
Abstract
Introduction
The effectiveness of pit and fissure sealants depends upon the physical and chemical properties of the material (i.e. fluency, and penetration and adhesion properties), morphological complexity of the fissure, position of the tooth, individual skill of the operator, method of application, and, mainly, long-term retention of the sealant material. 8 Clinical performance of sealant materials is affected by the surface texture of the tooth. It has been recommended that fissures should be cleaned with a fluoride-free air slurry polisher before placement of the sealant material, in order to ensure that plaque has been removed from the grooves. 9 The method used for the pre-treatment of the enamel surface also affects sealant success.
Resin-based fissure sealants are usually placed after acid etching. The enamel surface of the tooth is etched and then rinsed and dried before the sealant material is placed. Moisture contamination of the enamel surface reduces the penetration of the sealant, and leads to microleakage.
Several invasive and noninvasive techniques can be used for effective placement and long-term retention of resin-based fissure sealants. 10 The invasive technique involves opening pit and fissure cavities with a dental bur for deepening and widening the pits and fissures and for removing organic material, plaque, and the thin layer of prismless enamel. This invasive procedure enhances acid conditioning, allows deeper penetration of the sealant into the fissures, and extends the surface area. The sealant is then placed over the remaining intact fissures and pits. This procedure is called “preventive resin restoration”. 11,12 Although acid etching is one of the most commonly used noninvasive techniques for conditioning the tooth surface before placement of the sealant material, air abrasion and lasers are also used as alternative noninvasive techniques for surface pre-treatment. 10
An Erbium: Yttrium Aluminium Garnet (Er:YAG) laser is an alternative noninvasive technique to conventional conditioning methods, for surface pre-treatment. 13 –16 Laser etching, a new technique for surface treatment, is a painless procedure and does not involve vibration or heat. It has the advantage of cleaning, conditioning, and decontamination in barely accessible depths of fissures, in only one step, and with a single device. 17 Effective ablation of dental hard tissues with the use of Er:YAG laser is attributed to its 2.94-mm wavelength emission, which coincides with the main absorption band of water (∼3.0 mm) and OH-groups in hydroxyapatite (∼2.8 mm). 18,19 The incident radiation is highly absorbed by water molecules in the dental hard tissues, causing sudden heating and water evaporation. 20,21 The resulting high-stream pressure leads to the occurrence of successive micro-explosions with ejection of tissue particles, which are characteristic of the ablation process and determine the microcrater-like appearance of lased surfaces. 17,21 –23 With its decontaminating and cleansing properties, laser pre-treatment of occlusal pits and fissures with a subsequent phosphoric acid etching is a treatment option for “deep fissure” caries and is also preferred in minimally invasive procedures (e.g., preventive resin restoration) to obtain a better clinical outcome. 24,25
Air abrasion, another method for surface pre-treatment, which has been used in dentistry since 1945, has become more popular with the development of minimally invasive dentistry. In this technique, a high-speed stream of purified aluminium oxide or newly developed calcium carbonate (CaCO3) particles delivered by air pressure is used to abrade the enamel. 26 The advantages of this method include the lack of pressure, heat, noise, and vibration of dental rotary instruments, reduced pain, and less need for local anesthesia. 27 –29 Surface pre-treatment with air abrasion provides a roughened surface necessary for optimal bonding with the sealant material. 30
The aim of the present study was to evaluate the effects of the following different surface pre-treatment techniques on marginal integrity: (a) Er:YAG laser irradiation at two different output powers, (b) a combination of Er:YAG laser irradiation at two different output powers and acid etching, (c) air abrasion alone, (d) a combination of air abrasion and acid etching, and (e) acid etching alone. The null hypothesis tested was that the variations in the methods of surface pre-treatment would not affect the marginal seal of a resin-based fissure sealant material.
Materials and Methods
Thirty-five human third molars without occlusal carious lesions were collected. The teeth were cleaned with a scaler and pumice/water slurry in dental prophylactic cups to remove the debris from pits and fissures, and stored up to 6 months in sterile saline solution. The study was conducted at the Istanbul University, Faculty of Dentistry, Department of Operative Dentistry. All steps of the procedure were performed by the same operator. Regardless of fissure types and depths, teeth were randomly divided into seven experimental groups based on the surface pre-treatment technique used (n = 5 for each group; Table 1). The compositions and the application steps of the materials used are presented in Table 2.
