
Abstract
Introduction
The inflammatory response and cytokine release from the injured myocardium are essential components of the host response to MI. 7 –9 It has been well demonstrated that LLLI regulates the expression of cytokines after tissue damage and inhibits inflammation in many tissues. 10 –13 However, little is known concerning the alteration of the cardiac cytokine expression profile after LLLI. Antibody-based protein array technology has emerged as a powerful tool for protein profiling and candidate biomarker screening. This approach can allow for rapid high-throughput profiling of multiple proteins in a single sample and the detection of low-molecular weight biomarkers that are typically missed by other techniques. 14,15 In this study, with the aid of antibody-based protein arrays, we would like to address: (a) the expression of cytokines following MI with or without laser irradiation; and (b) the effect of LLLI on heart function and ventricular remodeling.
Materials and Methods
Animals
The study was performed in accordance with guidelines of the “Regulation to the Care and Use of Experimental Animals” (1996) of the Beijing Council on Animal Care. All experiments were carried out in accordance with the Ethics Committee for Animal Study in Fu Wai hospital. Female Sprague–Dawley rats (Vital River Laboratory Animal, Inc., Beijing, China) weighing 260–280 g were enrolled in this study. The experimental protocol is shown in Fig. 1.

Flow chart of the study protocol. MI, myocardial infarction.
Creation of myocardial infarction
Myocardial infarction was induced in the female rats by permanent ligation of the left anterior descending artery. 16 Briefly, the animals were anesthetized by intraperitoneal injection of 10% chloral hydrate (300 mg/kg body weight) and ventilated via oral intubation using a Harvard Rodent Ventilator (Model 683, Harvard Apparatus, Holliston, MA). The heart was exposed through a minimal anterolateral thoracotomy, and the left anterior descending coronary artery was ligated 3 mm distally from where it branches off the aorta. The surviving rats were randomly divided into laser (n = 33) and control groups (n = 33). Rats that received the same procedure of thoracotomy without coronary ligation served as the sham group (n = 28).
Laser irradiation
The laser device used in this study was A diode laser (KDL-300, Beijing KeDian Microwave Electronics Co., Beijing, China) with wavelength 635 nm, power 5 mW, CW, laser, beam spot size 0.8 cm2, irradiance 6 mW/cm2, irradiation time 150 sec, energy 0.8 J, and energy density 1 J/cm2. The laser beam was placed in contact with the myocardium surface corresponding to the infarction area. The LaserCheck energy meter (LM-91B, National Institute of Metrology, Beijing, China) determined the precise output of the equipment, and then the power was divided by the beam spot area 0.8 cm2 to calculate the power density. Laser irradiation was performed as described above about 5 min post-coronary artery occlusion. The optical fiber was fixed with a delivery arm and precisely positioned with the fiber tip 26 mm above the myocardium. This allowed for a laser beam spot size of 0.8 cm2. 17 Seventy-two hours after the initial laser irradiation, the rats were lightly anesthetized, the skin sutures over the chest were removed, and the intercostal muscles below were exposed to perform the additional irradiation whose parameters were the same as the initial laser irradiation. 5,6
Antibody array analysis for cytokines
One day after laser irradiation, 5 rats from each group were sacrificed and the hearts were harvested. The free wall of left ventricle was excised and the samples were homogenized with ice-cold protein extraction reagent containing protease inhibitors (Shanghai KangChen Bio-tech Inc, Shanghai, China). The amount of protein in each supernatant was determined by using a BCA Protein Assay Kit (Shanghai KangChen Bio-tech Inc.). A commercially available antibody array (Ray-Bio® Rat Antibody Array 1.1, RayBiotech Inc., Norcross, GA) for analysis of 19 rat cytokines was used for screening. The name and location of each cytokine in the array is listed in Table 1. Each membrane was placed into the provided 8-well tray, 2 ml blocking buffer was added, and the trays were incubated at room temperature for 30 min to block membranes. After incubating the membranes with 1 ml of sample at room temperature for 1–2 h, the membranes were then washed three times with wash buffer and incubated with biotin-conjugated antibodies containing blocking buffer at room temperature for 1–2 h. The membranes were washed again and incubated with horseradish peroxidase (HRP)-conjugated streptavidin at room temperature for 1 h and detection buffer for 2 min. Finally, the membranes were exposed to x-ray film and then the signals were detected.
