
Abstract
Introduction
The loss of a random skin flap can be attributed to extrinsic and intrinsic causes. The extrinsic ones include some that are systemic (arteriosclerosis, hypotension, infections, and malnutrition), local conditions (compression, tension, and flap angle) and techniques (planning failure). These causes can be generally controlled through adequate pre- and postoperative care. In contrast to the plurality of such extrinsic factors, the main intrinsic factor is known to be the inadequate blood flow in flaps. This complication can be explained by the section of the skin vessels and the sympathetic nerve terminals caused by flap elevation, which could reduce its blood flow. 4
Knowing the extrinsic and intrinsic factors that lead to the flap loss, and in an attempt to perform the skin flaps with more safety, some researchers began to study the techniques related to the increase of blood supply, in order to minimize the ischemic condition, and thereby increase the area viability and possible coadjuvant in the skin flap survival.
According to the literature, some researches use different types of drugs: vasodilators, calcium channel blockers, prostaglandin inhibitors, anticoagulants, antiadrenertics, and antioxidants; 5 –7 however some of these drugs can trigger some unexpected systemic effects and are therefore not recommended for clinical practice.
Other research using nonpharmacological resources, such as acupuncture and electro-acupuncture, 8 polarized low-frequency electrical currents, 9 and non-polarized currents, 8,10 can be found in the literature and deserve to be noted. Some recent researchers have been using low-intensity laser. 1,2,3,11,12
Tobacco is considered a drug by the norms that regulate the United States Food and Drug Administration (FDA), which include it in the same group of substances as nicotine, morphine, opium, and other addictive drugs. 13
Studies confirm a significant association between tobacco use and the development of diseases such as cancer in the lungs, oral cavity, stomach, and bladder; obstructive pulmonary disease; and gastroduodenal ulcers; and it is also one of the risk factors for cardiovascular diseases. 14
Some experimental researchers 15,16 observed that there is a deleterious effect on the skin flaps exerted both by nicotine in isolation and by cigarette smoke, causing an increase in the necrotic area in the skin flap.
In the study performed by Campos et al., 5 the authors studied the action of nicotine on randomized skin flaps in mice. They concluded that nicotine was harmful to the skin, increasing the necrotic area when this drug was used in the preoperative period. Its continuous use in the postoperative period has also increased this area.
Medeiros et al. 13 reported that both smoking and the application of plasters of nicotine on the patient's skin inhibit the flow of oxygen to the tissues while in healing, via vasoconstriction induced by the sympathetic nervous system. Similarly, smoking elevates carboxyhemoglobin levels in the blood, resulting in less oxygen tension in the tissues.
In the literature, there is experimental research that attempt to decrease the necrosis of skin flaps caused by nicotine, with pharmacological resources 17,18 and the application of transcutaneous electrical nerve stimulation (TENS) as a physiotherapeutic resource. 19
The shortage of published articles on the use of low-intensity laser to minimize the deleterious effects of nicotine has encouraged us to perform this study in an attempt to reduce these effects, and to provide an increase in the viability of random skin flap in rats.
According to Prado et al. 20 and Pinfildi et al., 2 low-level laser irradiation is a therapeutic method often used to speed up the wound healing process to promote an increase in blood flow and vascular neoplasm, which would enable greater viability of the skin flap in rats subjected to nicotine.
Materials and Methods
Animal experiment
This study was approved by the Ethics Committee on Animal Experimentation of the Medical School in Ribeirão Preto- Universidade de São Paulo, protocol no. 048/2006.
For this study, 24 male adult Wistar rats, weight ranging from 280 to 310 g, were provided by the Central Bioterium of Universidade de São Paulo. The experimental procedures were performed in the experimental morphology laboratory of the Surgery and Anatomy Department at the Medical School of Ribeirão Preto-Universidade de São Paulo (FMRP-USP). The animals were kept in propylene individual cages, with a 12-h light–dark cycle under controlled temperature (22–27°C), maintained on rodent chow, with water ad libitum.
