
Abstract
Introduction
A significant body of evidence has now accumulated demonstrating that low-level laser therapy (LLLT) has a positive effect on bone tissue metabolism and on fracture consolidation. 4,5 In vitro studies using osteoblastic cells showed that LLLT is capable of increasing mitochondrial activity, 6 osteoblast DNA and RNA synthesis, bone nodule formation, 1 osteocalcin and osteopontin gene expression and ALP activity, increasing osteoblast proliferation. 7,8 Also, LLLT is able to accelerate the process of fracture repair in rabbits and rats, increasing the callus volume and bone mineral density. 9,10 Ribeiro et al. 10 found an upregulation for cyclooxygenase-2 expression in bone cells produced by laser irradiation, resulting in the improvement of bone repair in tibial bone defects of rats. Denadai et al. 11 observed that the association of 650 nm laser and bone morphogenetic proteins (BMPs) was capable of accelerating fracture consolidation in tibial defects in rats. In addition, Blaya et al. 12 demonstrated that the animals irradiated with 685 and 830 nm lasers showed a higher concentration of newly formed bone.
However, the mechanism by which LLLT acts on osteoblast cells and bone healing is not fully understood and, for many, the use of LLLT as a treatment modality is still controversial. 13 Thus, there is a clear clinical need to understand the molecular details of pathways that control bone formation after laser irradiation, which might possibly accelerate the healing fractures and treat the 5–10% of fractures that fail to heal satisfactorily. 14
It is well known that bone regeneration is a complex temporal and spatial interaction of osteoclasts and osteoblats cells, regulated by a series of cell-signaling molecules, cytokines, proteins, and growth factors, which induce or modulate osteoproducing cells to create a competent bone mass. 15 Osteoblasts are effector cells for bone formation with the widely known ability to form bone tissue by secretion of alkaline phosphatase, type I collagen, proteoglycan, bone sialoprotein, and osteocalcin. Also, bone morphogenetic proteins (BMPs) are involved in osteoblast differentiation and bone regeneration. BMPs are members of the transforming growth factor (TGF) superfamily of signaling molecules and act as morphogens to regulate embryonic development. 16,17 Evidence suggested BMP derived from mesenchymal cells and osteoblasts could exhibit chemotactic properties to stimulate differentiation of mesenchymal cells into osteogenic/chondrogenic lineage and increase expressions of alkaline phosphatase and osteocalcin. 18 In addition, BMP also affect bone remodeling through the regulation of osteoclast bone-resorbing activity. 19 BMP have been reported as having a role in the mechanical stimulation of fracture healing and chondrocyte differentiation. 7,9 Four members of the BMP family, BMP-2, BMP-3, BMP-4, and BMP-7, have shown positive effects on fracture healing and bone formation. 20 –23
RUNX2 is a multifunctional transcription factor that controls skeletal development by regulating the differentiation of chondrocytes and osteoblasts and the expression of many extracellular matrix protein genes during chondrocyte and osteoblast differentiation. 24
Although the positive effects of LLLT on tissue regeneration, the mechanism by which the LLLT acts on bone is not fully understood. 19 Since this modality is widely used to accelerate the process of tissue healing, the aim of this study was to extend prior histological descriptions of laser therapy on bone healing by characterizing the temporal–spatial pattern of the expression of bone formation genes. We used histology and quantitative real-time polymerase chain reaction (qPCR) to assess gene expression following laser therapy irradiation on created bone defects in tibias of rats.
Methods
Animals
Male Wistar rats (weighing 300 ± 20 g, 12–13 weeks, N = 60) were distributed randomly into two groups: control or laser irradiated group. They were maintained under controlled temperature (22 ± 2°C), light–dark periods of 12 h, and with free access to water and commercial diet. All animal handling and surgical procedures were strictly conducted according the Guiding Principles for the Use of Laboratory Animals. This study was approved by the Animal Care Committee guidelines of the Federal University of São Paulo. As described below, noncritical size bone defects were performed on both tibias. Rats were killed at 7, 13, and 25 days after surgery.
