
Abstract
Introduction
When endodontic treatment fails, resistant microorganisms are usually present. Enterococcus faecalis is a gram-positive facultative anaerobic bacterium frequently associated with endodontic treatment failure 4 that forms intra- and extraradicular biofilms. This biofilm pattern protects the bacteria from the action of intracanal irrigants and medicaments. 5 For this reason, research has sought alternative procedures to those conventionally used during root canal treatment with the attempt to improve the outcome, especially in those cases of persistent apical inflammation.
Techniques, instruments, and equipments have been developed to improve clinical work and achieve high success rate in treatment. Since the early 1990s, several studies have been done on the impact of low-intensity lasers in endodontics. 6,7 Promising results have been shown in microbial reduction in the root canal system by photodynamic therapy (PDT). 3,8 –10 Photodynamic inactivation of microorganisms is based upon the concept that a dye, known as a photosensitizer, should be localized preferentially in the bacteria and not in the surrounding tissues or cells, and subsequently activated by low doses of visible light of an appropriate wavelength to generate free radicals or singlet oxygen that are toxic to target microorganisms. 11,12
The disadvantage of PDT is in the photosensitizing agents that may stain the tooth structure. To date, there has been no study published that aimed to minimize or solve this problem. Therefore, the aim of this study was to evaluate the efficiency of several chemical adjuncts in methylene blue (MB) removal, after PDT in root canals.
Methods
Sample selection
Forty single-rooted caries-free human teeth were selected for the study (Ethics Committee approval No. 168/09, Ethics Committee of School of Dentistry, University of Taubate, Brazil). The teeth were scrubbed, autoclaved and stored in saline until use.
Sample preparation
After access opening, the root canal contents were removed with Hedströem files (Dentsply/Maillefer, Ballaigues, Switzerland) and 2.5% sodium hypochlorite (NaOCl). Working length was established by negotiating the canal with a No. 10 file (Dentsply/Maillefer) until it could be visualized through the apical foramen, and then 1 mm was subtracted.
Cleaning and shaping was achieved with hand files (K-files, Dentsply/Maillefer, Ballaigues, Switzerland) and 2.5% NaOCl. After each file, rinse and suction were performed using 0.2 mL of 2.5% NaOCl, and the root canals were prepared until a No. 55 master apical file. After completion of cleaning and shaping, the canal was completely filled with 17% ethylenediamine tetracetic acid (EDTA) (Biodinâmica, Ibiporã, Paraná, Brazil) and soaked for 3 min for smear layer removal. A final rinse was performed with 2 mL of 2.5% NaOCl followed by 2 mL of distilled water. The canals were then dried with paper points (Dentsply/Maillefer).
PDT
The root canals were completely filled with 0.01% MB solution (Farmacia de Manipulação Formula & Ação, São Paulo, Brazil) with a 30-gauge needle (ProRinse, Dentsply-Tulsa Dental, Tulsa, OK) and left soaking in the canal for 5 min, as pre-irradiation time. The canals were then irradiated with a diode laser (660 nm) (MMOptics, São Carlos, São Paolo, Brazil) coupled with a 300-mm diameter cylindrical optical fiber. The laser power output was 40 mW, the irradiation time 240 sec, and the amount of energy was 9.6 J. Assuming 2 that the root canal surface area is 0.316 cm2, the output power used in the present study corresponded with an energy fluence of ∼30.4 J/cm2 and a power density of 126.6 mW/cm2. Spiral movements were applied to the fiber to ensure an equal diffusion of the light inside the tooth. 13
The crowns were sectioned from the roots at ∼3 mm under the cementoenamel junction using a low speed diamond saw (Isomet; Buehler, Lake Bluff, IL). The root canal orifices were sealed with composite resin (TPH Spectrum, Dentsply Detrey, Konstanz, Germany) to maintain the dye and further chemical adjunct in the root canal space.
Division of groups
The specimens were randomly divided into four groups (n = 10) according to the chemical adjunct employed for dye removal: (a) NaOCl, irrigation with 2.5% NaOCl; (b) NaOCl + Endo-PTC cream, irrigation with 2.5% NaOCl in conjunction with Endo-PTC cream rubbing on the walls of the pulp chamber with a cotton pellet; (c) irrigation with 70% ethyl alcohol; and (d) control group, irrigation with saline.
Each specimen was irrigated with 15 mL of the respective solution for 3 min delivered by a 30-gauge needle (ProRinse, Dentsply/Tulsa Dental, OK) placed in the pulp chamber.