Bis-GMA; bisphenol A glycidyl methacrylate.
Study groups
In group 1, Er:YAG laser irradiation was performed at a wavelength of 2940 nm with an output power of 7 W (20 Hz, 350 mJ) using an Er:YAG laser system (Versawave; Hoya Conbio, Fremont, California). This output power was chosen in accordance with the manufacturers' recommendation to use in the enamel tissue. The laser beam was aligned perpendicular to fissures in the non-contact mode at 1 mm distance, in accordance with the manufacturer's instructions for pre-treatment of the enamel surface before placement of the sealant. The duration of exposure depended upon the time needed to guide the laser beam evenly across the pits and fissures to be irradiated. After irradiation, teeth were rinsed and air-dried, and fissure sealant (Helioseal F; Ivoclar-Vivadent, Schaan, Liechtenstein) was applied and light-cured for 20 sec (VIP; Bisco Inc., Schaumburg, Illinois).
After laser irradiation at the same output power (7 W) as was described for group 1, the ablated occlusal surfaces were etched with 37% orthophosphoric acid (Total Etch; Ivoclar Vivadent) for 15 sec in group 2, and then rinsed thoroughly with copious water for 20 sec, air-dried for 5 sec, after which Helioseal F was applied and light-cured for 20 sec.
In group 3, laser irradiation was performed on the enamel surfaces at an output power of 5.5 W (25 Hz, 220 mJ). Helioseal F was applied without an acid etching procedure and light-cured for 20 sec.
In group 4, laser irradiation was performed at an output power of 5.5 W, as was described for group 3. After the occlusal surfaces were acid-etched with 37% orthophosphoric acid for 15 sec, fissure sealant was applied and light-cured for 20 sec.
In group 5, occlusal fissures were abraded using an air abrasion device (PROHPYflex 3; Kavo, Biberach, Germany) with PROPHYpearls (CaCO3 powders; 45 μm) at an angle of 45° and a 2–3 mm distance from the tooth surface. The working air pressure of the air-polishing devices was set to 3.2 bar (manufacturers recommendation) measured with a pressure gauge between the air turbine clutch and working handpiece. After air abrasion, teeth were rinsed thoroughly with water for 30 sec. Occlusal surfaces were then etched with a 37% orthophosphoric acid, rinsed thoroughly with water for 20 sec and air-dried for 5 sec. Helioseal F was then applied and light-cured for 20 sec.
In group 6, the occlusal surfaces were air-abraded, as in group 5, rinsed thoroughly with water for 30 sec, and air-dried for 5 sec. Fissure sealant was applied on the air-abraded fissure surfaces without an acid etching and light-cured for 20 sec.
Group 7 was the control group, in which pits and fissures were acid-etched with a 37% orthophosphoric acid without any surface pre-treatment, rinsed thoroughly with water for 20 sec, and air-dried for 5 sec. Helioseal F was then applied and light-cured for 20 sec.
Thermocycling, dye penetration and evaluation
The sealed molars were thermocycled in deionized water for 10,000 cycles between 5 ± 2 and 55 ± 2°C, with a dwell time of 30 sec, at the Selcuk University, Faculty of Dentistry. The sealed molars were then stored in individual tubes at a humidity of 100%, at 37°C for 1 week. The surfaces of the sealed molars were coated with wax, leaving the sealant and ∼2 mm enamel around it uncovered. The wax was covered with nail varnish (four times). Afterwards, the specimens were immersed in 5% methylene blue for 24 h.
After thermocycling and dye penetration procedures, the molars were rinsed thoroughly with tap water and the roots were removed with a diamond bur. The nail varnish was removed from the crown of each tooth. The sealed crowns were embedded in self-curing acrylic (Pan Acryl; Inci Dental, Istanbul, Turkey). Using a low-speed saw under water cooling (Isomet; Buehler, Lake Bluff, Illinois), the specimens were sectioned mesiodistally with three parallel cuts of 1-mm thickness, yielding six surfaces per tooth for analysis. Microleakage evaluation was performed by two observers, who were blinded to the pre-treatment techniques, using a standardized method, in which microleakage was scored under a light microscope (Olympus Optical Co., Tokyo, Japan), at x40 magnification. The images were also analyzed using ImageJ image processing software (Version 1.34 s; National Institutes of Health, Bethesda, Maryland). Microleakage was assessed by scoring dye penetration as a qualitative method as well as a quantitative rational measurement method.