Laser irradiation equipment
Laser irradiation was performed with low-power gallium-aluminum arsenide (GaAlAs), wavelength 830 nm, power 30 mW, continuous wave laser (CW), beam cross section area of 0. 07cm2, irradiance 429 mW/cm2, irradiation time 84 sec, energy 2.52 J, fluence (energy density) 36 J/cm2, Ibramed - Brazilian medical equipment Industry Ltda® (Amparo, Brazil). Application was by the punctual transcutaneous method by contact, with laser positioned at 90° to the skin flap.
The equipment was calibrated in the São Paulo University Physics Department. Before each application, the calibrator was adjusted. Radiant power determination was performed by attaching the end of the laser diode, at a 90° angle, to the digital potency analyzer Lasercheck® (Coherent®, Staunton, VA) sensor, calibrated, and used according to the manufacturer's recommendations. Three consecutive measurements were collected, and the mean value was used.
Experimental model
The skin flaps were delineated (10 cm long × 4 cm wide) according to McFarlane et al., 21 and received the laser irradiation (energy density 36 J/cm2 e energy 2.52 J) in one point at 2.5 cm of the flap cranial base, with a plastic molding being positioned to standardize the area to be irradiated.
The 24 rats were weighed and divided into three groups with eight animals each:
Group 1 (control)
was subjected to subcutaneous injection of physiological saline solution sodium chloride, once a day, for a period of 1 week before and 1 week after the surgical procedure. These random, cranial-based skin flaps were subjected to a simulation of diode laser irradiation.
Group 2
was subjected to nicotine injected in the subcutaneous tissue with a dose of 2 mg/kg once a day for a period of 1 week before and 1 week after the surgical procedure. The cranial-based skin flaps were subjected to a simulation of diode laser irradiation.
Group 3
was subjected to nicotine injected in subcutaneous tissue in a dose of 2 mg/kg once daily for a period of 1 week before and 1 week after the surgical procedure. The cranial-based skin flaps were subjected to laser diode 830-nm irradiation.
The nicotine used in this study [Nicotine Sulphate L-1 Methil-2 (3-Piridyl)-Pirrolidyne Sulphate; grade II; MW 422-6; SIGMA] (St. Louis, MO) was diluted with saline to the concentration of 1 mg/ml 16 and injected in the rats' subcutaneous tissue in Groups 2 and 3.
Surgical procedure
The animals were anesthetized by intraperitoneal injection, with a mixture of ketamine (95 mg/kg) and xylazine (12 mg/kg). After anesthesia, the hair on the animal's back was digitally removed. Following, a cranial based skin flap (10 cm long × 4 cm wide) was performed on their backs. The flap was limited by the line joining the inferior angles of the scapulas and the superior margins of the pelvic bones. 21
The flaps were elevated containing deep and superficial fasciae, panniculus carnosus and skin. A 10 × 4 cm plastic sheet (polyester/polyethylene) was placed between the flaps and the donor sites in order to avoid revascularization of the flaps. 11 Afterwards, the flaps were sutured in the original position (“donor site”) by using 4-0 monofilament nylon thread with simple stitches separated 1 cm from each other. 8
Immediately after the procedure, the animals in Groups 1 and 2 were kept anesthetized for another 30 min. They were then subjected to a simulation with laser irradiation, always at the same time.
In Group 3, the animals were irradiated with 830-nm laser diode, always at the same time, immediately after surgery, in the 4 subsequent days.
Laser irradiation occurred in one point at the 2.5 cm of flap cranial base, with the plastic molding being positioned to standardize the area to be irradiated.
On the 7th post-operative day, areas of necrosis were assessed through two macroscopic analysis techniques, paper template and Mini-Mop® (Semi-automatic Kontron image analysis, Kontron Bildanalysis®, Munich, Germany) and after macroscopic evaluation a 1 cm2 sample was also collected with a punch (local laser irradiation) for subsequent count of pervious blood vessels.
After defining the skin flap and collecting its sample, the animals, still anesthetized, were killed with an overdose of anesthetics.
Method to determine the percentage of necrotic area in the skin flaps
Template method
The percentage of skin flap necrosis area was calculated on the 7th postoperative day through the paper template method. 22 The boundary between viable tissue characterized by skin that was soft, reddish, warm, and haired; and necrotic tissue (skin that was stiff, dark, cool, and hairless) was demarcated on the animals.
