Objective: Bleeding control is a major concern during dental surgery. A novel photocoagulation method using an irradiating blue-violet light emitting diode (LED) was investigated. Background: Some dental light-curving units can emit blue-violet wavelengths around 380–515 nm with two peaks (410 nm and 470 nm). These wavelengths can cover the maximum absorption spectra of hemoglobin (430 nm). Materials and Methods: Blue-violet LED 380–515 nm, 750 mW/cm2, 10 sec (7.5 J/cm2) was used. Irradiation was performed for 10 sec or an additional 10 sec for 10 cases of tooth extraction at a distance of 1 cm from the socket. Bleeding was stopped by conventional roll pressure in another five cases as a control. Bleeding time for both procedures was measured. A Mann–Whitney U test was used for statistical analysis. In vitro transmission electron microscope (TEM) studies were performed to clarify the mechanism of hemostasis by blue-violet LED irradiation. Results: Irradiation with the blue-violet LED yielded immediate hemostasis of the socket. Five cases showed coagulation within the first 10 sec, and another five cases required an additional 10 sec to fully control the bleeding. In contrast, the conventional method required 2–5 min (median 180 sec) to obtain hemostasis. The difference between the time required to stop the bleeding in the two methods was found to be statistically significant (p = 0.0014). A week later, the LED-irradiated sockets were healed uneventfully with epithelial covering. TEM showed the formation of a thin amorphous layer and an adjacent agglutination of platelets and other cellular elements under the layer at the interface of the irradiated blood. Conclusion: Blue-violet LED irradiation of bleeding sockets caused immediate clot formation and hemostasis. This procedure was safe and reliable and showed no adverse effects.
Introduction
Bleeding during or after tooth extraction, oral surgery, and gingivectomy is a commonly observed clinical complication causing intraoperative and postoperative problems.1 Many wounds are left open after these procedures. Normally a roll pressure dressing is recommended for these cases. Although these procedures are routinely performed, operators sometimes encounter a troublesome hemorrhage from the resulting lesions. Here, we describe a simple and novel method for stopping the bleeding via photothermal interactions using blue-violet wavelengths.
A curing light emitting diode (LED) that emits specific wavelengths (380–515 nm) with two dominant peaks at approximately 410 and 470 nm is commercially available for the polymerization of composite resin for caries decay.2,3 This tool becomes a key to an initiator such as camphorquinone and lucirin® (diphenyl phosphine oxide), and the catalyst packages of composite resin. The visible blue-violet wavelengths emitted by this LED are used for composite photopolymerization and are also selectively absorbed by red blood cells, which are primarily composed of hemoglobin.4,5 Extraction sockets are generally filled with blood that contains strongly light-absorbing hemoglobin. The absorbing hemoglobin transforms the light into heat energy on the bleeding surface. This mechanism was applied to achieve photocoagulation of socket bleeding with very short LED irradiation. This is the first report that investigates the mechanism of stopping oral bleeding using a blue-violet LED light.
Material and Methods
LED irradiation
The conditions of LED irradiation used in this study were the following:
Blue-violet LED 380–515 nm.
Power output at the light-guide tip: 942 mW.
Continuous output.
Light guide aperture: 1 cm in diameter (0.785 cm2).
Output power measured on a power meter at 410 nm (Nova, Ophir, North Andover, MA) showed approximately 750 mW/cm2 at a distance of 1 cm from light emitter aperture.
Irradiation area: approximately 1.25 cm2.
Irradiation time of 10 sec equals energy 50 joules and an energy density of 7.5 J/cm2.
Irradiation time of 20 sec equals energy 100 joules and an energy density of 15 J/cm2.