In the qualitative assessment, microleakage was scored on a three-point rating scale, in which Score 0 indicated no microleakage; Score 1 indicated microleakage up to one-half of the fissure wall; and Score 2 indicated microleakage more than one-half of the fissure wall (Fig. 1). In the quantitative assessment, microleakage was evaluated by the microleakage proportion [(A+C)/(B+D)] that was expressed as the length of dye penetration (A+C, in mm) divided by the length of the sealant-tooth interface (B+D, in mm), (Fig. 2). 31
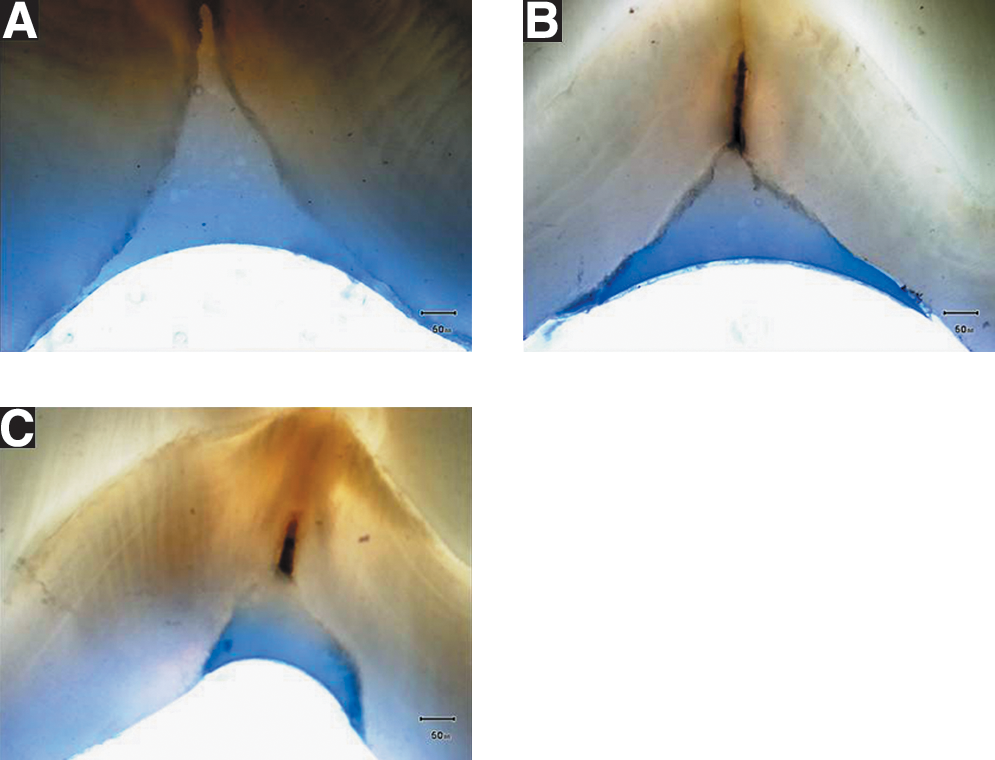
Examples of the standardized scores. (

Diagrammatic depiction of the measurement of the dye penetration. Length of dye penetration (a+c), length of tooth–sealant interface (b+d).
Statistical analysis
Data were analyzed using SPSS for Windows (Version 11.0, SPSS Inc., Chicago, Ilinois). A preliminary analysis was performed using the Kolmogorov–Smirnov test in order to test the normality of the data. Because the data was not normally distributed, one-way analysis of variance (ANOVA) and Kruskal–Wallis test were used to assess intra-observer agreement in microleakage scoring. The chi-square and Fisher's exact tests were used to test group differences in microleakage scores. The Mann–Whitney U test was used to test the statistical significance of the differences. For pairwise multiple comparisons, the Bonferroni correction was used. A p value <0.05 was considered statistically significant.