CINC-2, CINC-3, cytokine-induced neutrophil chemoattractant 2 and 3; CNTF, ciliary neurotrophic factor; GM-CSF, granulocyte/macrophage colony-stimulating factor; IFN-γ, interferon γ; IL-1α, interleukin 1α; IL-1β, interleukin 1β; IL-4, interleukin 4; IL-6, interleukin 6; IL-10, interleukin 10; LIX, LPS-induced CXC chemokine; MCP-1, monocyte chemoattractant protein 1; MIP-3α, macrophage inflammatory protein 3α; β-NGF, β nerve growth factor; TIMP-1, tissue inhibitor of metalloproteinase 1; TNF-α, tumor necrosis factor α; VEGF, vascular endothelial growth factor.
By comparing the signal intensities, relative expression levels of cytokines can be evaluated. The intensities of signals can be quantified by the use of densitometry. Positive control can be used to normalize the results from the different membranes being compared. This allows the normalized intensity value of each cytokine in each group to be converted into the relative n-fold change. A 1.3-fold change in spot intensity compared to controls was considered as significant. 18
Enzyme-linked immunosorbent assay
After antibody array analysis, the significantly changed cytokines were identified. The expression levels of targeted cytokines were measured respectively with the ELISA kits (Rapid Bio Lab, Calabasas, CA) in accordance with the instructions of the manufacturer. The optical density was measured at a wavelength of 450 nm by a Model 680 Microplate Reader (Bio-Rad Laboratories, Hercules, CA).
Echocardiographic assessments
Transthoracic echocardiography was performed 2 weeks after MI (n = 10 in each group). 19 Parasternal long- and short-axis views were obtained with both M-mode and two-dimensional echocardiography images. As a measure of cardiac performance, left ventricular end-systolic (LVESd) and end-diastolic (LVEDd) diameters were measured. Left ventricular fractional shortening (LVFS) and ejection fraction (LVEF) were calculated as follows: LVFS(%) = (LVEDd-LVESd)/LVEDd × 100 ; and LVEF (%) = [(LVEDd3-LVESd3)/LVEDd3] × 100. Dimensions were measured just below the level of the papillary muscle. All measurements were averaged over three consecutive cardiac cycles and were analyzed by two independent experienced investigators who were blinded to the treatment status of the animals.
Cardiac morphometric evaluation
The infarct size, infarct wall thickness, and expansion index were measured after echocardiographic assessments. The hearts were excised and immediately soaked in cold saline for 10 sec to remove excess blood from the ventricles. The hearts were then fixed in 10% neutral buffered formalin for 48 h. Transverse slices (2.0–2.5 mm thick) from control and laser group were then prepared in a plane parallel to the atrioventricular groove and in the middle of the infarct. Infarct size was determined by histomorphometric methods. 20,21 Briefly, 8-mm thick serial sections were prepared and stained with hematoxylin and eosin (H&E). Infarct size was expressed as percentage area of the total area of the left ventricle using image-analysis systems (Olympus, Tokyo, Japan). The infarct wall thickness was determined in each section as the mean of three measurements of the middle and two lateral regions of the infarcted area in the LV. 4 Expansion index was calculated as previously described. 22,23
Statistical analysis
Comparisons between any two groups were evaluated using Student's t test. The differences among groups were tested by one-way analysis of variance (ANOVA) followed by the least significant difference (L.S.D.) test for multiple comparisons. Values were analyzed using the statistical package SPSS 13.0. (SPSS Inc., Chicago, IL) A value of p < 0.05 was accepted as statistically significant.
Results
Surgical mortality
As shown in Fig. 1, a total of 110 female rats were enrolled in this study; 16 rats died of fatal ventricular arrhythmia during the creation of MI. Additionally, 10 rats from laser and control group (n = 5, respectively) died within the first 24 h after MI. No more rats died after 1 day post-MI. These animals were excluded from the final analysis. No rats died in the sham group.
