
Abstract
Introduction
Current evidence, however, suggests that the Early Treatment Diabetic Retinopathy Study (ETDRS) treatment protocol with laser still remains the most effective treatment of DME. 7 ETDRS demonstrated that argon laser photocoagulation reduces the risk of severe visual loss in eyes with DME by 50%. 8 The end point of this laser technique is the placement of a visible laser spot over the area of retinal thickening. With standard laser techniques as recommended in ETDRS, some patients have deterioration of vision caused by subretinal fibrosis, subretinal neovascular membranes, progressive enlargement of laser scars, and visual field loss. 9 –15 These complications have been attributed to spread of thermal energy and collateral damage to adjacent neural retinal and choroidal layers with continuous wave laser therapy. To reduce this collateral damage, other laser wavelengths such as diode (810 nm), and techniques such as subthreshold and micropulse laser delivery have been evaluated in the management of DME. 16,17 Histological studies have shown that application of diode laser pulses of short duration results in selective ablation of the retinal pigment epithelium with little damage to the neural retina and the choriocapillaris. 18,19
The use of subthreshold, micropulse diode laser in patients with DME was first reported approximately a decade ago by Friberg and Karatza. 20 Since then, there have been only a few other studies evaluating the role of subthreshold, micropulse diode laser in treating patients with DME. 21 –26 None of these studies have studied the efficacy of this technique using multifocal electroretinography (MfERG), which is the most sensitive electrophysiological test to detect functional effects on the retina. The present study is the first randomized study to evaluate the safety and efficacy of subthreshold micropulse diode (SDM) laser in the management of DME.
Methods
This was a prospective randomized interventional study performed on 46 eyes of 33 patients with DME. Only patients with the nonproliferative stage of diabetic retinopathy were included in the study. The study protocol was cleared by the ethics committee of All India Institute of Medical Sciences, New Delhi. Informed consent was obtained from all patients before enrolment into the clinical study.
Patients for the study were recruited from the medical retina clinic of our center from July 2006 to January 2008. Patient eyes were randomized to either of two treatment groups: Group 1 (SDM laser group) and Group 2 (Nd:YAG laser group).