Results
The percentages of dye penetration along enamel/sealant interface in the experimental groups and post-hoc pairwise multiple comparisons are presented in Table 3. The Kruskal–Wallis H test revealed a significant difference between the experimental groups (p < 0.05).
The same superscript letters represent the lack of statistical significance, whereas different superscripts represent the presence of statistical significance among the experimental groups.
According to the dye penetration scoring (via scoring; 0, 1, 2), conventional acid etching showed significantly less microleakage than conditioning with Er:YAG laser irradiation, regardless of the output power or subsequent acid etching (p < 0.05). Although not significant, microleakage score was lower in the group in which a combination of air abrasion and acid etching was performed than in the group in which only air abrasion was performed (p > 0.05; Fig. 3). The microleakage score of the group in which a combination of air abrasion and acid etching was performed, was similar to that of the group in which conventional acid etching was performed.
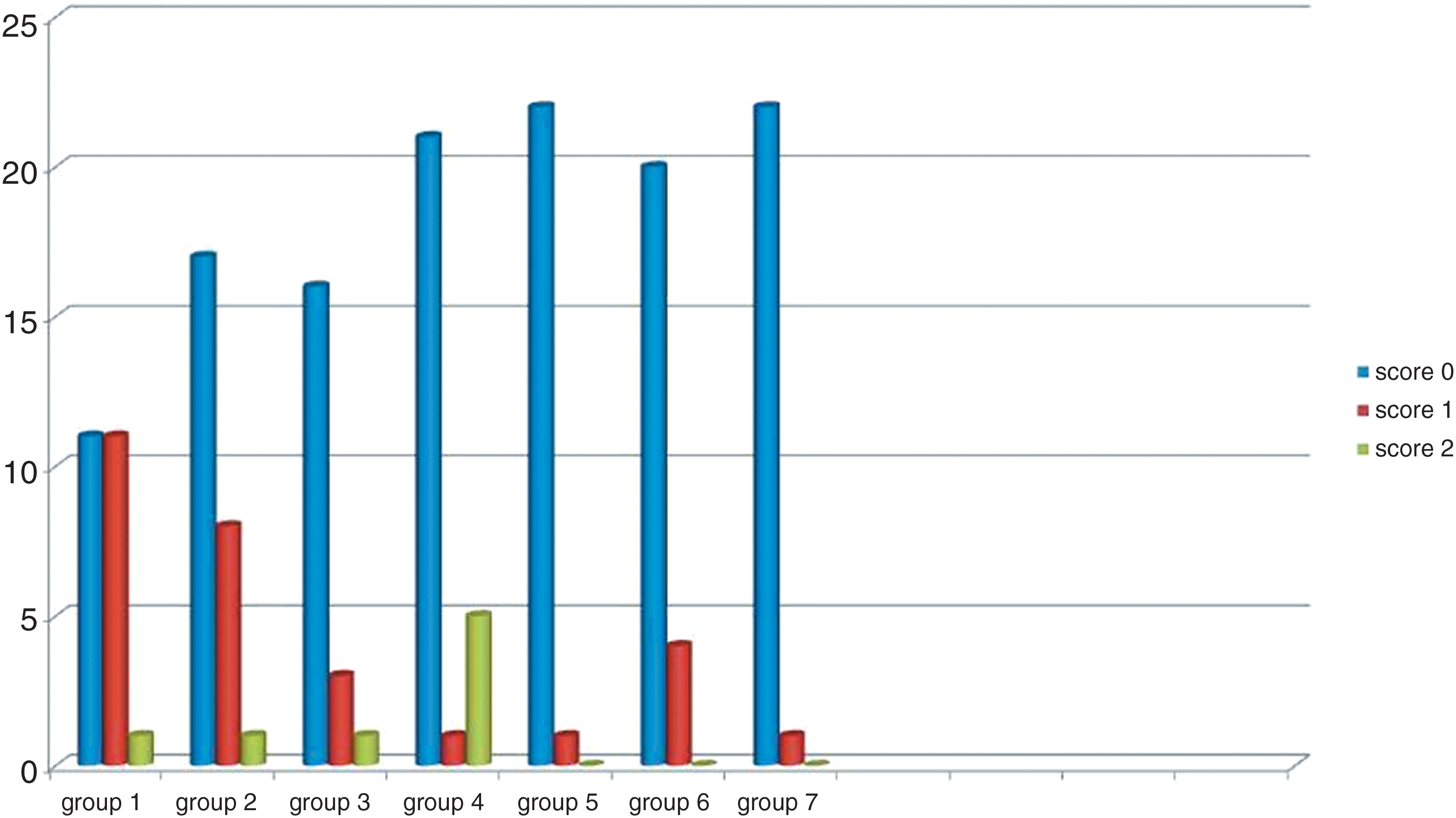
Microleakage scores per molar and per experimental group.