Cytokine antibody array analysis
As shown in Fig. 2, the levels of cytokine-induced neutrophil chemoattractant-3 (CINC-3), fractalkine, interleukin(IL)-10, leptin, tissue inhibitor of metalloproteinase- 1(TIMP-1), and VEGF in the control group were significantly upregulated compared with those of the sham group.

Typical images of rat cytokine antibody array. A total of 19 cytokines were placed on the array. Representative antibody arrays incubated with protein extraction from laser (
The density of granulocyte/macrophage colony-stimulating factor (GM-CSF) and IL-4 (0.38 and 0.28, respectively) in the laser group was higher than that of the control group (0.24 and 0.19, respectively), while the density of CINC-3 and fractalkine (0.24 and 0.10, respectively) was decreased compared with the density in the control group (0.36 and 0.14, respectively; Fig. 3).
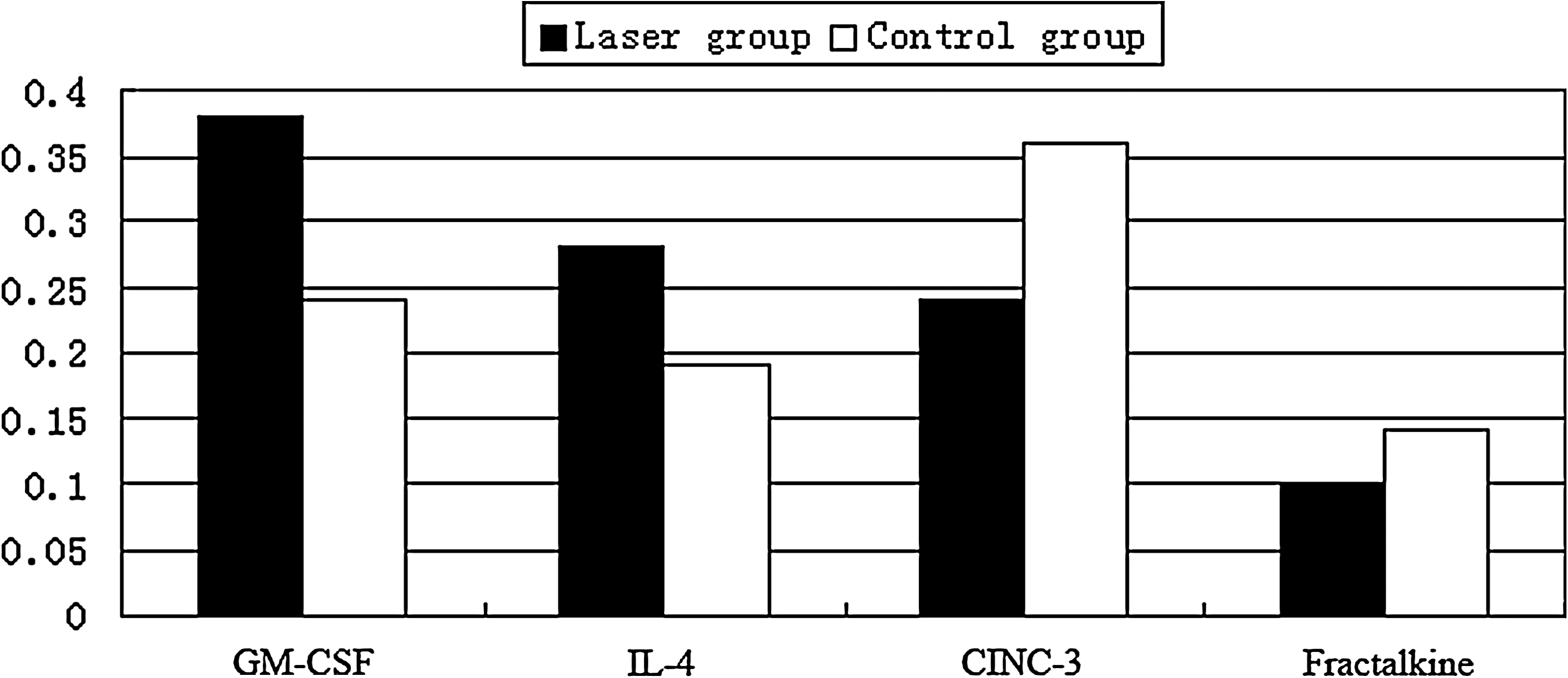
The density of cytokines in laser and control group. The data was expressed as the average of density of 5 samples from each group.