We excluded patients with proliferative retinopathy, significant media opacities precluding fundus evaluation and laser therapy, prior medical treatment (intravitreal/ peribulbar steroids or anti-angiogenic drugs), prior laser treatment, macular pathology other than diabetic maculopathy, and ocular surgery within 6 months prior to screening. Patients with uncontrolled hypertension and renal failure requiring dialysis were also not enrolled into the study.
Best corrected visual acuity (BCVA) was noted using the ETDRS chart and logMAR of EDTRS acuity at a distance of 4 m. In all patients, contrast sensitivity was recorded at 1 m in the same room and at the same illumination settings using the Pelli-Robson chart. Color fundus photography and fluorescein angiography (FA) were performed using the Zeiss 450 plus fundus camera (Carl Zeiss Meditec, Germany). Fundus photographs at 50° were chosen for this study to cover the central 45° testing field of the MfERG.
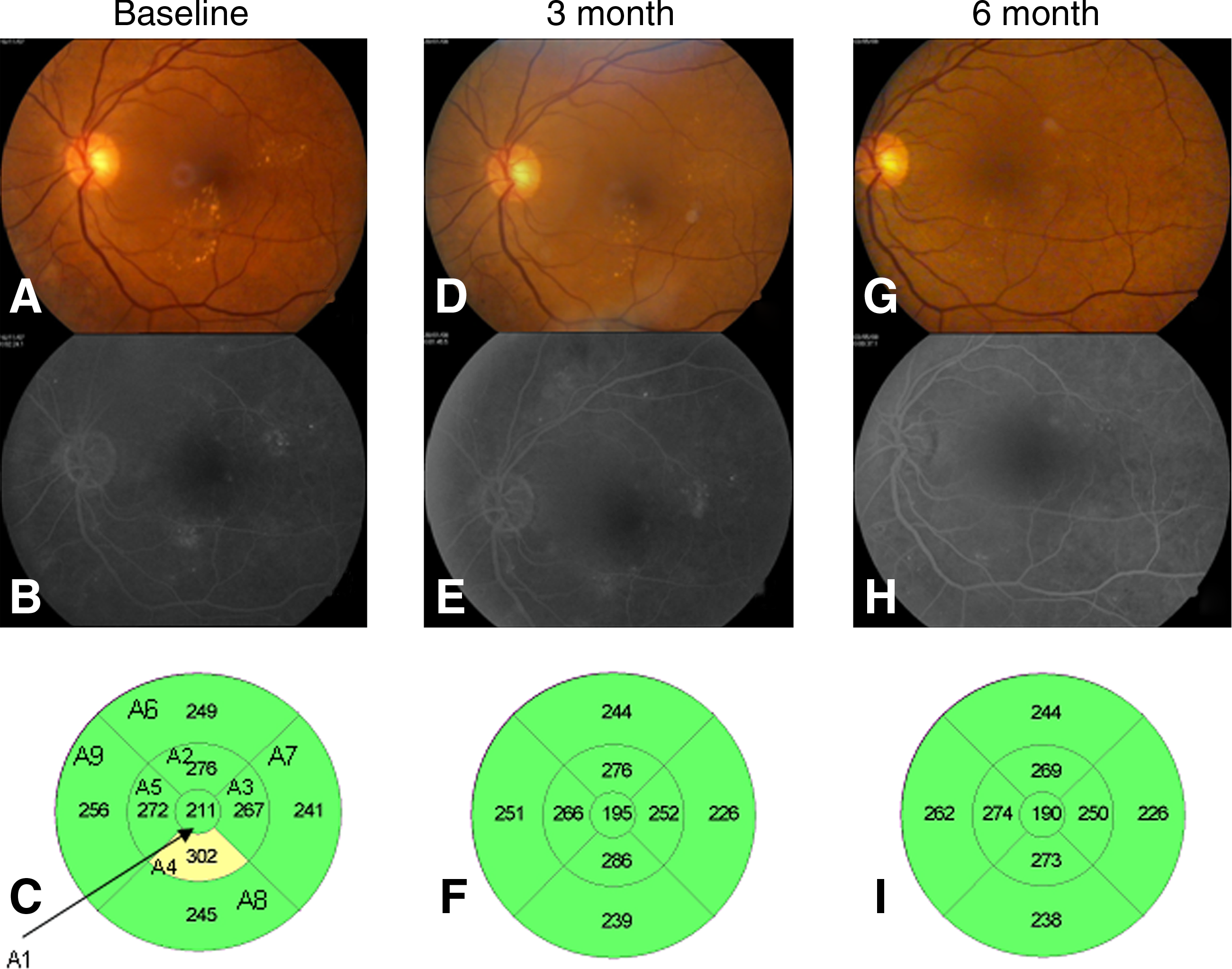
Optical Coherence Tomography (OCT) scanner (Zeiss Instruments, Dublin, CA), with the standard fast macular scan protocol was used to determine the macular thickness. For quantitative evaluation of the macula, the retinal map thickness printout was divided into nine EDTRS areas including a central disc with a diameter of 1000μm and inner and outer rings of 3000 and 6000μm respectively. Each ring was further divided into four quadrants (Fig. 1). Images were judged to be “acceptable” only if they had good demarcation of the vitreoretinal and chorioretinal interface allowing for a correct identification of the two interfaces by the software, and absence of artifacts caused by eye motion or unstable fixation.
(
MfERG was recorded using the Metro-Vision ERG machine (Metrovision, Pe´renchies, France) and International Society for Clinical Electrophysiology of Vision (ISCEV) guidelines. The patient preparation included adequate pupillary dilation using Tropicamide (Alcon Laboratories, Inc., Fort Worth, TX) 1.0% and phenylephrine 2.5% eye drops. Recording was done after placing the electrodes: one contact lens electrode over the cornea (anesthetized with proparacaine 0.5% drops), and two gold foil electrodes (one on the forehead and the other on the temporal side of the eye to be stimulated). The fellow eye was occluded. An array of 61 hexagonal elements was delivered by an eye camera-display-refractor unit (EDI) driven at a frame rate of 75 Hz. The hexagons were modulated between white (200 cd/m2) and black (<2 cd/m2) according to an m-sequence during the 5-min recordings. The stimulus unit was adjusted for best focus of the central fixation target before the recording.