The groups in which a combination of laser irradiation and acid etching was performed and the groups in which only laser irradiation was performed exhibited higher microleakage at the enamel/sealant interface than the other experimental groups. No significant differences in microleakage scores (p > 0.05) were noted between the laser-irradiated groups and the “air abrasion only” group. Although not significant, the group in which only air abrasion was performed showed less microleakage than the laser-irradiated groups, whereas it exhibited more microleakage than the group in which a combination of air abrasion and acid etching was performed, and the group in which only conventional acid etching was performed (p > 0.05).
Quantitative evaluation of microleakage proportion revealed that the group treated with conventional acid etching, as well as those treated with air abrasion and acid etching, showed less microleakage, with a 99% complete sealing compared to the other experimental groups (p < 0.05). Laser irradiation at an output power of 7 W, and the combination of laser irradiation at an output power of 7 W and acid etching, led to 88% sealing, and these two groups irradiated with laser at an output power of 7 W exhibited significantly higher microleakage than the other groups (p<0.05).
As is indicated by both qualitative and quantitative results, groups treated with conventional acid etching and a combination of air abrasion and acid etching exhibited less microleakage than the other experimental groups.
Discussion
The null hypothesis of the present study, stated as “the variations in the methods of surface pre-treatment would not affect the marginal seal of a resin-based fissure sealant material,” was rejected, as the group in which conventional acid etching was performed, as well as the group in which a combination of air abrasion and acid etching was performed, showed less microleakage than the laser-irradiated experimental groups.
In addition to physicochemical interaction between the resin and enamel, retention of the sealant material depends upon mechanical adhesion of the material. 32 As the mechanical bond between the resin and enamel is accepted as the main factor in sealant retention, the most important variables among physical factors include surface characteristics, morphology, and surface roughness of the enamel. The longevity of fissure sealants placed is related to the presence of a sufficient bonding strength between the tooth surface and the material, and to the retention of the sealant material. Gaps formed at the bonding interface between the sealant material and tooth surface lead to microleakage and debonding, which causes failure of the restoration. When evaluating the performance of a sealant material, microleakage is an important factor that reflects the insufficient bonding between the tooth and sealant material. Measurement of microleakage is an effective method to evaluate the effectiveness of different surface preparation and conditioning methods for fissure sealants. 33 In the present study, different surface pre-treatment methods were employed before placement of the sealant material, and microleakage was measured quantitatively and qualitatively to evaluate the effectiveness of different surface pre-treatment methods in providing sufficient bonding. Beside its common use in microleakage studies, evaluation of microleakage with qualitative data is not sensitive enough. Therefore, we calculated the microleakage proportion, which was expressed as the length of dye penetration divided by the length of the sealant–tooth interface to obtain quantitative data, which is more sensitive in examining the marginal seal. In the present study, the qualitative results were in accordance with the quantitative results. Although both quantitative and qualitative methods used for microleakage assessment in the present study revealed similar results, it might be suggested that quantitative assessment provided more objective evaluation. The qualitative scoring of the microleakage according to the enamel and dentin thickness is subjective and less sensitive, as the enamel or dentin thickness varies in each tooth. However, assessment of microleakage proportion, which was expressed as the length of dye penetration divided by the length of the sealant–tooth interface, is a more sensitive and objective measurement. In the present study, as the experimental groups were designed regardless of the fissure types, the penetration depths were variable. Therefore, the high standard deviations in the results might be attributed to the differences in fissure morphology and fissure orifice. When quantitative measurement is used to assess the microleakage, standardization of the fissure types and penetration depths are recommended.