A mold of entire flap and the necrotic area was drawn and cut in transparent paper (Fig. 1), being checked in a precision balance (+/− 0.001 g error). After that, the following equation was used:
A mold of the entire skin flap was drawn in translucent tracing paper delimiting the necrotic area from the viable one.
Mini-Mop®
The percentage of the necrotic area was also calculated on the 7th postoperative day through the semi-automatic Kontron image analysis (Kontron Bildanalysis®). A template of the whole flap was delineated in translucent tracing paper to distinguish the necrotic area from the viable one. It was then fixed on the graphics pad of the Mini-Mop®, making the delineation of the total and necrotic area with a ballpoint pen. With this procedure, the Mini-Mop Videoplan®, automatically analyzed the area in mm2, sending the data to a compatible IBM-PC microcomputer to store the files and later convert them to be used in Excel for statistical analysis.
Histological analysis for pervious blood vessels count
After the morphometric evaluation of skin flaps, samples of the viable segments (local application of laser) were collected and immersed in a Bouin fixation solution for 24 h. After, they were immersed in alcohol solution at 70o Gay Lussac (GL) for 2 weeks to remove the excess of picric acid present in the fixation solution. Following, they were submitted to a routine histological examination to be included in paraffin.
Perpendicular cuts to the fragment surface, 5-μm thick, were obtained, colored with Masson's tricome, and mounted between slides and coverslips for conventional morphological analysis.
The miographic photographs were obtained in a conventional light microscope AxiosKop2 plus (Carl Zeiss, NY) with a square image of 1 mm at reticule level to the side, a digital camera Cam HRc Axio (Carl Zeiss) adapted to a Pentium III compatible computer and Axio Vision 3.1. software.
For this count, all pervious blood vessels present in the histological cuts were estimated (veins, arteries, arterioles, and venules)
A total of 100 microscopic fields from each sample were analyzed in a total area of 6.25 mm2, and viewed at 40 × magnification (Fig. 2). The examiner was unaware which group the slide belonged to.
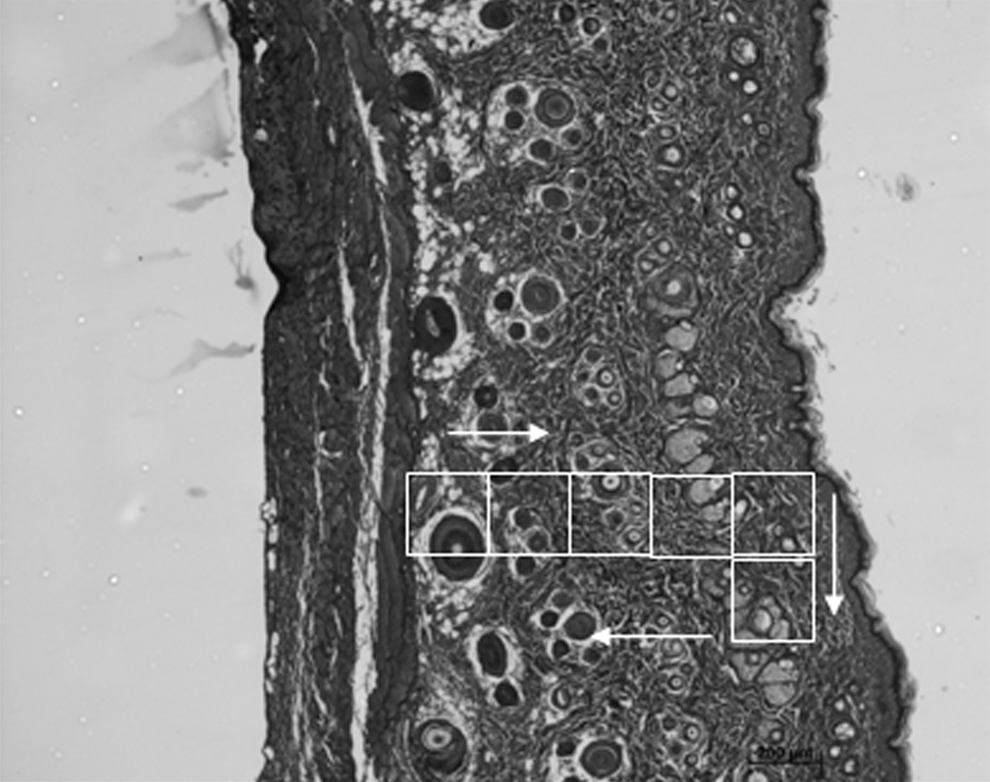
Sequence of microscopic fields used in pervious blood vessel count for histological analysis, totaling 100 fields.