Laser photocoagulation of the enrolled patients was performed by a single surgeon (P.V.) using transequator lens (Volk Optical Inc., Mentor, OH) to deliver the laser energy. Iridex Oculight SLx (Iris Medical, Mountain View, CA) was used for delivery of SDM laser and Zeiss Visulas 532s (Carl Zeiss Meditec AG, Germany) for delivery of 532 Nd:YAG laser. For patients randomized to the diode photocoagulation (Group 1), a spot size of 125 μm was chosen. The power was initially adjusted upward to a minimum threshold value for a barely visible burn (160–260 mW). The power was then set at half the value and the delivery was changed to micropulse mode with an “on” time of 0.1 ms and an “off” time of 1.9 ms in a pulse envelope of 2000 ms' duration. In patients treated with Nd:YAG laser (Group 2) a spot size of 50–100 μm, power (90–180 mW) and an exposure of 0.1 sec was used. The laser spots were placed one spot size apart in the area of leakage. Direct ablation of visible microaneurysms located >500 μm was also performed in this group. The standard procedure (i.e., power needed to achieve a barely visible reaction) was used to deliver energy in the Nd:YAG laser group. For the SDM group, a test burn was given in the nasal retina to achieve a visible reaction. This numeric value was halved and the machine set to micropulse mode to deliver SDM laser (again according to recommended approach) at 10% duty cycle.
Patients were followed up at 6 weeks, 3 months, and 6 months. At the 3-month and 6-month visits the following examinations were performed: BCVA, contrast sensitivity, FA, OCT, and MfERG. OCT was performed at the 6week follow-up also.
Statistical analysis
Descriptive statistics to determine mean, standard deviation, and frequency distribution were produced using SPSS (version 15). Mann-Whitney and Friedman tests were for intergroup and intragroup nonparametric data analysis, respectively and a p value <0.05 was considered to be statistically significant.
Results
We included and randomized 46 eyes of 33 patients who matched our eligibility criteria to either SDM laser (Group 1) or Nd:YAG laser (Group 2) and followed up for 6 months. Baseline patient data are summarized in Tables 1 and 2. In Group 1, there were 20 eyes with focal macular edema and 3 with diffuse macular edema. In Group 2, there were 22 eyes with focal macular edema and 1 with diffuse macular edema.
BCVA, Best corrected visual acuity; MfERG, Multifocal electroretinography.
BCVA, best corrected visual acuity; MfERG, multifocal electroretinography.
The glycosylated hemoglobin median value in Group 1 at baseline was 9.46±1.75% (range 6.9–13.6), at 3 months it was 7.53±0.72% (range 6.7–8.6) and at 6 months it was 7.40±1.01% (range 6.2–10.5). The median value in Group 2 at baseline was 8.98±1.49% (range 6.9–11.6), at 3 months it was 7.73±1.38% (range 6.2–8.6) and at 6 months it was 7.39±1.34% (range 6.1–10.7). Systemic control of diabetes as indicated by these values was comparable in both the groups and was not statistically significant (p=0.97). All patients completed the follow up visits and no patient was excluded at any point during the study.
The baseline mean visual acuity in Group 1 was 0.41±0.3. Following treatment, visual acuity was 0.41±0.3 and 0.43±0.3 (p=0.48) at the 3- and 6-month follow-up visits, respectively. Twenty (87%) patients had stabilized vision or improved visual acuity, whereas three patients showed a decrease (13%). The maximum visual acuity gained was 10 letters (two lines on the ETDRS chart). The baseline mean visual acuity in Group 2 was 0.33±0.2. On follow-up visits after laser, the visual acuity at the 3rd month was 0.36±0.2 and at the 6th month it was 0.41±0.3 (p=1.0). Fifteen (65%) patients had stabilized or improved vision whereas eight patients showed a decrease (35%). The maximum visual acuity gained was 10 letters (two lines on the ETDRS chart). We found no significant difference between the two groups as regards the initial and final mean visual acuity (p=0.77).