Temperature changes in the oral cavity are important factors that can cause microleakage. As temperature changes in the oral cavity can affect the bonding interface between the sealant material and tooth surface; we evaluated dye penetration after the samples were thermocycled for 10,000 cycles, with a dwell time of 30 sec to simulate oral conditions. 34
Advances in minimally invasive dentistry introduced new technologies, such as Er:YAG laser irradiation and aluminum oxide air abrasion, to remove dental hard tissues. The tooth surfaces are prepared before adhesive applications with the least discomfort for the patient. 35,36
Er:YAG laser has been considered as a promising alternative for preventive dentistry because of its ability to increase fluoride uptake and decrease acid solution, thereby creating a surface more resistant to acid attack. 37 Therefore, if a sealant falls out from a laser-pretreated tooth, the surface would be more resistant to acid dissolution. 38 The laser pre-treatment approach has proven to be effective for the preparation of the enamel surfaces of pits and fissures before placement of the sealant only when the procedure is followed by the phosphoric acid treatment, a step that cannot be eliminated. 39 –42 In the present study, the enamel surfaces conditioned with Er:YAG laser irradiation showed higher microleakage than those conditioned with air abrasion followed by acid etching, as well as those conditioned with acid etching alone. Although not significant, the enamel surfaces conditioned with Er:YAG laser irradiation followed by acid etching exhibited less microleakage than those conditioned with Er:YAG laser irradiation alone. These results were in accordance with those reported in previous studies, in which Er:YAG laser irradiation alone or a combination of Er:YAG laser irradiation and acid etching was compared with conventional acid etching treatment. 13,14,33 Er:YAG laser irradiation of fissures followed by acid etching have not yet provided sufficient sealing compared to conditioning with air abrasion alone, conditioning with air abrasion followed by acid etching, or conditioning with conventional acid etching.
It is stated that the laser irradiation causes morphological changes such as porosities, cracking, and microfissures, which were responsible higher microleakage. 20 Microporosities of laser-irradiated enamel surfaces, which result in a disorganized destruction of enamel prisms, are not as uniform as acid-conditioned enamel, thereby leading to poor sealing with higher microleakage. 43 These unexposed areas could be caused by the pulsed nature of the laser beam. The irregular etching pattern of the laser irradiation may adversely affect the quality of the marginal integrity and seal. 42 The higher degree of microleakage observed at the tooth–sealant interface of Er:YAG laser-irradiated fissures could be the result of the morphologic configuration of the dental substrate after irradiation with a high output power. It has been shown that the higher the frequency, the lower the cooling of the irradiated tissue between the pulses, and therefore the higher the temperature of the lased surfaces. Extensive and multiple areas of fusion and re-crystallization appear to interfere with the bonding procedure. 44,45 Er:YAG laser irradiation also modifies the calcium-to-phosphorus ratio, and leads to the formation of more stable and less acid-soluble compounds, which would adversely affect the sealant adhesion. This acid-resistant enamel surface might compromise the diffusion of the adhesive system. 37,46 Therefore, an additional phosphoric acid etching should be combined with laser pre-treatment to prepare the surface.