Standardization protocol for digital images
The samples were individually positioned in a plaster apparatus, made for the present study, consisting of a negative impression mold of the lingual aspect of the tooth, in order to standardize the sample position while performing readings with the photographic camera.
Dental stone type IV (Herostone, Vigodent, Petrópolis, Brazil) was mixed and inserted in plastic cups. The teeth were held in place with finger pressure until setting of plaster, thus obtaining a replica of each tooth, with personalized height, length, width, and depth.
Chromatic analysis
Photographs were taken of each specimen in its respective plaster apparatus by using a Canon Rebel digital camera (Canon Inc., Tokyo, Japan) with a 105-mm macro lens (Sigma, Hong Kong). The lens/object distance was 200 mm ± 5, the aperture was closed to f = 22 and exposure speed was 1/250 sec. Illumination was given with two 5500° Kelvin bulbs, fixed on a static table in which a vertical stem fixed the digital camera, providing an optical setup of 0° observation and 45° illumination to the object. Digital images were taken at 3 time intervals: before the PDT (T0), after irradiation (T1) and upon dye removal (T2).
The images were digitized, with an input resolution of 350 pixels per inch, using an image editing software (Adobe Photoshop 7.0.1). All images were saved in jpeg mode.
The image, originally from the CYMK system (C = cyan, Y = yellow, M = magenta, K = black), was converted to 256 gray scale levels. The chromatic alteration was evaluated by the K color system, which measures the variation of the brightness or the values of black, white, and intermediate gray levels of an image in gray scale. Four points from cervical third in each tooth were selected for evaluation. The K values (the percentages of white and black in a scale from 0 to 100) from each point were entered in a table, at all time intervals (Fig. 1).

Chromatic alteration analysis. Image digitized and K values calculated using Adobe Photoshop 7.0.1.
Statistical analysis
A paired t-test was used for intragroup analysis to compare the K values in each group at the different experimental times (T0, T1, and T2). This test was selected because in this case the same samples were used for each experimental time and the data distribution was normal. The effectiveness of the tested protocols for MB removal was determined by the difference between T2 and T1. Additionally, Kruskal–Wallis test, complemented by Dunn's test, was used for comparative intergroup analysis detecting the statistical differences between the tested protocols. This test was selected because in this case the data distribution was not normal.
Results
Table 1 shows the means of absolute values of K in each group at the experimental times: before the PDT (T0), after irradiation (T1), and upon dye removal (T2). When comparing T0 and T1, the results showed significant increase of K values indicating staining degree after PDT in all groups.
*Equal letters denote no significant statistic difference (p < 0.05).
Comparing T1 and T2, the K values decreased significantly in all groups after the use of chemical adjuncts.
When comparing T0 and T2, only in the groups irrigated with NaOCl and NaOCl + Endo-PTC showed no significant difference in the K values, which means that the specimens of those groups exhibited similar color before PDT and after the use of those post-PDT protocols.
The comparison among the groups according to the protocols for dye removal is shown in Fig. 2. The effectiveness of the chemical adjuncts tested for MB removal was determined by the difference between T2 and T1, and was in decreasing order: NaOCl + Endo-PTC cream (−3.11) > NaOCl (−2.97) > ethyl alcohol (−1.28) > saline solution (−1.19). There were no significant statistical differences between the groups irrigated with NaOCl, or between the control group and the group treated with ethyl alcohol.
