
Abstract
Introduction
Malignant transformation seems to be more likely in erosive lesions, possibly due to the exposure of the deeper epithelial layers to oral environmental carcinogens. 4
Oral lesions of OLP are difficult to control and are often refractory to conventional therapies. 4 Traditional treatment consists of various medical therapies. Topical corticosteroids are widely accepted as the primary treatment of choice. 5 The greatest disadvantage of topical therapy for OLP lesions is the lack of sufficient mucosal adherence. In addition, one-third of OLP patients treated with topical corticosteroids develop secondary candidiasis which mandates to be treated. 6,7 Another disadvantage of prolonged use of these drugs is tachyphylaxis, a decrease in their biological effectiveness. 8
By considering the resistance to topical treatments in some patients and other disadvantages, looking for an alternative effective treatment with minimal side effects seems to be necessary. 9,10
The aim of our study was to compare the effect of low intensity laser therapy (LILT) (630-nm diode laser) versus topical corticosteroids in the treatment of oral erosive and atrophic lichen planus.
Materials and Methods
Thirty adult patients with atrophic-erosive biopsy-proven OLP in the tongue or buccal mucosa, sized ≤3 cm, attending the Department of Oral Medicine (Mashhad Dental Faculty) between April 2008 and March 2009 were randomly allocated into an experimental (laser treated) and a control group (corticosteroid treated).
Patient exclusion criteria included those presenting with systemic diseases, drug consumption, pregnancy, photosensitivity, patients younger than 20 years, and patients who had lesions with dysplasia or had received treatment for OLP at least 1 month prior to the beginning of our study. Lesions adjacent to the amalgam filling site were also not eligible for the study. The study protocol was approved by the Institutional Ethics Committee (IEC) of Mashhad University, and each subject signed a detailed informed consent form.
Patients in the experimental group were treated by laser irradiation (exposure time, 2.5 min; fluence 1.5 J/cm2 per session; irradiance 10 mW/cm2; one illumination point; area 1cm2). A diode laser was used as a light source (Mustang 2000+, Russia, KLO3 probe, 630 nm, 10 mW, continuous wave, spot size: 1 × 1 cm). Irradiation was done two times a week (once every third day) for a maximum of 10 sessions.
Patients in the control group were treated by local corticosteroids consisting of dexamethasone (0.5 mg in 5 ml water) mouth wash for 5 min, followed 30 min later by a mouth rinse with 30 drops of Nystatin (100,000 units) for 5 min. This treatment was repeated four times a day for one month and patients were followed up weekly during this period.
The patients' pain experience was measured by means of the visual analogue scale (VAS), as follows: Score 3 = 7 < VAS ≤10; Score 2 = 3.5 < VAS ≤7; Score 1 = 0 < VAS ≤3.5; Score 0 = no pain. 11
Reduction in sign scores was assessed by Thongprasom sign scoring as follows: 12 score 5 (white striae with erosive area = 1 cm2), score 4 (white striae with erosive area <1cm2), score 3 (white striae with atrophic area >1 cm2), score 2 (white striae with atrophic area <1 cm2), score1 (mild white striae only), score 0 (no lesions, normal mucosa). The size of the lesions was determined by using a culis. The severity of the lesions in each site was recorded based on the presence of reticular/hyperkeratotic, atrophic, or erosive/ulcerative lesion (s). For patients with more than one lesion, a sign score was derived by summation of the scores of all four areas (right and left buccal mucosa, right and left border of the tongue).
Reticular score = ΣR, Atrophic score = ΣA, Erosive/ulcerative score = ΣE (RAE score) with a total weighted score of Σ (R × 1) + Σ (A x 1.5) + Σ (E × 2.0). 13 In order to determine the efficacy indices (EI) of the treatment (improvement of lesions), the following formula was used: [100% × (Total score of lesion before treatment-Total score of lesion after treatment)]/Total score of lesion before the start of treatment.
The EI were evaluated on a 5-rank scale: 14 Healed: EI = 100%; Marked improvement: 75% ≤EI < 100%; Moderate improvement: 25% ≤EI < 75%; Mild improvement: 25% < EI < 0; No improvement = 0.