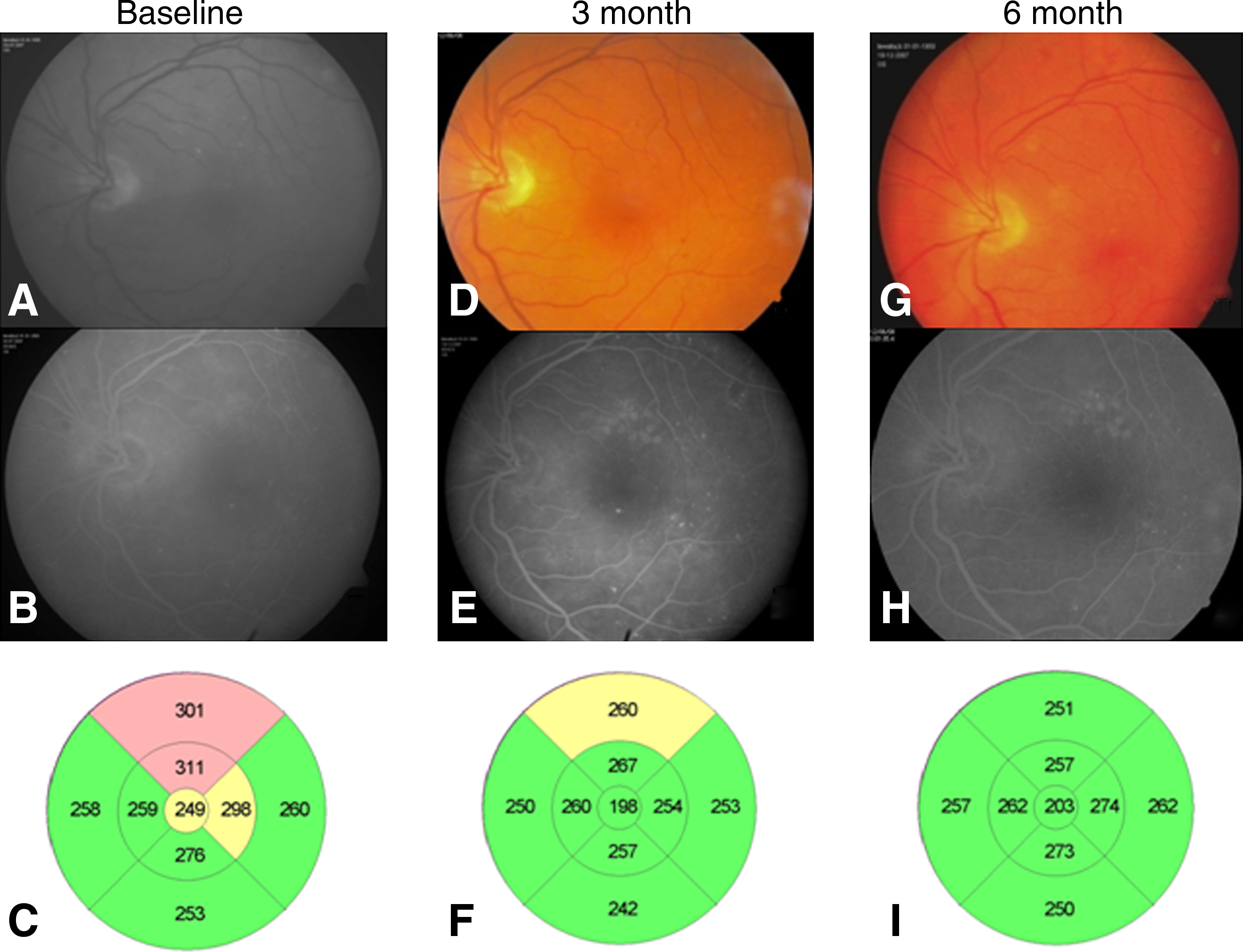
In Group1, the baseline mean average macular thickness was 298.5±49.3 μm. On follow-up visits post-laser, the average macular thickness at the 6th week was 303.5±56.0 μm, at the 3rd month it was 286.7±52.7 μm, and at the 6th month it was 274.9±62.9 μm (Fig. 1). In this group significant decrease in mean average macular thickness occurred at 6 months (p=0.047). In Group 2 the baseline mean average macular thickness was 312.9±45.8 μm. On follow-up visits post-laser the average macular thickness at the 6th week was 299.7±50.6 μm, at the 3rd month it was 296.0±34.3 μm, and at the 6th month it was 286.7±32.8 μm (Fig. 2). In this group, significant decrease in mean average macular thickness occurred at 6 months (p=0.029). Although the final outcome was comparable in both groups (p=0.64), it took a slightly prolonged time in the subthreshold micropulse group for the edema to decrease. It is worth noting that there was a mean increase in the macular thickness at 6 weeks in the diode laser group, though it was not statistically significant (p=1.0). Changes in central macular thickness from baseline at various follow-up intervals are shown in Fig. 3.