Surgery
Noncritical size bone defects were surgically created at the upper third of the tibia (10 mm distal of the knee joint). Surgery was performed under sterile conditions and general anesthesia induced by intraperitoneal injection of xilazin (Syntec®, 20 mg/kg, IP) and ketamin (Agener®, at 40 mg/kg, IP). The medial compartment of the tibia was exposed through a longitudinal incision on the shaved skin and muscle tissue. A standardized 2.5-mm diameter bone defect was created by using a motorized drill (12,356 rpm) under copious irrigation with saline solution. The cutaneous flap was replaced and sutured with resorbable polyglactin, and the skin was disinfected with povidone iodine. The animals received analgesia (i.m., 0.05 mg/kg buprenorphine) and were returned to their cages. The health status of the rats was monitored daily.
Treatments
The treatments started 24 h post-surgery and were performed for 3, 6 and 12 sessions, with an interval of 48 h. A low-energy Ga-Al-As laser 830 nm, 30 mW, continuous wave laser, 0.028 cm2, 1.071 W/cm2, 47 s, 1.4 Joules, 50 J/cm2 (Tera laser, DMC Equipamentos, São Carlos, SP, Brazil) was used. The parameters were specified based on the equipment specification of the manufacturer. The irradiation was performed in one point, above the area of the injury, through the punctual contact technique. On days 7, 13, and 25 post-injury, rats were sacrificed individually by carbon dioxide asphyxia. Both tibias were removed for analysis.
Histopathological analysis
For the qualitative histopathological analysis, the right tibiae were used. They were removed, fixed in 10% buffer formalin (Merck, Darmstadt, Germany) for 48 h, decalcified in 4% EDTA (Merck), and embedded in paraffin blocks. Five-micrometer slices were obtained in a serially sectioned pattern and stained with hematoxylin and eosin (H.E stain, Merck). A descriptive qualitative histopathological evaluation of the total area of the bone defect was performed by a pathologist (blinded to the treatment), under a light microscope (Olympus, Optical Co. Ltd, Tokyo, Japan), at 25x magnification. Any changes in the bone defect, such as presence of woven bone, bone marrow, inflammatory process, granulation tissue, or even tissues undergoing hyperplastic, metaplastic, and/or dysplastic transformation were investigated per animal.
Quantitative RT-PCR (qRT-PCR)
Immediately postmortem, right tibias were dissected (periosteum intact) and rapidly frozen in liquid nitrogen. The ends of each tibia were removed and region of the callus stored (−80°C) until analysis by quantitative real-time polymerase chain reaction (qPCR). Total RNA was isolated using standard protocols. Trizol reagent (1 ml, Invitrogen, Carlsbad, CA) was added to the sample and allowed to thaw. The mixture was transferred to a polypropylene tube and incubated (room temperature, 5 min). Chloroform (0.2 ml, Sigma, St. Louis, MO) was added, mixed vigorously, and the mixture was transferred to a 2 ml tube (Eppendorf, Hamburg, Germany) and centrifuged (2°C, 15 min). The nucleic acid phase was decanted and an equal volume of RNase-free 70% ethanol was added. Potential DNA contamination was removed by RNase-free DNase I (Invitrogen). RNA integrity was verified by RNA gel electrophoresis and spectrophotometry. Four genes of interest were selected representing processes associated with osteogenesis (Table 1). For each gene, rat-specific primers were designed for real-time PCR around exon junctions where possible. All real-time primers were initially tested against standards and a standard curve was generated. First strand cDNA was synthesized (M-MLV RT, Invitrogen) from total RNA (1 μg). RT-qPCR reactions were carried out at 50 μl total volume. Following an initial denaturing step for each primer (Table 1), the genes of interest were amplified through 40 cycles (Rotor-Gene, R 3000, Robert Research, Mortlake, Australia). Gene amplification was measured by SYBR green (Applied Biosystems, Carlsbad, CA) fluorescence during the annealing/elongation phase. All samples were run in duplicate and the average was used for further analysis. Measures of real-time PCR cycle to threshold were normalized to the expression of ribosomal protein S18 (RPS18) for each tibia. For comparison between experimental groups, RPS18 normalized expression from each tibia was divided by the normalized gene expression from the control group to obtain a fold increase in gene expression of LLLT group and control group in days 7, 13, and 25.
ALP, alkaline phosphatase; BMP4, bone morphogenetic protein 4; OC, osteocalcin; Runx 2, transcriptional factor.
Statistical analysis
The normality of all variables' distribution was verified using Shapiro–Wilk's W test. Two-way ANOVA was used to assess the effect of displacement level and time. Post hoc, multiple comparisons were made using Fisher's protected least significant difference tests with statistical significance defined as p < 0.05.