Statistical analysis
After data collection, the results obtained were statistically analyzed through the ANOVA test (variance analysis), followed by the multiple comparison analysis (orthogonal contrast) to compare the groups in each variable (paper template method, Mini-Mop® and blood vessel count. 23 For all statistical tests, a significance level of 5% was set.
Results
Histological aspects of the skin flaps on the 7th postoperative day
The histological examination of the skin at segment level of the laser application in the skin flap (Fig. 3) shows a typical epidermis with several cell layers covered by the stratum corneum.

A relatively thick dermis consisting of a large amount of collagen fibers distributed in all directions characterizes a densely packed connective tissue and is permeated by a large number of hair follicles sometimes associated with the sebaceous glands.
In Groups 1 and 3, a large number of pervious blood vessels of various sizes were observed, whereas in Group 2, these vessels were not easily observed. Cutaneous muscle fibers were visible deep in the dermis.
Percentage values of necrosis area obtained through the paper template method and Mini-Mop®
Data obtained by descriptive statistical analysis, when the two methods were compared to measure the areas where necrosis was established, are shown in Table 1. The graph for the percentage distribution of the necrotic area for each group is represented in Fig. 4.
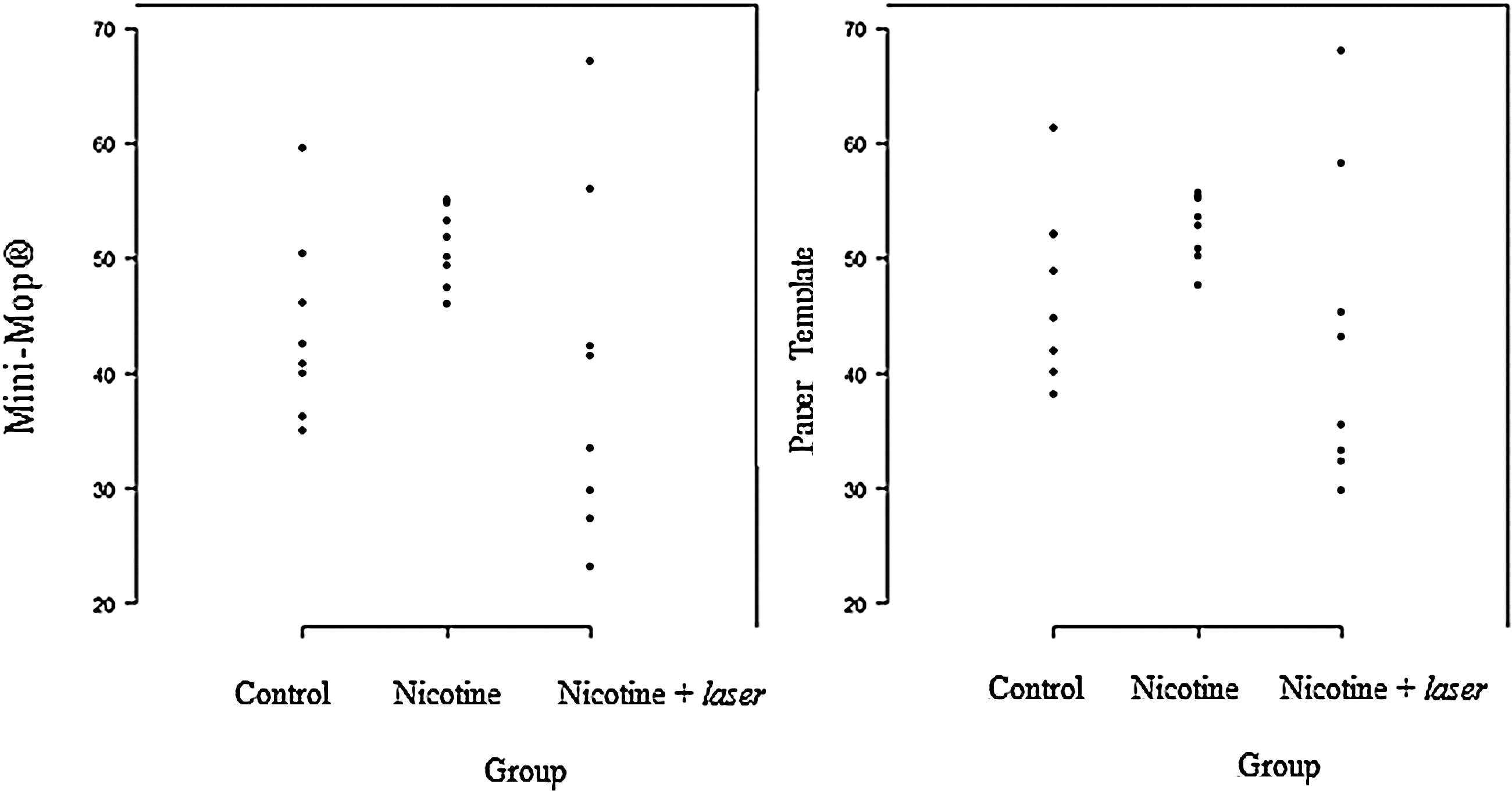
Graph of percentage dispersion of tissue necrosis on the 7th postoperative day through the paper template method and Mini-Mop®.
CV, coefficient of variation.
To verify the existence or nonexistence of statistically significant differences between the two methods, paper template and Mini-Mop®, the intraclass correlation coefficient (ICC) 23 was applied in the three groups.
The ICC obtained with a 95% confidence interval indicated a 0.64 substantial level of agreement between the methods.
Data obtained from the necrotic area in both experimental-method groups were subjected to ANOVA followed by multiple comparison analysis procedure (Orthogonal Contrast Method). The results are presented with a significance level of 5% in Tables 2 and 3.