(
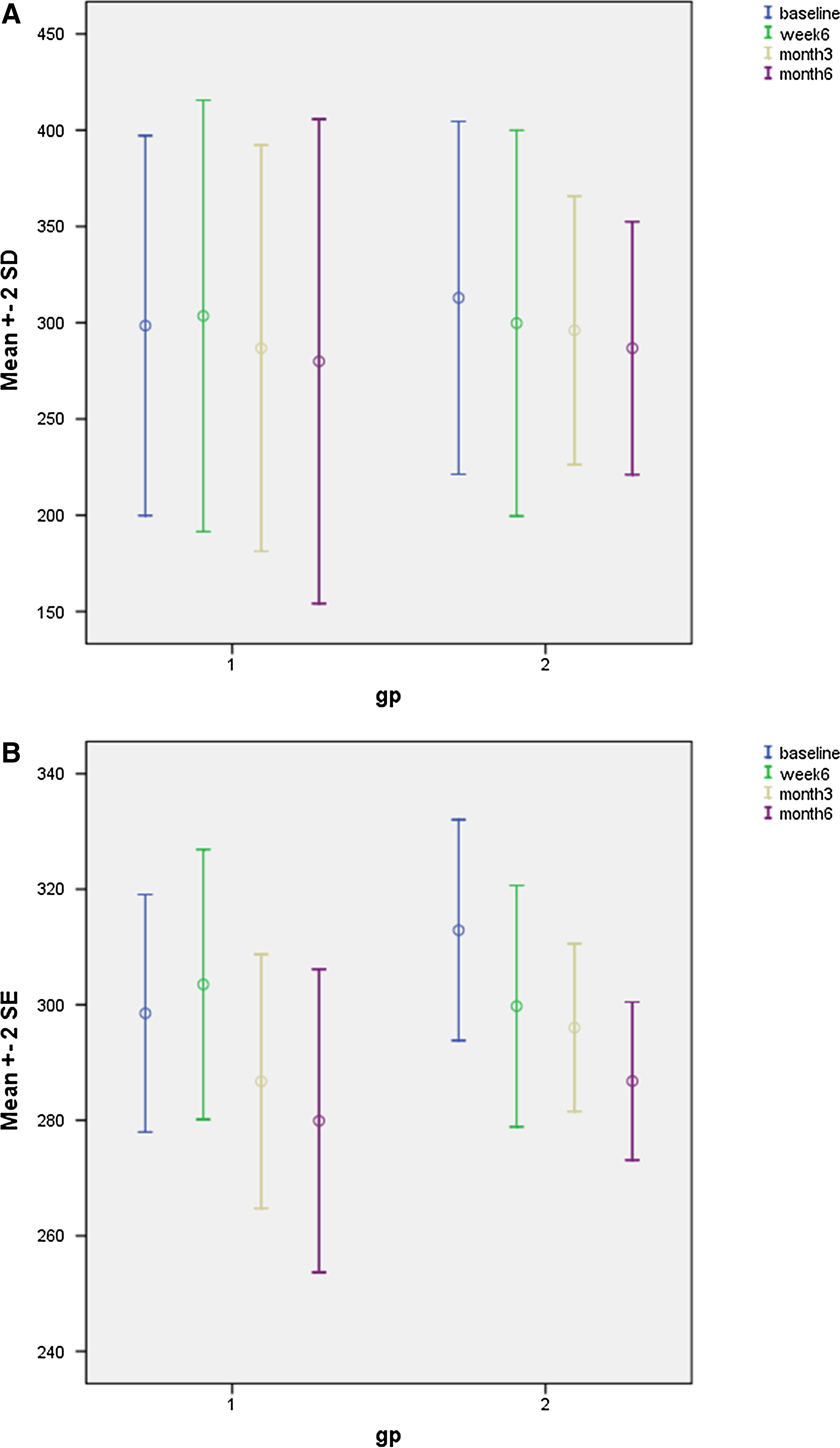
Bar graph showing change in central macular thickness (CMT) from baseline.