Results
Histological analysis
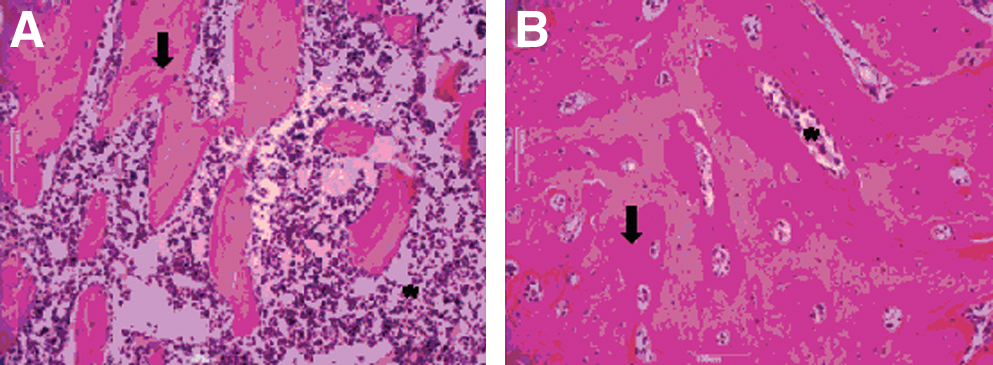
Seven days post-surgery, the defects in the control group were filled by highly cellularized granulation tissue. Eventually, new bone formation was observed on the surface of some bone particles (Fig. 1A). Specifically, this was noticed in five animals. The laser-irradiated animals demonstrated similar characteristics as those described in the control group (Fig. 1B). Woven bone formation was noted in six animals.

Bone defects after 7 days of surgery from control group
On day 13 after the surgery, the control group demonstrated new bone formation and remodeling bone trabecula surrounded by granulation tissue (Fig. 1B) marked by basophilic reversal lines. Bone marrow presented high vascularization as well. At the same period, laser irradiation produced an intense new bone formation, which was surrounded by highly vascularized connective tissue presenting slight osteogenic activity, with primary bone deposition (Fig. 2B).

Bone defects after 13 days of surgery from control group
On day 25, mature bone trabeculas were noted filling the bone defect in the control group (Fig. 3A). In the animals irradiated with laser, mature bone was also observed on the surface containing some areas of bone narrow (Fig. 3B).
Bone defects after 25 days of surgery from control group
Gene expression data
Figures 4, 5, 6, and 7 represent the temporal osteogenic gene expression in the control and LLLT treated group.
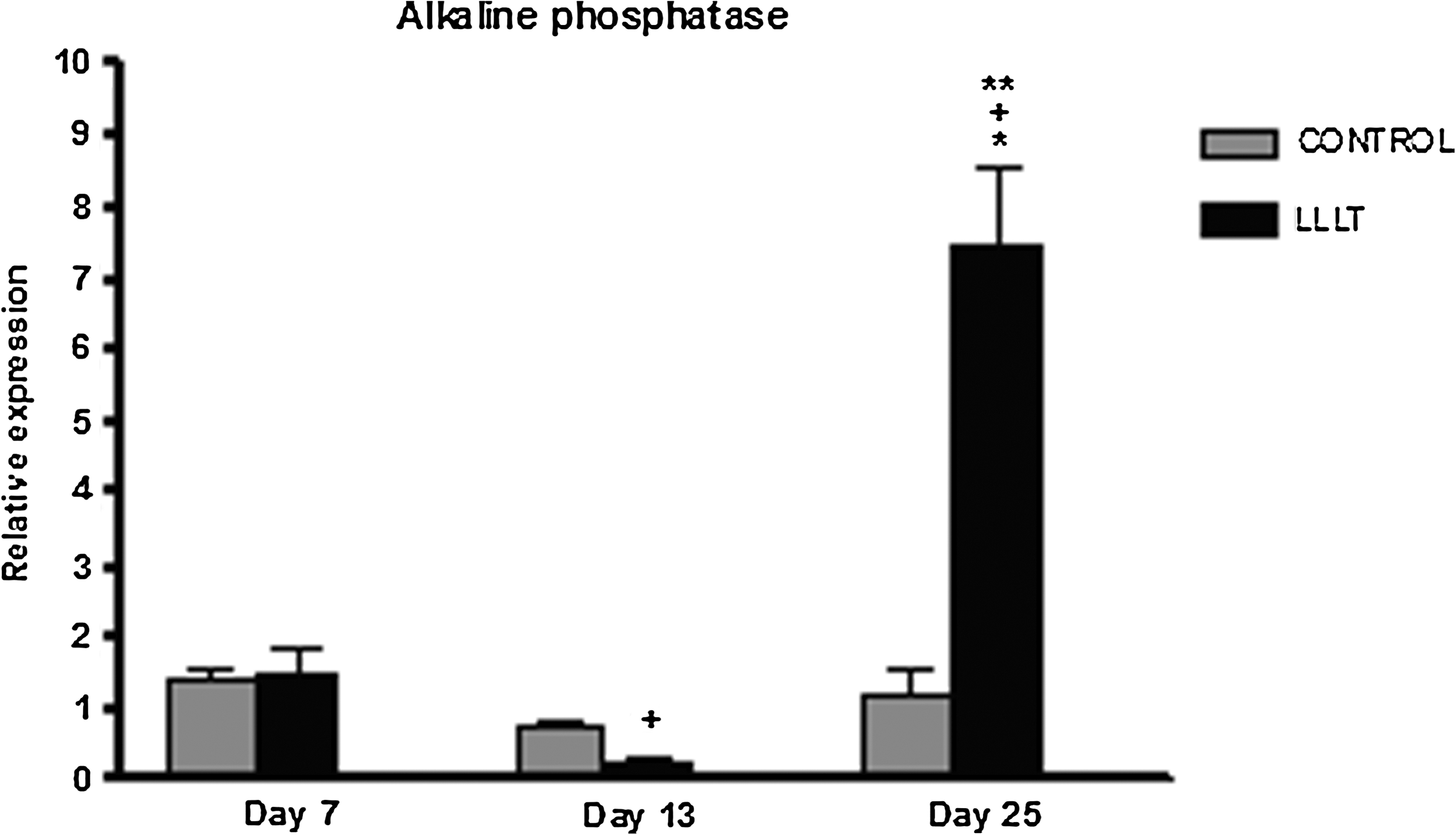