Mean log difference.
Mean log difference.
The experimental groups showed statistically significant differences between them, but not when compared with Group 1, considering the percentage of necrotic area in both groups (p < 0. 05).
Pervious blood vessel count
Data obtained from the pervious blood vessel count in skin flap samplings in each experimental group are shown in Fig. 5. Their respective means and standard deviations are organized in Table 4.

Graph of dispersion of the number of pervious blood vessels. Group 1, Control; Group 2, Nicotine; Group 3, Nicotine + laser.
CV, coefficient of variation.
Data obtained from the pervious blood vessel count between the experimental groups were subjected to ANOVA followed by multiple comparison analysis procedure (orthogonal contrast method). The results of this post-test with a significance level of 5% are shown in Table 5, with statistically significant differences between Groups 1 and 2 and 2 and 3. There was no difference between Groups 1 and 3.
Discussion
Some experimental researchers attempted to reduce the necrotic area of the skin flaps subjected to the action of nicotine through pharmacological 17,18 and therapeutic resources such as TENS. 19 But so far, there are no studies on the use of low-level laser as a therapeutic resource to improve the viability of skin flaps in rats.
Considering that laser irradiation can promote angiogenesis and increase blood flow, some researchers have started to investigate the effect of this therapeutic agent on the viability of skin flaps. 3,12,20
In this study, the application of laser radiation occurred at a point located 2.5 cm from the base of the flap, based on the experimental model for low-level laser in ischemic random skin flap in rats proposed by Prado et al. 3 The authors attempted to determine the most effective area for the laser application. The laser was applied in different areas, 2.5, 5, and 7.5 cm from the cranial base. The conclusion was that the most effective site to improve the viability of the skin flap was the one located 2.5 cm from the flap cranial base.