Multifocal electroretinogram changes were recorded at baseline, 3 months, and 6 months. The mean values of the implicit time of the P1 wave were compared. In Group1, the baseline mean P1 wave implicit time delay was 46.27±4.9 ms. At the 3 and 6 month follow-up visits, the mean P1 wave implicit time delay was 44.57±2.9 and 45.27±3.4 ms (p=0.23), respectively. In Group 2, the baseline implicit time mean value was 46.55±4.9 ms. On follow-up visits post-laser the mean value at the 3rd month was 44.99±3.3 ms and at the 6th month it was 45.27±4.1 ms. There was no statistically significant change in the mean implicit time delays in both the groups (p value 0.65 at 3 months and 0.46 at 6 months). In both groups, we found areas of no signal recording (signal void areas) after laser treatment. In the double-frequency Nd:YAG laser group, 18 eyes had developed focal signal void regions in the treated region (Fig. 4). In comparison, signal void areas were evident in only 4 eyes treated with SDM laser. Focal signal void areas are those in which the waveforms do not have any value, and they occur in regions with functional loss.
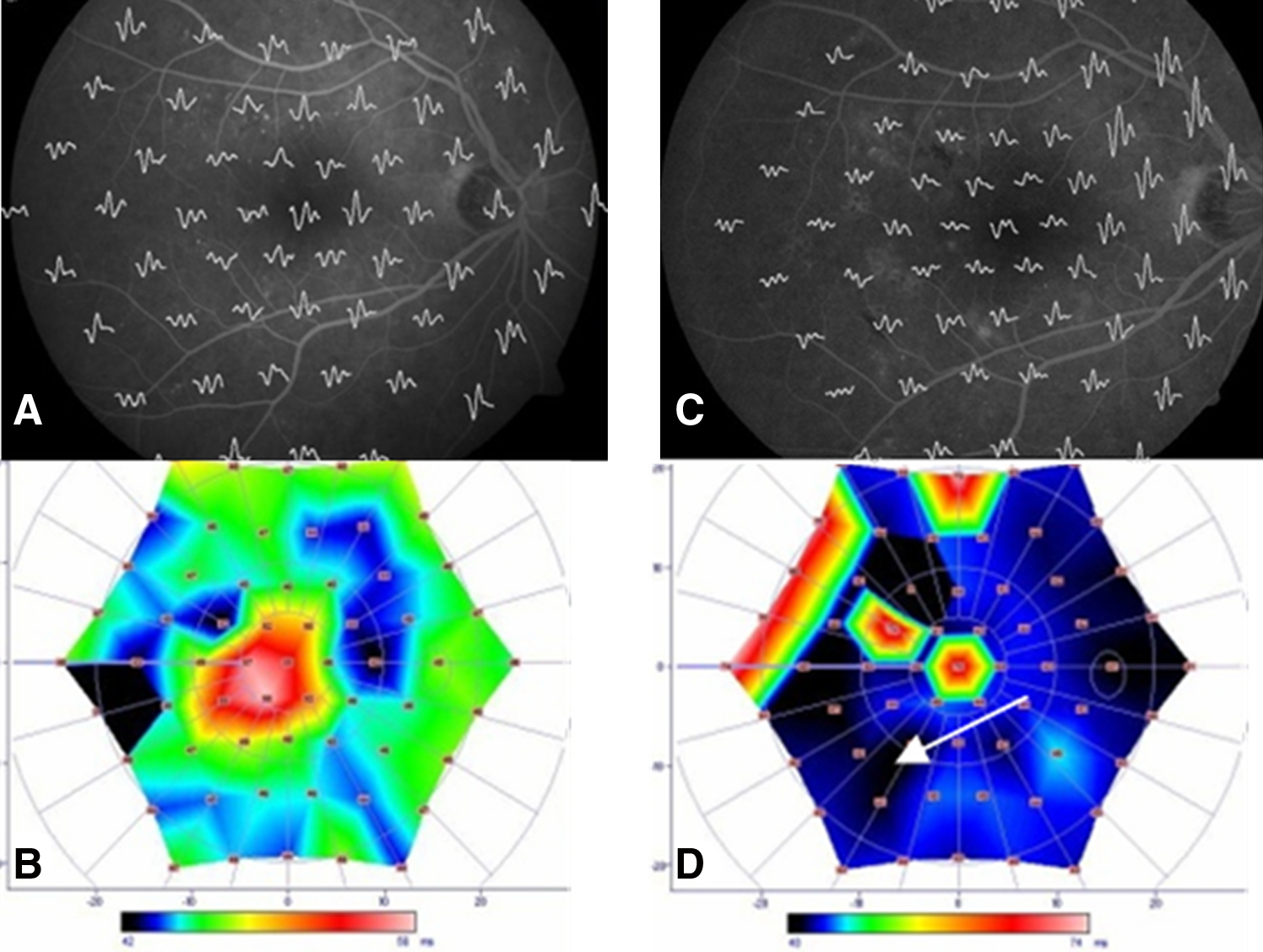
MfERG images before and after treatment of macular edema with Nd:YAG laser (at 3-month follow-up). Note focal signal void areas (white arrows) following laser photocoagulation.