Means and SD of the changes in the expression of the ALP genes in the control and laser-treated animals measured by the RT-PCR. *p < 0.05 vs. control; + p < 0.05 vs. 7 days; **p < 0.05 vs. 13 days.
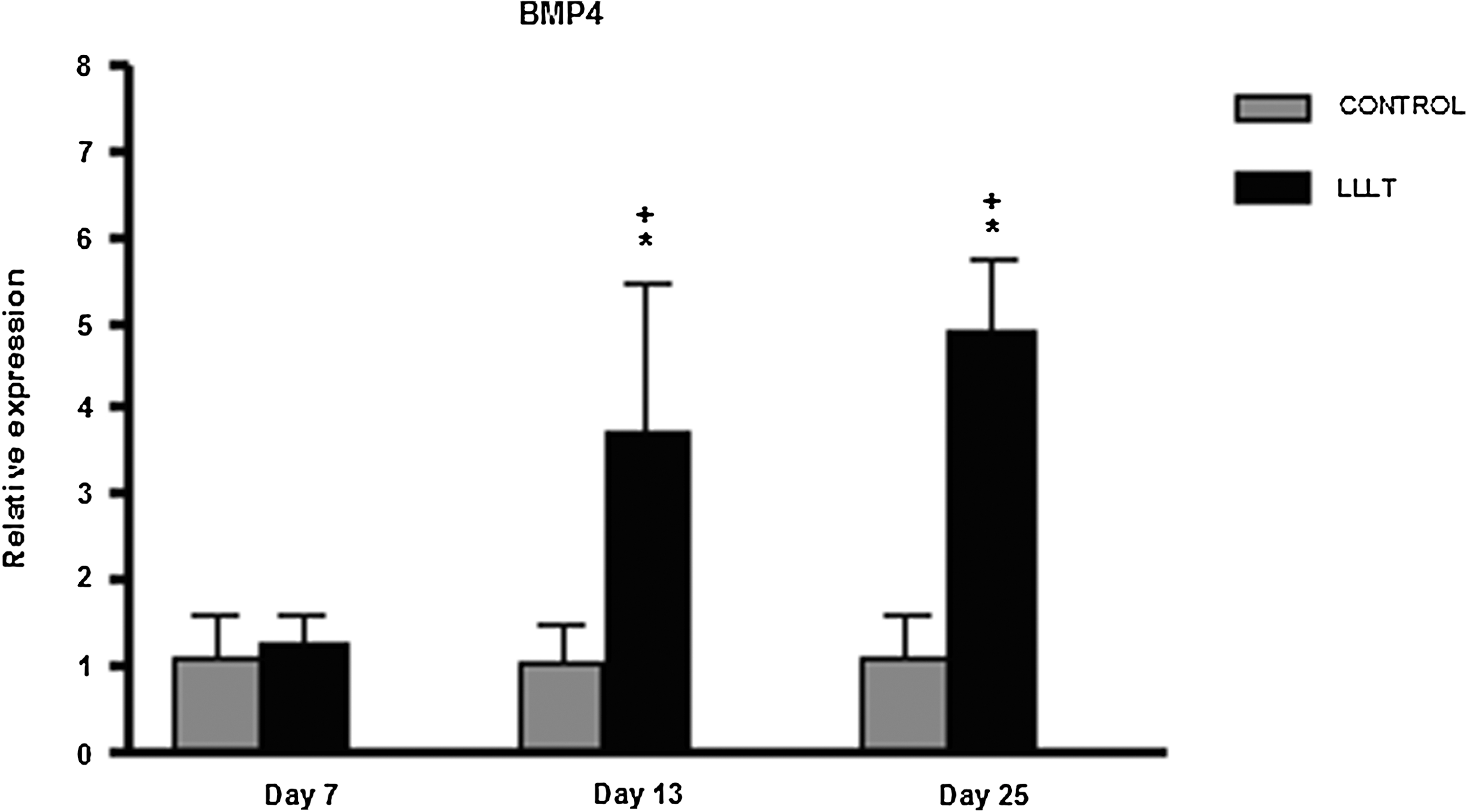
Means and SD of the changes in the expression of the BMP4 genes in the control and laser-treated animals measured by the RT-PCR. *p < 0.05 vs. control; + p < 0.05 vs. 7 days.

Means and SD of the changes in the expression of the osteocalcin genes in the control and LIPUS-treated animals measured by the RT-PCR. *p < 0.05 vs. control.

Means and SD of the changes in the expression of the ALP genes in the control and LIPUS-treated animals measured by the RT-PCR. *p < 0.05 vs. control; + p < 0.05 vs. 7 days.
Day 7: of the four genes reflecting osteogenic coupling potential in this model, it was observed that only osteocalcin was upregulated at this time point comparing the treated group and control group (Fig. 6). Expression of ALP, Runx2, and BMP4 did not significantly differ between the treated and control groups (Figs. 4, 5, and 7).
Day 13: only BMP4 was consistently and significantly upregulated in the laser-treated group when compared to the nontreated animals at this time point. BMP4 was upregulated at an average of 3.5-fold. Other genes did not show significant change after the laser therapy.