In the present study, the fissures were irradiated with Er:YAG laser at two different energy output (5.5 and 7 W) according to the manufacturers' recommendation for the enamel surface preparation (5–7 W), alone or followed by acid etching. Er:YAG laser was performed on fissures at 7 W under water cooling in the non-contact mode to increase the fissure surface area and to improve the penetration and retention of the sealant. The group irradiated with laser at an output power of 7 W, and the group irradiated with laser at an output power of 7 W followed by acid etching showed higher microleakage than the two groups irradiated with laser at an output power of 5.5 W. It was previously demonstrated that the specimens conditioned with Er:YAG laser irradiation at 200 mJ under water cooling exhibited fissures free from debris and enamel etching-like patterns predominantly, with no signs of melted and recrystallized enamel. 47 In the present study, fissures conditioned with Er:YAG laser irradiation at an output power of 5.5 W exhibited higher microleakage than those conditioned with either air abrasion or acid etching. Laser irradiation alone was not able to maintain a highly resistant interface, and therefore non-etched surfaces exhibited higher microleakage. There are also many studies evaluating the microleakage and marginal adaptation using Er:YAG laser irradiation at high output powers (>300 mJ). Such high output powers induce enamel subsurface damage. Therefore, the use of Er:YAG laser alone has been reported in many publications to result in poorer marginal adaptations with a higher degree of microleakage. On the other hand, finishing the enamel surfaces with acid etching after Er:YAG laser irradiation has been reported to exhibit better marginal adaption. 13,20,37,43 Moshonov et al. 48 reported in their study that the use of high energy output (800 mJ) with ER:YAG laser resulted in no difference in microleage between lased and acid-etched surfaces. This discrepancy is explained by some authors as the high output power, causing a significant removal of dental substance, which interferes with the marginal sealing at the fissure surfaces. 48,49
Surface pre-treatment with air abrasion technique is painless, silent, and more conservative than pre-treatment with rotary instruments, but needs the use of a rubber dam to avoid the spread and aspiration of abrasive particles. 50 Stains and debris can easily be cleaned by an air-abrasive technique, thereby revealing the underlying caries hidden by the stains. Some authors have stated that the enamel surface roughened by the air abrasive particles can also maintain a microretentive surface ready to bond a resin material without the need of acid etching. 13,49 Manhart et al. 33 also showed that the superficially roughened enamel with a retentive surface morphology was created by the use of air abrasion.
In the present study, the fissures pre-treated with air abrasion followed by acid etching, and the fissures pre-treated with acid etching alone exhibited less microleakage than did those in the other experimental groups. This finding was consistent with the results of the study by Duangthip and Lussi 51 who reported that air abrasion combined with acid etching improved the penetration ability of sealants, and provided a better seal than the traditional pumice cleaning and acid etching treatment. Air abrasion technique removes the dental substrate mechanically without heat generation. Therefore, this technique affects neither the organic nor the inorganic components of tooth. 49 Removal of the prismless layer of enamel at the entrance and the wall of the fissures by air abrasion technique enhances the development of resin tags for better bonding. 52 Air abrasion technique has been reported to be more effective when combined with acid etching. 53,54 According to the findings of the present study, the use of air abrasion followed by acid etching can be recommended to maintain an adequate seal. However, it should be kept in mind that the dust particles generated during the procedure can be annoying, the devices are not cheap, and the manufacturer's instructions for use and warning statements should be strictly followed. Because of the previously mentioned limitations of the alternative surface pretreatment techniques, conventional acid etching treatment still remains the preferred technique.
Conclusion and Summary
In the present study, conventional acid etching, as well as air abrasion followed by acid etching, showed less microleakage than techniques used in the other experimental groups. Pre-treatment of fissures with air abrasion alone resulted in higher microleakage than did pre-treatment with a combination of air abrasion and acid etching. Pre-treatment with Er:YAG laser and air abrasion alone resulted in higher microleakage than did conventional acid etching. Laser pre-treatment of the enamel surface should be combined with acid etching. Alternative surface pre-treatment techniques exhibited better results when combined with acid etching. In accordance with the findings of previous studies, there is still a need for the use of an acid-etching procedure to obtain a sufficient seal. Although pre-treatment with air abrasion followed by acid etching, and pre-treatment with acid etching alone provided similar results, conventional acid-etching technique still remains the preferred method because of its simplicity and effectiveness. Occlusal pits and fissure pre-treatments resulted in loss of enamel substance especially when air-abraded with coarse air abrasion powder and laser irradiated with high output power according to the manufacturers' instructions. Therefore, composite resin restoration should be the treatment choice for these pre-treated occlusal fissures and pits, in order to minimize the effects of polymerization stress and occlusal forces, instead of sealing with fissure sealants. In these circumstances, it should be noted that material choice could be affected by surface pre-treatments prior to the fissure sealant application that would be done according to the different manufacturers' instructions.
Footnotes
Acknowledgments
The authors gratefully acknowledge Ozden Calay, M.D. for her cooperation with the statistical analysis of the study.
Author Disclosure Statement
No competing financial interests exist.