Fifteen patients participated in the clinical trials. The treatment protocol was accomplished in agreement with the Helsinki Declaration. The reason for the LED irradiation was explained to the patients, and written informed consent was obtained from all patients with their signature. The ages of the patients ranged from 35 to 85 years. The reasons for extraction were advanced caries, tooth fractures, periodontitis, and apical periodontitis. These clinical data are shown in Table 1. Exclusion criteria were as follows: (a) patients under 18 years old; (b) pregnant women; (c) patients who received anticoagulation medication, and (d) patients with systemic bleeding disorders. Extraction was performed under local anesthesia (ORA® Inj. Dental Cartridge, Showa Yakuhin, Tokyo Japan). After the extraction of the tooth, granulation tissues were thoroughly eliminated by curettes. The extraction sockets were not sutured.
Patient Conditions for Tooth Extraction and Bleeding Time After Blue-Violet LED Irradiation or Cotton Roll Pressure (Control)
Patient no.
Name
Age
Sex
Reason for extraction
Extraction region
Bleeding time (sec)
Blue-violet LED irradiation
1
S. K.
45
F
Caries
Left upper second premolar
10
2
O. U.
38
F
Apical periodontitis
Left upper first incisor
10
3
O. A.
61
M
Periodontitis
Left upper first molar
10
4
S. M.
65
M
Periodontitis
Left lower first molar
20
5
M. K.
60
F
Periodontitis
Left lower first molar
10
6
Y. U.
25
F
Pericoronitis
Right upper third molar
10
7
M. K.
60
F
Apical periodontitis
Left lower first molar
20
8
K. S.
79
F
Apical periodontitis
Left lower first premolar
20
9
N. F.
75
F
Apical periodontitis
Right upper first molar
20
10
T. D.
35
M
Tooth fracture
Left lower second molar
20
Cotton roll pressure
11
S. Y.
85
F
Tooth fracture
Left upper first molar
125
12
S. M.
61
M
Periodontitis
Right upper second premolar
300
13
T. M.
77
F
Periodontitis
Right upper second molar