Confirmation of cytokine levels using ELISA
ELISA was applied to confirm the levels of CINC-3, fractalkine, GM-CSF and IL-4 in each group. As shown in Table 2, 1 day after LLLI, the level of fractalkine in the laser group was significantly lower than that of the control group (p = 0.033). The GM-CSF level in the laser group was significantly elevated when compared with that of the control group (p = 0.02). However, there were no significant differences in the levels of CINC-3 and IL-4 between the laser and control groups.
p < 0.05 vs. control group. b p < 0.05 vs. sham group. CINC-3, cytokine-induced neutrophil chemoattractant-3; FKN, fractalkine; GM-CSF, granulocyte/macrophage colony-stimulating factor; IL-4, interleukin-4.
All the four cytokines in the control group increased significantly compared with those of the sham group. However, at 2 weeks after LLLI, there were no significant differences among the three groups in cytokine expression.
Assessment of the heart function
The results of echocardiographic assessment at 2 weeks after laser irradiation are shown in Fig. 4. LVEF and LVFS in the control group (49.14 ± 6.93% and 21.72 ± 3.75%, respectively) decreased significantly compared to the LVEF and LVFS of the sham group (81.45 ± 4.66 and 45.15 ± 4.73, respectively; p < 0.01). Accordingly, LVEDd and LVESd in the control group (7.74 ± 0.67 and 6.16 ± 0.70 mm) were higher than that of the sham group (6.40 ± 0.52 and 3.51 ± 0.41 mm; p < 0.01). However, there were no significant differences in LVEF, LVFS, LVEDd, or LVESd between control and laser groups.