Day 25: a significantly increased ALP expression was observed in laser-treated animals, compared to the control (up by an average of 6.1-fold; Fig 4). Similarly, the expression of BMP4 and Runx 2 was also increased in the treated group compared to nontreated group (Figs. 5 and 7). BMP4 expression was significantly elevated, up by an average of 4.4-fold in bone defect treated with LLLT, compared to nontreated control. Also, Runx 2 increased 2.7-fold. However, no significant increase was found in the osteocalcin expression (Fig. 6).
Discussion
The present study aimed to investigate the effects of the LLLT on the histology and expression of osteogenic genes (alkaline phosphatase, osteocalcin, Runx 2, and BMP4) during the process of bone healing in tibias of rats. The histological analysis showed that animals treated with LLLT presented more mature trabeculas, higher amount of bone deposition, and highly vascularized connective tissue, especially at the intermediate and late stages of repair (13 and 25 days after surgery) when compared to control.
Also, RT-qPCR analysis showed that laser irradiation during the process of bone healing did not produce any effect on the early responses from osteoblastic cell proliferation genes (7 days post-surgery), except in osteocalcin gene expression. Interestingly, the gene response was followed by a significant upregulation of the osteogenic markers with the constant expression of BMP4 (intermediary and late stages of repair). LLLT was also able to produce a marked increase in ALP and Runx2, corresponding to an intense phase of bone cell activity and neoformed bone deposition and mineralization. To the best of our knowledge, this has not been demonstrated so far.