210
14
S. N.
41
M
Apical periodontitis
Left upper canine
180
15
I. K.
55
F
Apical periodontitis
Left upper central incisor
150
An operator irradiated the bleeding socket with LED light from a distance of 1 cm by the same manner for light-curing composite resin without touching to the surgical area. The LED irradiation was performed on 10 patients over the extraction socket for 10 sec and an additional 10 sec when bleeding continued. Another 5 patients were treated by conventional cotton roll pressure to stop the bleeding as the control. Bleeding time for both procedures was measured. Bleeding time was defined as the length of time for bleeding to cease from the extraction socket after gentle wipe with a piece of gauze. The extraction socket was photographed before and after the irradiation. One week later, the extraction sockets were re-examined to confirm the healing process.
As a nonparametric analysis, the Mann–Whitney U test was employed for statistical analysis comparing bleeding time between LED irradiation and the conventional method.
In vitro experiment
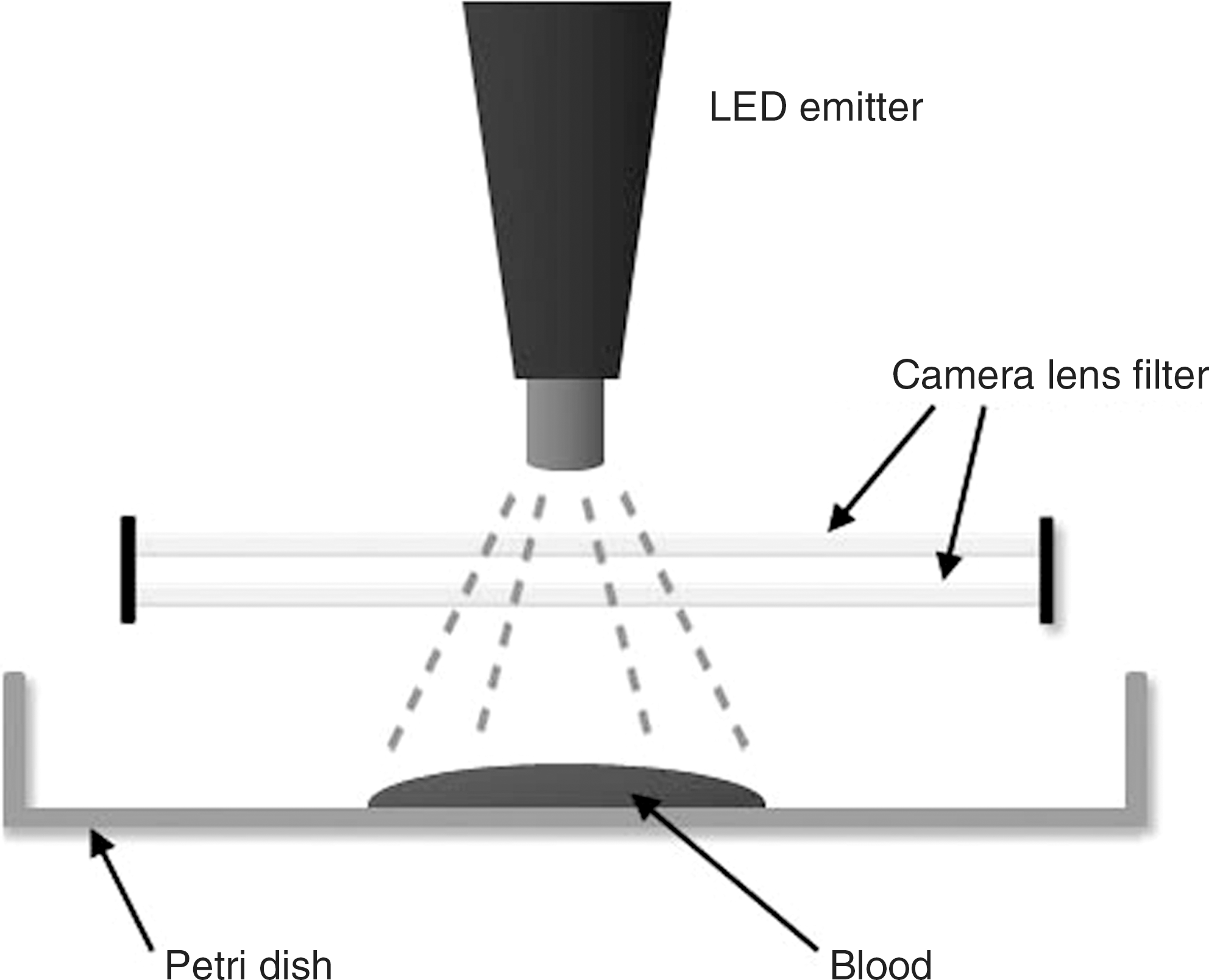
The structures of blue-violet LED-generated coagula were investigated using an electron microscope. A small amount of venous blood was obtained from two volunteers. Thin specimens were prepared by placing undiluted blood in a Petri dish, and the exposed blood was irradiated with the blue-violet LED emitter for 10 and additional 20 sec at a distance of 1 cm from the blood surface. Two pieces of camera lens filter (Kenko HC SKYLIGHT IB) were placed between the blood and the emitter to diminish the influence of the direct heating from the LED emitter as shown Fig. 1. Only the effect of the blue-violet wavelengths on the blood surface was analyzed.
Schematic illustration of blue-violet LED irradiation to the blood in vitro. The LED irradiated the blood surface through two camera-lens filters.