In this study, the experimental groups were irradiated during 5 consecutive days, that is, immediately after the operation, and on the 4 following days. Pinfildi et al. 11 and Assis et al. 24 have also used this method to irradiate their experimental groups during 5 consecutive days.
The punctual contact technique was used for laser application, as described in the studies by Amir et al., 25 Pinfildi et al., 11 Bossini et al., 26 and Santos et al. 27 According to some authors, laser application in contact with the skin surface during irradiation increases the penetration depth because of the reduction in reflection and energy dispersion. 28
Studies that used lasers with 830-nm wavelength 29,30 found significant results in the increase of the viability of skin flaps, therefore this wavelength was chosen.
In this study, the parameters used were similar to those in the study by Prado et al., 30 who used a device with 830-nm wavelength, power 30 mW/cm2, fluence 36 J/cm2, and beam irradiation area of 0.07 cm2, with continuous beam.
The fluence used in this research was 36 J/cm2, based on the research conducted by Prado et al., 12 who also used this dose, which was enough to achieve reduction of necrosis. Therefore, the total energy applied on the skin flaps was 2.52 J, and significant reduction of the necrotic area was found, even in animals subjected to nicotine.
The flaps, in this study, were analyzed on the 7th postoperative day because there were signs of necrosis appearing in the flap between the 3rd and 4th days, with the final threshold of necrosis being reached between the 7th and the 10th days. 21
After submitting the percentage data of the necrosis area to statistical tests, obtained through both macroscopic analysis methods (paper template and Mini-Mop®), it was demonstrated that experimental Groups 2 (nicotine) and 3 (nicotine + laser) presented statistically significant differences between them, but not when compared to the control group (Group 1) (p < 0.05). This showed the relevance of the laser in promoting the reduction of the necrotic area, which resulted in a similar size to that of the control group.
To verify the existence or nonexistence of statistically significant differences between the values obtained by the two macroscopic methods (paper template and Mini-Mop®), the ICC 23 considering the three groups obtained a value of 0.64. This shows a great/substantial correlation between the two methods, according to the categorization for the ICC. 23
In addition to the macroscopic analysis of the necrotic area, a skin flap sample was collected on the 7th day to count the pervious blood vessels present in the samples in the three groups studied, to provide additional data regarding the flap viability.
In order to analyze if there was some difference between the groups in relation to the pervious blood vessel count, statistical tests were performed and showed statistically significant difference between Groups 1 (control) and 2 (nicotine) and between Groups 2 (nicotine) and 3 (nicotine + laser). This analysis revealed that nicotine promoted a reduction in the number of pervious blood vessels by vasoconstriction, leading to the increase of tissue ischemia, and consequently, reducing the skin flap viability, which was also observed through the macroscopic methods. Group 3 was not different from Group 1 in the calculation of vessels, which allowed us to clearly characterize the effective action of the 830-nm laser on the increase of viability in the skin flaps tested.
In the studies by Amir et al. 25 and Bossini et al. 26 a larger number of small blood vessels were found in the irradiated flaps. This corroborated the study, which presented a large number of pervious vessels in Group 3 (nicotine + laser), with values statistically similar to the ones obtained in the control group.
Many authors reported that the low-level laser could increase the blood flow in the microcirculation by eliciting the release of nitric oxide, a potent vasodilator, in the irradiated site. 31 In addition, it could promote the release and secretion of vascular growth factor related to angiogenesis, 31 thus enabling more adequate supply of oxygen and nutrients to address the needs of the proliferative phase in the healing process.
When the correlation between the average area of necrosis and the average number of pervious blood vessels was established in the three groups of animals, it was notably recognized that the smaller the area of necrosis of the skin flap, the greater the number of pervious blood vessels in the sample and vice versa.
Conclusions
Low-level laser therapy with a wavelength of 830 nm was effective in increasing the viability of skin flaps in rats subjected to controlled injection of nicotine (Group 3), promoting an increase in the number of blood vessels and reducing the area of necrosis, when compared to non-irradiated ones (Groups 1 and 2).
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
This study was performed at the Laboratory of Anatomy and Surgery, Department of Biomechanics, Medicine and Rehabilitation of the Locomotor System, FMRP-USP, Ribeirão Preto, Brazil.