Each subject was evaluated weekly for improvement rate and adverse effects during the time of treatment and then was followed up 3, 6, and 12 months after completion of treatment to evaluate any relapse. Data were analyzed using SPSS version 15 (SPSS Inc., Chicago, IL). We have used descriptive statistics including mean, median, standard deviation (SD), and also inferential statistics including Chi-square, Mann–Whitney, Student's t-test, Fisher's exact and Wilcoxon tests.
Results
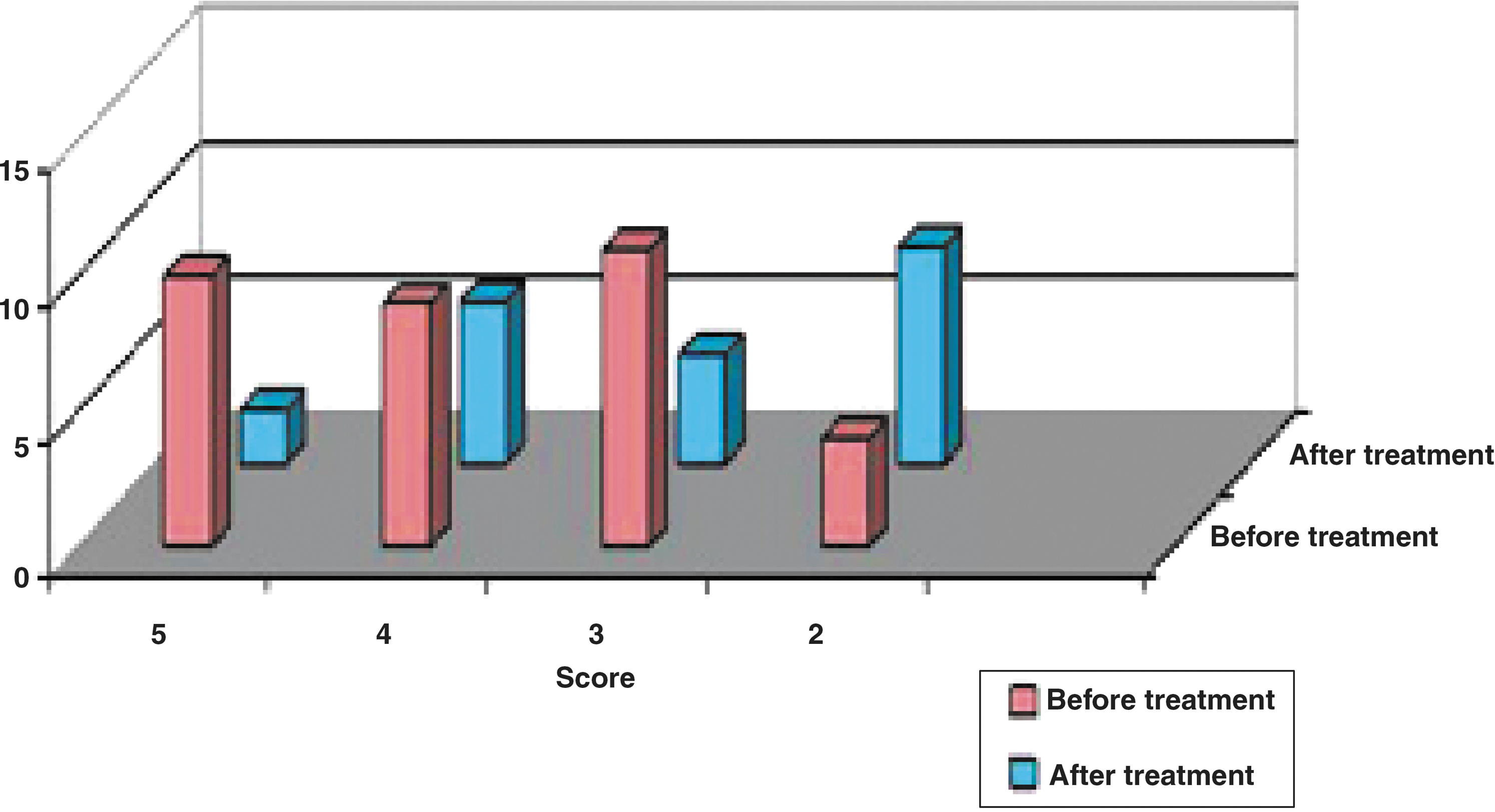
Six of thirty patients who were initially selected for this study were excluded because they discontinued the treatment between sessions. Statistical analysis showed no significant difference between the two groups regarding gender representation, age, marital status, and duration of disease before our treatment, location of the lesions, or previous treatments. The Mann–Whitney test showed no significant difference in sign score changes between the two groups before and after treatment. (Figs. 1 and 2)

Sign score of OLP lesions in experimental group.