Transmission electron microscopy (TEM)
Irradiated and nonirradiated coagula were fixed with 2.5% glutaraldehyde in 0.1 M PBS for 2 h. The samples were washed overnight at 4°C in the same buffer and then postfixed with 1% OsO4 buffered with 0.1 M PBS for 2 h. The coagula were dehydrated in a graded series of ethanol and embedded in EPON 812. Semi-thin (1 μm) sections for light microscopy were collected on glass slides and stained for 30 sec with toluidine blue. Ultra-thin (90 nm) sections were collected on copper grids, double-stained with uranyl acetate and lead citrate, and then examined by transmission electron microscopy (H–7100, Hitachi, Hitachinaka, Japan).6
Results
Irradiation with the blue-violet LED caused almost immediate hemostasis of the socket bleeding in all cases. Five cases showed hemostasis within the first 10 sec, and another five cases required an additional 10 sec to control the bleeding. Thus, hemostasis occurred at 15 sec on average after the blue-violet LED irradiation (Table 1). The blood clot was observed to cover the socket as if a pudding with a shiny surface. Figures 2A and B show a case before and after blue-violet LED irradiation over the bleeding socket. In contrast, the conventional cotton pressure method required 2–5 min (median 180 sec) to obtain hemostasis, and the clot surface was depressed (Table 1). The difference in bleeding time between the LED irradiation method and the conventional method was clearly shown and was statistically significant (p = 0.0014).
(A) Photograph of extraction socket just after the extraction of the mandibular left second molar with obvious bleeding (mirror image). (B) Photograph of extraction socket [the same socket as in (A)] after LED irradiation (20 sec). The bleeding socket was controlled by blood coagulation with a shiny surface (mirror image). (C) Photograph of extraction socket [the same socket as in (A)] a week later. The extraction socket was covered with epithelium (mirror image).
One week later, the LED irradiated sockets were healed uneventfully, and an epithelial covering over the sockets was observed (Fig. 2C).
In vitro LED irradiation
We confirmed that the insertion of two pieces of lens filter between the LED emitter and the blood surface largely diminished direct heating from the LED emitter without reducing power fluence on the surface of the blood. We observed that the inner surface of the lens filter facing the blood surface was clouded with steam from the blood during LED irradiation even though the temperature of the whole area did not increase rapidly. This indicated that the photothermal interaction at the interface of the irradiated blood surface occurred as vaporization and superheating of the blood fluid.
Transmission electron microscopy
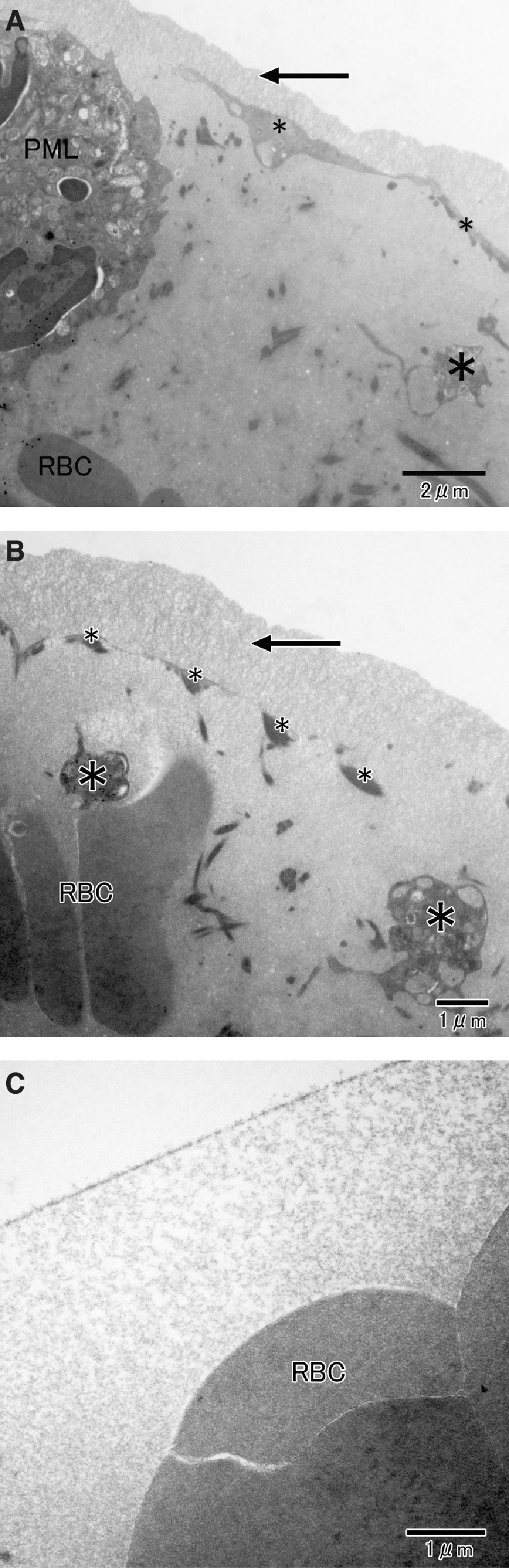
As shown in Figs. 3A and B, blue-violet LED irradiated blood formed a thin layer (about 50–1500 nm) of an amorphous structure at the interface of the blood clot. The layer seemed to consist of denatured plasma proteins. Beneath the layer, many platelets and other cellular elements agglutinated adjacently as if they supported the layer and formed blood clots. Under these structures, various blood cells, including red blood cells, appeared to keep their normal structure. Some leukocytes appeared to approach the interface border in comparison to nonirradiated samples. This unique structure seemed to contribute to form coagulum and hemostasis. Nonirradiated blood specimens were found to have no such a structure (Fig. 3C).
