucosa to return to a normal clinical appearance with complete regeneration and no scar formation, and that it can avoid a consequent loss of function. 16 Treatment of OL should avoid defects, especially in aesthetically sensitive areas, such as the gingiva, where extensive injuries caused by tissue loss may occur. In the present study, in the cases of gingiva submitted to cryosurgical treatment, the absence of scars and the preservation of functions were possible.
The recurrence rate of OL is variable in conventional surgery (10–35%), 3 cryosurgical treatment (0–32%), 5,7,9 and laser surgery (20–40%). 4,27,28 Regarding malignant transformation, it appears that none of these modalities stands out as superior to another. The use of cryosurgical treatment of OL, as compared to other methods, has proven to be quite effective, especially when one considers its low cost, its easy execution, and the possibility of its application in extensive lesions that would otherwise require several sessions for complete removal. 5 –13
Discomfort caused by cryosurgical treatment includes mild to moderate pain and the presence of edemas. 9,11 –13 In this light, the LLLT association showed a tendency toward the improvement of the painful symptoms associated with cryosurgical treatment. In fact, LLLT has proven to be effective in the treatment of damaged oral tissue as well as in the alleviation of pain. 18,21 The use of LLLT in controlling postoperative pain has been previously studied. 29 –31 Clinically, LLLT has been used successfully in the treatment of chronic pain, especially as regards musculoskeletal conditions. 32 While some studies have shown positive outcomes, others have demonstrated less than satisfactory results. 33 These differences could be explained by variations in wavelength, power levels, irradiation method, and exposure time of LLLT. The LLLT stimulates cellular activity and leads to the release of growth factors caused by inflammatory cells 31,33,34 It also induces keratinocyte proliferation, angiogenesis, and mast cell activation, which may accelerate wound healing. 35 This acceleration is the result of a shorter acute inflammation phase and an earlier commencement of the proliferative phase of tissue repair when granulation tissue is produced. 35 Other LLLT action mechanisms have postulated that photons are made up of wave lengths of a visible or nearly infrared spectrum. These photons are absorbed by chromophore enzymes, such as cytochrome c oxidase. Alterations in the activity of the cytochrome c oxidase in turn increases the production of adenosine triphosphate (ATP), which leads to the normalization of the cellular function. 36
The expected effect of LLLT in this study may also be related to biochemical and bioelectric properties. The bioelectric effect occurs by increasing the synthesis of ATP to maintain the membrane potential, in turn preventing depolarization and thus hampering the transmission of painful stimulus. 37 Another possible explanation for the neuropharmacological and analgesic effects of LLLT is the increase in blood circulation and the release of endorphins. 38 Alterations in neuronal activity have also been found to play a role in pain relief through laser therapy. 32
In conclusion, the LLLT is an important strategy to reduce post-surgical pain caused by the cryosurgical treatment of OL.
Footnotes
Acknowledgments and Author Disclosure Statement
We are grateful to Fundação de Amparo a Pesquisas do Estado de Minas Gerais (FAPEMIG, Brazil) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, Brasil) for their financial support. The authors thank to DMC LTDA (São Carlos, Brazil) for their supply of the 660 AsGaAl laser and NUPEN for assistance. MCF Aguiar, TA Silva, and RA Mesquita are research fellows of CNPq.