Laser therapy has emerged as an efficient noninvasive treatment to stimulate osteogenesis and to accelerate bone healing. 25,26 Such findings are in line with other studies investigating bone repair in rats. 27,28 A recent literature review of 34 articles found that laser therapy has a positive stimulating effect on bone both in vivo and in vitro. 28 These results indicated that the use of laser energy with infrared wavelengths can increase osteoblastic proliferation, collagen deposition, and bone formation. 28 Kazen et al. 5 also found an enhancement of the callus development in the early stage of the healing process in rabbits treated by laser therapy.
In our study, the expression of BMP4 was markedly increased in the laser-treated animals, at 13 and 25 days after surgery. BMPs induce differentiation to osteoblast from mesenchymal precursor cells and its role in facilitating fracture healing and bone formation is well known. 29 Probably, the upregulation of BMP4 in the treated groups was responsible by the earlier recruitment of cells observed in the histological analysis and the higher amount of neoformed bone tissue in this group, which may be a result of a higher number of mature osteoblasts and a higher deposition of neoformed bone.
Interestingly, the most prominent effect of laser therapy on osteogenic markers was observed at the last period evaluated, with an upregulation of ALP, BMP4, and Runx2. Runx 2 is essential for osteoblast differentiation and osteogenesis. During the process of bone differentiation, a set of bone-specific genes (ALP and osteocalcin) are activated and this transcriptional factor is a key regulator of osteocalcin and ALP. 30 ALP is also an important marker of early osteoblast differentiation but its function is less clear. 30 It can be suggested that the upregulation of the these genes in the laser-treated group could be responsible by the differentiation of osteoblast cells, a stimulation of osteogenesis, and higher deposition of bone matrix, which could correspond to our histological findings at the last period.
Regarding the effects of LLLT on the expression of specific osteoblastic markers, very few data have been reported. 31 Stein et al., 19 irradiating human osteoblast-like cells (SaOS-2) with 670 nm laser, observed that cell viability, alkaline phosphatase activity, and the expressions of osteopontin and collagen type I mRNA were slightly enhanced in the irradiated cells. Xu et al. 32 also investigated the effect of LLLT on the expression of mRNA RANKL and mRNA osteoprogesterin (OPG). The authors concluded that LLLT irradiation may directly promote osteoblast proliferation and differentiation, and indirectly inhibit osteoclast differentiation, by downregulating the RANKL:OPG mRNA ratio in osteoblasts. Conversely, some studies reported slight effects on alkaline phosphatase activity, 33 osteoglycine, 34 osteopontin, and bone sialoprotein expressions. 1 Bouvet–Gerbettaz et al. 31 evaluated the expression of mRNA of BMP2, ALP, osteocalcin, collagen type 1, and bone sialoprotein 2 after laser irradiation in murine bone marrow cells culture by quantitative RT-PCR and did not demonstrate any significant differences between laser and control expression patterns.
The methodology employed in this study is aligned with previous reports found in the literature. 35,36 The model of bone defects has been used by many authors. 36 –38 It was found that the dose of the laser used had a positive result on bone metabolism at the site of injury. It is possible to find in the literature a wide range of fluencies and wavelengths of laser irradiation used by different authors on bone healing and fractures. Some authors suggested that doses among 1–5 J/cm2 induce stimulatory effects on both bone and soft tissues. 7 Others state that a total dose per session of 16 J/cm2 is more effective to induce positive effects on bone metabolism. 28 Moreover, some reports have suggested higher doses. 38 Because of this controversy, it is not possible to determine an ideal protocol of treatment yet.
The results of this work highlight the stimulatory effects of laser therapy on bone healing. Such findings would allow us to obtain relevant data on the potential efficacy of this therapy as an effective treatment for non-unions fractures or pseudoarthrosis. However, the reasons for the stimulatory effects of LLLT and the suite of parameters to be used in clinical therapies warrant further investigation.
Conclusion
The present study has demonstrated positive effects of LLLT on bone repair as depicted by histopathological and gene expression analysis, mainly at intermediary (13 days) and late periods (25 days) after bone injury.
Despite these results, further investigation is required to study other possible response mechanisms that may explain the positive effects of the LLLT on bone tissue. Such future studies will undoubtedly contribute to a better understanding of the safety of laser therapy and to design future research strategies in humans.
Footnotes
Author Disclosure Statement
No competing financial interests exist.