(A) TEM micrograph of the LED irradiated blood surface showing the amorphous layer (arrow) formed by photothermal interaction with the blue-violet LED. Beneath the layer, many platelets (small *) and various cellular elements (large *) agglutinated in alignment with the layer and seemed to form a blood coagulum. A polymorphonuclear leukocyte (PMN) appeared close to the interface. Under these structures, red blood cells (RBC) appeared to maintain relatively normal morphologies (bar = 2 micrometers). (B) TEM micrograph of the LED-irradiated blood at a higher magnification of the interface of the blood which consisted of an amorphous layer (approximately 1500 nm showing by arrow) made by photothermal interaction. Platelets (small *) and other cellular remnants (large *) are lined with the layer (bar = 1 μm). (C) TEM micrograph of a nonirradiated blood surface. The amorphous layer was never observed. Microfibrinous structures and red blood cells (RBC) were observed.
Discussion
Blue-violet LED irradiation immediately controlled socket bleeding in this preliminary clinical trial. As shown in transmission electron microscope photographs, a thin layer composed of an amorphous structure and agglutinated platelets was formed at the interface of the irradiated blood. This might occur as a photothermal interaction that clinically manifested as vaporization and superheating of the blood. Blood fluid and cells under the layer appeared intact. This process of coagulation was different from the nonirradiated coagulation process.
Coagulation, which involves platelets and coagulation factors, proceeds by a complex cascade to form fibrin crosslinks.7,8 To date, various materials, such as hemostatic gauze, gel foam, and collagen, have been used to help stop bleeding.1 These products are known to enhance or promote hemostasis and help coagulation by enhancing platelet aggregation. Electrocautery has also been an accepted method for controlling hemorrhage. However, if the electrocautery point touches the bone, severe damage occurs, leading to necrosis and the sequestration of bone tissue for an extended period of time.9 Similarly, various hard lasers are used for soft tissue incision and ablation because of their excellent cutting and hemostatic effects.10,11 Nd:YAG, CO2, and diode lasers are commonly selected for these purposes. These lasers, however, are also known to cause thermal damage to the underlying bone and to produce carbonization when they irradiate the bone directly.10,12
In contrast, the coagulation of tissue using a laser is called laser photocoagulation and employs visible blue light that is selectively absorbed by hemoglobin and melanin. Laser photocoagulation therapy is used to treat a number of eye diseases, such as retinal detachment and abnormal blood vessels in the retina.13,14 Condensation of protein materials by the controlled use of intense light energy produces the destruction of abnormal tissues and forms adhesive scars, especially in ophthalmology. Clinical and structural changes in blood treated with laser photocoagulation were reported by Black and Barton.15 They proposed a three-stage mechanism for coagulation involving a heating phase, a primary coagulation phase involving spherocytes and met-hemoglobin formation, and a secondary coagulation phase involving spherocyte rupture and extended coagulum formation. Our results tended to follow a similar mechanism, but the interaction was much milder. Only the surface interaction was clearly observed. The inside of the coagulum seemed to remain intact without causing such spherocyte rupture or extended coagulum formation.