Sign score of OLP lesions in control group.
There was no statistically significant difference in clinical severity between the two groups based on Student's t-test. Although the sign scores decreased in almost all scoring groups of the experimental (P = 0.006) (Fig. 1) and control (P = 0.007) patients (Fig. 2), they were not statistically significant (Table 1).
Symptom improvement was achieved after treatment in either group (P < 0.001); however, paired t-tests and Mann–Whitney tests showed no significant statistical difference between these two groups (Table 2). Efficacy indices were more than 75% in 36.4% of the experimental group and 38.5% in the control group, indicating a similar level of improvement between the two groups (Table 3). Fifty percent of the experimental group and 40% of the control group did not show any relapse at follow up sessions, with no statistical difference between the two groups.
There were no serious intra- or postoperative complications in the experimental patients and we did not observe any other side effects during the follow-up period.
Discussion
The results of our study demonstrate that LILT is as effective as topical corticosteroid treatment for OLP. (Figs. 3 –5). Although LILT has been used for more than three decades in health care studies, its mechanism of action on inflammation is complex. 15

Clinical view of the buccal lesion before treatment.

Clinical view of the buccal lesion after three sessions of laser treatment.

Clinical view of the buccal lesion after five sessions of laser treatment.
It has been shown that LILT causes vasodilation and increases local blood flow which brings in oxygen and makes a greater movement of immune cells into the tissue. 16 Modulation of mast cell functions by LILT is important in control of inflammation in the oral cavity. Increased proliferation, maturation and migration, as well as transformation to myofibroblasts, a decreased production of pro-inflammatory prostaglandin E2, and increased production of basic growth factors have also been noted in LILT. 17
By considering the inflammatory pathogenesis of OLP, LILT may be an effective means of treatment. Wavelength is the most important factor in all types of phototherapy, and the best wavelength should be selected to obtain the best results. The extensive penetration of red and near-infrared light into tissues has been well documented. 16,17
Earlier studies examining the effect of low intensity lasers on OLP used excimer lasers (308 nm) which are in the ultraviolet area of electromagnetic waves with low penetration depth and carcinogenic effects. 15 Here, we used the 630 nm laser because it is one of the most effective wavelengths for wound healing. 18 In addition, no side effects have been reported in treatments using this wavelength. 16 –18
The results of earlier studies that used excimer lasers were disappointing. Passeron et al. used excimer lasers (308 nm) on 4 patients with OLP. 19 Kollner et al. also studied the effect of excimer lasers on 8 patients with OLP, and only one patient responded completely after 12 sessions. 20 In a study by Trehan et al., an excimer laser was used in eight patients with OLP who had previously failed to respond to traditional treatment and five patients improved more than 75%, 21 although the number of sessions was more than in the study of Kollner and Passeron. 19,20
In the experimental laser group, 63% of patients had more than 50% improvement of their lesions. Only one patient, who had severe psychological problems, had no change in her lesions. Stress has been considered as the most frequent cause of acute exacerbations in OLP patients. 22,23 While a double blind placebo control study (using a probe without emission as placebo) may have been equally or more informative, it would be unethical to deprive patients who are looking for a treatment for their painful lesions. Although our sample size was small, it seems that 630 nm LILT was as effective as and comparable with topical corticosteroid therapy in the treatment of OLP, and in long term follow-up, even, showed better results. In addition, LILT did not exhibit unwanted side effects. Based on these results, more detailed randomized controlled trials are needed.
Footnotes
Acknowledgments
The authors would like to extend their appreciation to the vice chancellor for research, MUMS (Mashhad University of Medical Sciences) for the financial support. “The results described in this paper was part of a (MSD) student thesis proposal”
Author Disclosure Statement
No competing financial interests exist.