Change in the BCVA, contrast sensitivity, central macular thickness, and implicit time on MfERG in both SDM laser and Nd:YAG laser groups are summarized in Tables 1 and 2.
We did not encounter any treatment-related complications such as lens opacity, choroidal hemorrhage, or retinal hemorrhage with either of the procedures.
Discussion
SDM laser is form of laser therapy that has been shown to result in selective ablation of the retinal pigment epithelium. The selective ablation is achieved by keeping the laser energy delivered in ultra-short periods unlike the conventional, continuous wave lasers. As SDM laser decreases the risk of collateral thermal damage to adjacent layers of the retina, it is being evaluated as a safer method for the treatment of patients with DME. The present study is the first to evaluate the effect of SDM laser in comparison to conventional frequency-doubled Nd:YAG laser using MfERG in patients with DME.
The first report of treating patients with DME with SDM laser was by Friberg and Karatza. 20 They reported a decrease of macular edema in 87.5% of treated eyes. Subsequently, Laursen et al. compared the efficacy of SDM laser and conventional argon laser in a randomized trial and reported that SDM laser was equally efficacious. 21 A year later, Luttrull et al. reported that visual acuity was maintained in 85% of eyes treated with SDM laser and that macular edema resolved in 79% of patients. 22 These three reports did not discuss quantitative changes in the edema following treatment, as no data using OCT were collected.
A subsequent report, again by Luttrull et al., provided OCT changes following SDM laser. 23 These authors found that macular thickness did not change significantly in the first 2 months after treatment. At 3 months, however, reduction of macular thickness was observed. Ohkoshi and Yamaguchi have recently reported early and rapid reduction of macular edema following treatment of Japanese patients with SDM laser. 25
Vujosevic et al. have shown that in terms of reduction in macular thickness, SDM laser is as efficacious as conventional laser. 26 In this study they also found that patients treated with SDM had improved retinal sensitivity on microperimetry.
Similar to the findings in previously reported studies, we noted that SDM laser was as effective as conventional frequency-doubled YAG laser in maintaining visual acuity. Although the final change in central macular thickness as measured on OCT was comparable in both groups, it took a slightly prolonged time in the subthreshold micropulse group for the edema to decrease. This observation is similar to that reported by Luttrull et al., 23 but unlike the results of Ohkoshi and Yamaguchi. 25
The present study is the only report showing the effects of SDM and conventional laser using multifocal ERG. Using this electrophysiological modality of testing macular function, we found no statistically significant change in the mean implicit time delays in both the groups. Interestingly however, a large majority of subjects in the double- frequency Nd:YAG laser group had developed focal signal void regions in the lasered region. In comparison, signal void areas were evident in only a few eyes treated with SDM laser. This observation on MfERG seems to indicate that following SDM laser, retinal functioning at the physiological level is better maintained compared to the results after treatment with conventional laser. This is probably a result of lesser collateral thermal damage to the neural retina.
One limitation of this study is the inclusion of patients with both focal and diffuse macular edema. Of the 46 treated eyes, 4 were found to have diffuse leak on fluorescein angiography (3 in the SDM group and 1 in Nd:YAG group). Also, macular thickness in patients with diffuse edema in this study was not severe (<400 mu). Because of the small numbers and less severe nature of the condition in these patients with diffuse edema, it is unlikely that the inclusion of these eyes in statistical analysis would have impacted the results.
In conclusion, we found SDM laser to be as effective as conventional double- frequency ND:YAG laser in the treatment of DME. Evaluation using MfERG is unique to this study and suggests that SDM may be a better modality in retaining physiological functioning of the neural retina compared to conventional laser.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.