The high financial cost of the laser apparatus is a barrier for its application in dentistry. In addition, as the laser beam is composed of a collimated light source, permanent damage to the eyes can occur if no special care is taken during laser manipulation.16 Recently, high-power LEDs have become available in dental clinics for the photopolymerization of composite resin fillings. The output power of LEDs has been enhanced as a new light activator, and LED devices are easily handled due to their compact size and are less expensive. In this preliminary clinical trial, a blue-phase G2 device was used because it emits a wide range of blue-violet specific wavelengths (380–515 nm) corresponding the absorption spectrum of hemoglobin (430 nm) and shows a power density high enough to cause photocoagulation. Hemoglobin has primary and secondary peak absorption spectra at around 430 and 555 nm, respectively, though the spectra show variation depending on oxygen binding.17 Other LEDs with similar characteristics also can be used for immediate hemostasis and blood clotting. Most importantly, LED application is less harmful to the eyes than lasers. After being exposed to LED blue-violet light, dental composites polymerize and harden into a solid filling. However, it is known that the light is often unable to penetrate more than 2–3 mm into the composite.18,19 Thus, LED irradiation of a bleeding socket was hypothesized to interact with blood within the surface area, causing absorption and scattering and resulting in the surface condensation of proteins including hemoglobin, followed by coagulation. Otherwise, LED irradiation never causes adverse effects to the surrounding tissues; blue-violet LED irradiation has been performed regularly to restore cervical caries lesions where marginal gingiva is adjacent. Thus, harmful effects and complications to the host tissue should be minimal. The precise mechanism of hemostasis by LED irradiation is under investigation using electron microscopy. Because this photocoagulation by blue-violet LED was simple, safe, and reliable, it may be applicable in clinics as an alternative or adjunctive form of hemostasis with or without conventional homeostatic gauze and gel foam, especially in difficult socket-bleeding cases.
LED application has the potential to benefit periodontal photoengineering and bone repair processes. In our study, blood clots filled the extraction socket when the LED was irradiated. The LED method seemed to provide a better coagulum filling than conventional pressure dressing. This better coagulum formation may result in early tissue repair with minimal alveolar bone resorption. The longitudinal healing process of the extraction sockets following blue-violet LED irradiation is under investigation. Thus, LED photocoagulation may produce not only rapid hemostasis, but also the acceleration of periodontal tissue healing. Pinheiro and Gerbi20 reviewed the recent studies of photoengineering of accelerated bone repair processes by low-level laser irradiation and mentioned that fibrin on a coagulum would act as a framework for cell migration during bone healing.
Based on these findings, it seems possible that the role of photomedicine, including photoengineering, will be recognized and applied in oral treatment in the near future.
Conclusion
A blue-violet LED (380–515 nm/750 mW/cm2) was applied at a distance of 1 cm over extraction sockets in 10 cases. In another five cases, bleeding was stopped by a conventional roll pressure method as the control. Immediate hemostasis of socket bleeding with LED irradiation was observed, in contrast to much slower hemostasis by the roll pressure method. This difference was statistically significant. One week later, healing had occurred uneventfully following both methods. Thus, the blue-violet LED irradiation method was simple, safe, and reliable for the coagulation and hemostasis of socket bleeding.
Footnotes
Acknowledgments
The authors would like to thank Dr. Norio Ueno and Ms. Fumie Furukawa for their kind contributions in preparing the manuscript, and Dr. Ryo Takagi for statistical analysis. The authors wish to thank Ivoclar Vivadent AG for providing the Bluephase G2 under investigation by our request. The authors obtained an understanding for the use of hemostatic purpose of this LED emitter with the company.