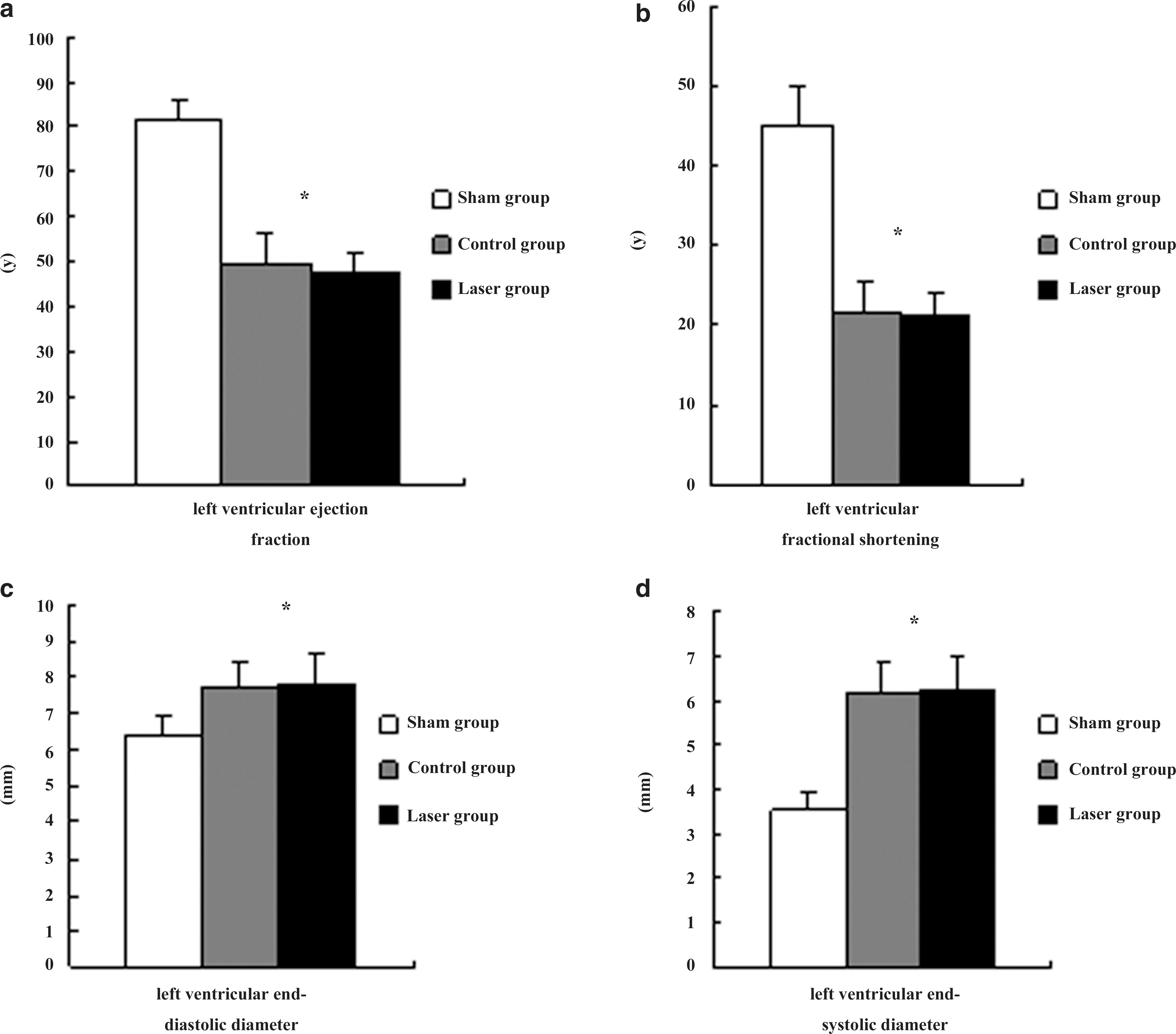
Evaluations of heart function and ventricular remodeling by echocardiography at 2 weeks after laser treatment. Compared with the sham group, the systolic heart function including ejection fraction (
Postmortem cardiac morphometric evaluation
At 2 weeks after MI, infarct sizes in laser group (37.0 ± 5.6%) significantly decreased compared with those of the control group (42.4 ± 5.0%; p = 0.034) (Figs. 5a, b, and c).
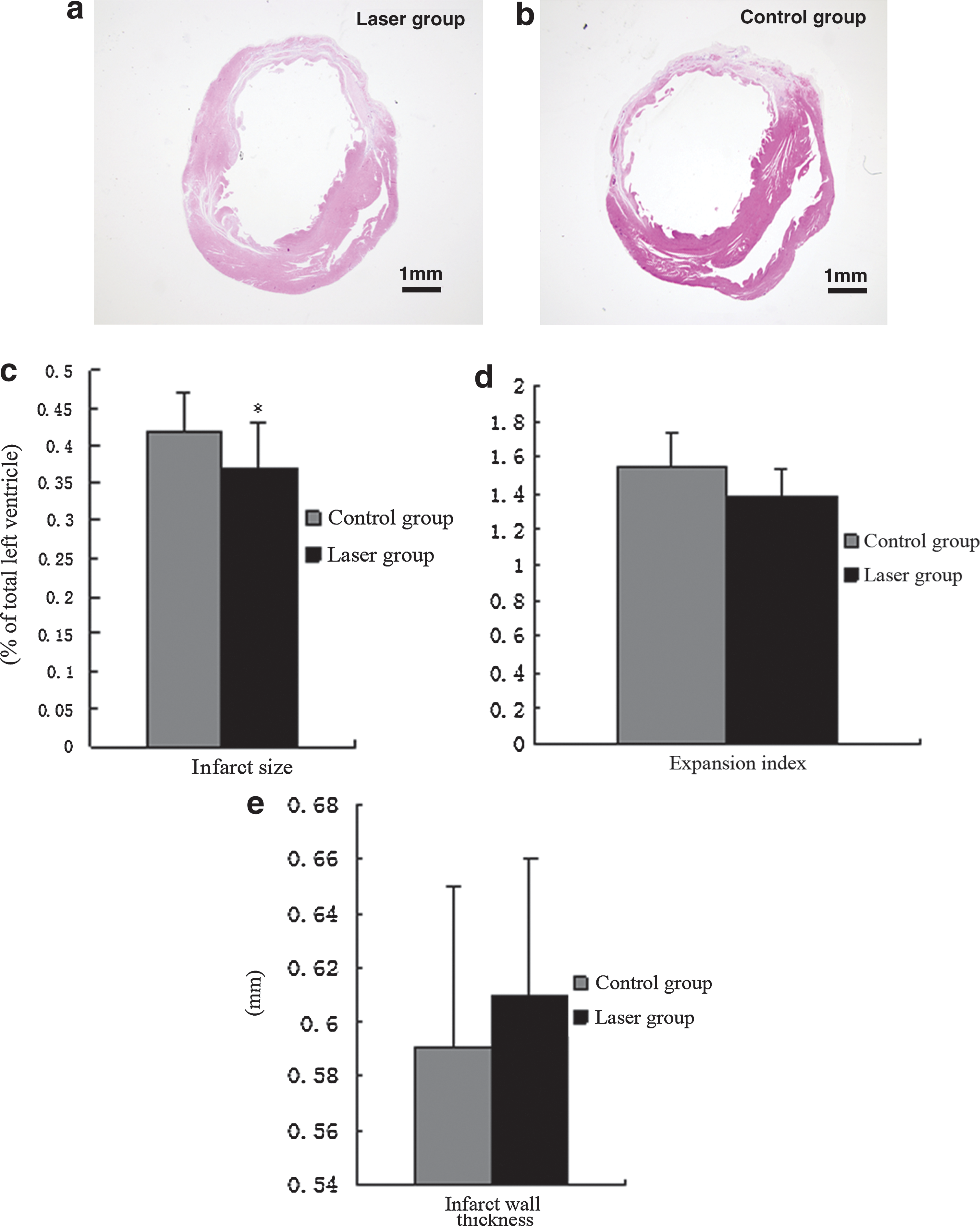
Typical light micrographs of cross sections of rat heart with (
Expansion index in the laser group tended to be lower than that in the control group (1.38 ± 0.16 vs. 1.55 ± 0.18, p = 0.057; Fig. 5d). The infarct wall thickness in laser and control group were 0.597 ± 0.052 and 0.608 ± 0.060 mm, respectively (p = 0.98; Fig. 5e).
Discussion
MI is the most common and clinically significant form of acute cardiac injury and results in ischemic death of a large number of cardiomyocytes. 24 Previous studies indicated that laser irradiation given at the proper power density and timing could limit the deterioration of cardiac function following MI. 5,6,25 However, little is known about the mechanisms associated with the cardioprotective effect following laser irradiation.
Ischemia-induced cytokine release plays a crucial role in inflammatory response for cardiac repair. Cytokine release following MI is involved in apoptosis, angiogenesis, cell growth, and differentiation. The interaction between cytokines and the ischemic injury is a dynamic process. The majority of released cytokines involved in ischemia-induced inflammation are upregulated during 1 day after MI. 26,27 Thus, we chose this time point to screen the alteration of cytokine expression after laser irradiation.
The major findings of the present study are that (a) LLLI regulated the cytokine expression of injured myocardium at early stage of MI. Laser treatment inhibited the expression of fractalkine but enhanced the GM-CSF expression in the myocardium; and (b) LLLI reduced the infarct area expansion. However, improved heart function was not observed at 2 weeks after laser treatment.
RayBio® Rat Cytokine Antibody Array study is the first commercially available cytokine protein array system. 28 –30 It can rapidly and accurately identify the multiple cytokine expression of various tissues. In our study, we used this technology to screen the alteration of the cardiac cytokine expression profile after laser irradiation. The results indicated that LLLI stimulated the production of GM-CSF, IL-4, and inhibited the expression of CINC-3 and fractalkine. In order to confirm the reliability of antibody array, ELISA was then performed to evaluate the expression of these four identified cytokines. The results showed that all the four cytokines in the control group increased significantly compared with the sham group. It is supported by other studies that a series of inflammatory responses, including chemokine release from the injured myocardium, would occur after MI. 7,8 Furthermore, upregulation of GM-CSF and downregulation of fractalkine in the myocardium were detected after laser irradiation at 1 day post-infarction.