Author Disclosure Statement
The authors declare that they have no conflicts of interest, and no competing financial interests exist. This study was partially performed through the Formation of Innovation Center for Fusion of Advanced Technologies in the Special Coordination Funds for Promoting Science and Technology from Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan.
References
1.
KoernerK.R., McBeeW.L.2006. Management of Perioperative Bleeding. Manual of Minor Oral Surgery for the General Dentist. KoernerK.R.Oxford UK: Blackwell, 277–294.
2.
LeprinceJ., DevauxJ., MullierT., VrevenJ., LeloupG.2010. Pulpal-temperature rise and polymerization efficiency of LED curing lights. Oper. Dent., 35:220–230.
3.
IlieN., HickelR.2008. Can CQ be completely replaced by alternative initiators in dental adhesives?Dent. Mater. J., 27:221–228.
4.
MerrickM.F., PardueH.L.1986. Evaluation of absorption and first- and second-derivative spectra for simultaneous quantification of bilirubin and hemoglobin. Clin. Chem., 32:598–602.
IchinoseS., MunetaT., KogaH.et al.2010. Morphological differences during in vitro chondrogenesis of bone marrow-, synovium-MSCs, and chondrocytes. Lab. Invest., 90:210–221.
7.
ShapiroS.S.2003. Treating thrombosis in the 21st century. N. Engl. J. Med., 349:1762–1764.
8.
ColmanR.W., MarderV.J.J., ClowesA.W.2006. Overview of coagulation, fibrinolysis and their regulation. Hemostasis and Thrombosis: Basic Principles and Clinical Practice, 5thColmanR.W., ClowesA.W., GeorgeJ.N., GoldhaberS.Z., MarderV.J.Philadelphia: Williams & Wilkins, 17–20.
9.
YoshinoT., AokiA., OdaS.et al.2009. Long-term histologic analysis of bone tissue alteration and healing following Er:YAG laser irradiation compared to electrosurgery. J. Periodontol., 80:82–92.
IshikawaI., AokiA., TakasakiA.A., MizutaniK., SasakiK.M., IzumiY.2009. Application of lasers in periodontics: True innovation or myth?Periodontol. 2000., 50:90–1126.
12.
SasakiK.M., AokiA., IchinoseS., IshikawaI.2002. Ultrastructural analysis of bone tissue irradiated by Er:YAG Laser. Lasers Surg. Med., 31:322–332.
13.
OspinaL.H., LyonsC.J., MatsubaC., JanJ., McCormickA.Q.2005. Argon laser photocoagulation for retinopathy of prematurity: long-term outcome. Eye (Lond), 19:1213–1218.
14.
ChewE.Y., FerrisF.L.3rd., CsakyK.G.et al.2003. The long-term effects of laser photocoagulation treatment in patients with diabetic retinopathy: The early treatment diabetic retinopathy follow-up study. Ophthalmology, 110:1683–1689.
15.
BlackJ.F., BartonJ.K.2004. Chemical and structural changes in blood undergoing laser photocoagulation. Photochem. Photobiol., 80:89–97.
16.
MatthewsL., GarciaG.1995. Light Sources and Units. Laser And Eye Safety In The Laboratory. New York: IEEE Press, 15–26.
17.
MiserendinoL.J., LevyG., MiserendinoC.A.1995. Laser Interaction with Biologic Tissues. Lasers in Dentistry. MiserendinoL.J., PickR.M.Carol Stream IL USA: Quintessence Pub. Co, 30–55.
18.
TsaiP.C., MeyersI.A., WalshL.J.2004. Depth of cure and surface microhardness of composite resin cured with blue LED curing lights. Dent. Mater., 20:364–369.
19.
PriceR.B., FelixC.A., AndreouP.2004. Effects of resin composite composition and irradiation distance on the performance of curing lights. Biomaterials, 25:4465–4477.
20.
PinheiroA.L., GerbiM.E.2006. Photoengineering of bone repair processes. Photomed. Laser Surg., 24:169–178.