GM-CSF was reported to mobilize bone marrow-derived stem cells to regenerate the damaged myocardium. 31 Furthermore, a recent clinical study 32 showed that short-term intracoronary and subcutaneous administration of GM-CSF could improve collateral flow in patients with coronary artery disease. LLLI has been shown to stimulate the expression of GM-CSF and thereby could augment the stem cell homing and collaterals formation for cardiac repair. Besides stem cell mobilization, Minatoguchi and co-workers reported that CSF may accelerate infarct healing by enhancing macrophage infiltration, matrix metalloproteinase activation, and cardiomyocyte apoptosis suppression by activating the cytoprotective transcription factor. 33 Fractalkine is involved in the pathogenesis of many inflammatory disorders and could induce leukocyte accumulation at inflammatory sites and modulate inflammatory activities via the recruited cells. 34 The upregulated fractalkine following MI is involved in myocardial remodeling and reduction of myocardial contractile function by dephosphorylation of phospholamban and reduction in SERCA activity. 35 The downregulation of fractalkine after LLLI treatment could decrease the leukocyte accumulation at the infarct sites and thereby alleviate the inflammatory activities following MI.
Although a repeated irradiation was performed 72 hours after initial irradiation, no further alteration in GM-CSF and fractalkine expression was observed at 2 weeks after MI. It indicated that the impact of LLLI on the release of cytokines vanished rapidly after irradiation. In our previous study, we also found that LLLI might not lead to stable and persistent cardioprotective effects. 17 Hence, a new irradiation protocol should be developed to amplify the beneficial effects of LLLI therapy.
Safavi and co-workers observed that LLLI inhibited the gene expression of interleukin-1β (IL-1β) and interferon-γ (IFN-γ) in a inflamed gingival mode. 12 In a rat carrageenan-induced pleurisy model, Boschi and associates demonstrated that LLLI induced an anti-inflammatory effect characterized by inhibition of IL-6, monocyte chemoattractant protein-1(MCP-1), IL-10, and TNF-a. 11 Our cytokine antibody array covered all the above cytokines; however, we did not detect any alteration of these mentioned cytokines. Therefore, we presumed that the protective effect of LLLI might be a tissue-specific feature.
We also found LLLI resulted in a significant reduction of infarct size. Unfortunately, no statistically significant improvement of heart function was observed in our study. It indicated that the effect of LLLI is moderate and the surviving cardiomyocytes still could not completely recover from the ischemia-induced injury. Our findings are mainly in agreement with previous study by Oron 5 who observed that LLLI reduced the infarct size in dogs. In Oron's study, infrared laser with 803 nm wavelength were used. The red laser, which we applied in the present study, might penetrate to a lesser extent in the myocardial tissue even of the rat and therefore not an optimal effect is achieved. But F Lin 36 indicated that the effects of LLLI therapy are not through induction of thermal effects but rather through a process that is still not clearly defined called “photobiostimulation”. This effect of LLLI is not dependent on coherence. In a future study, we plan to apply a new laser resource and a comprehensive strategy to join LLLI and other approaches, including stem cell transplantation and direct cytokine injection, to achieve satisfactory restored heart function.
Conclusions
In the present study, the antibody-based protein array technology was applied for screening the cytokine expression profile following MI, with or without laser irradiation. The present study indicates that LLLI has a protective effect on the injured myocardium by upregulating GM-CSF and downregulating fractalkine during the acute phase after LLLI. In a future study, we will apply the whole proteome analysis to analyze the alteration of more cytokines involved in inflammation at various points in time after laser irradiation. The cytokine expression profile after laser irradiation offers a potential novel mechanism for the use of laser therapy in the treatment of heart disease.
Footnotes
Acknowledgments
This study is supported by the Natural Science Foundation of China (81070099) and Fok Ying-Tong Education Foundation (121041). The authors thank Mr. Jacob Bauer from Vanderbilt University, Nashville, Tenn. for his excellent language editing.
Author Disclosure Statement
All the authors have no competing financial interests to disclose.