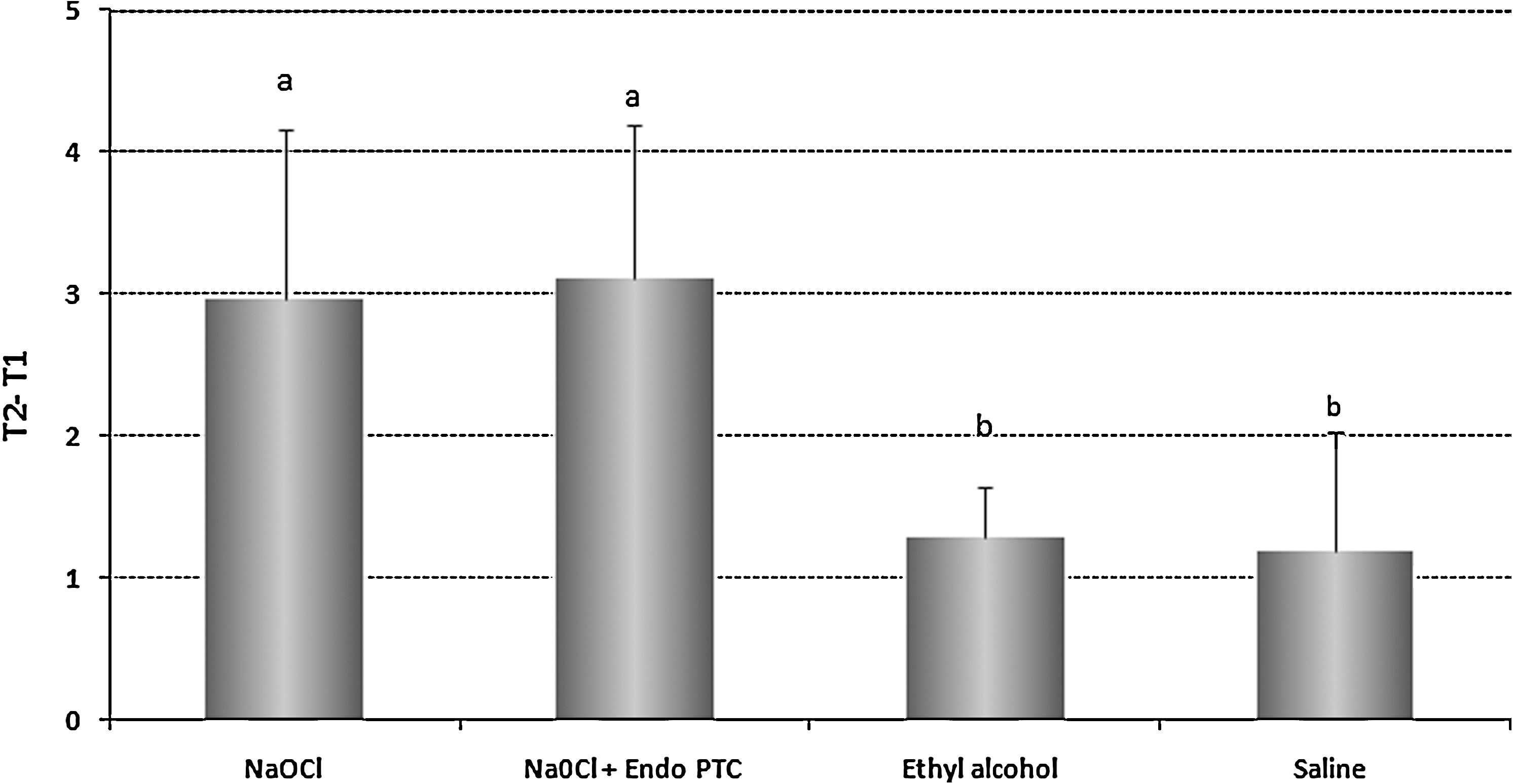
Analysis of effectiveness of MB dye removal in the groups tested (difference between T2 and T1). Standard deviation and results for intergroup statistic analysis by Kruskal–Wallis test. *Equal letters denote no significant statistic difference (Kruskal–Wallis test, p < 0.05).
Discussion
Color assessments for dental coloration have been made using value-oriented shade guides, colorimeters, and digitized photographs. 14 –16 In this study digitized photographs were used for this purpose. The methodology used to asses dye removal was based upon the difference in K values between the time intervals T2 and T1. The K values indicate the percentage of gray scale values varying from black at the weakest intensity to white at the strongest (0–100). Higher K values indicate dental staining. Therefore, greater negative values among the averages of those differences indicated a better performance by the employed protocol.
The best protocols to remove staining from MB when used for PDT were rinse with 15 mL of 2.5% NaOCl + rubbing with Endo-PTC cream and rinse with 15 mL of 2.5% NaOCl. When both protocols were used, the crowns presented with color that was very similar to the color prior to PDT.
MB is one of the most common used photosensitizers for PDT. It is an organic dye from the phenothiazine family, and has well-established photosensitizing properties, effective absorption of light with wavelengths >600 nm into the near-infrared, and capacity to penetrate into dentinal tubules. 2,3,8 Several microorganisms including gram-positive and gram-negative oral bacteria are known to be photoinactivated by MB, exhibiting efficient sensitization of singlet oxygen. 2,12
The MB removal by NaOCl is probably caused by its physicochemical properties, specially the capacity to release chlorine and oxygen, contributing to dental cleaning and bleaching. 17
Endo-PTC is a cream consisting of 10% urea peroxide, 15% Tween 80 (detergent), and 75% carbowax (vehicle) which is used as a lubricant during cleaning and shaping of the root canals. 18 Recently, Silva Garcez et al. 19 demonstrated the effectiveness of PDT with a paste base photozeinsitizer (Endo-PTC and .01 MB) against Enterococcus faecalis. According to the authors, the reaction between urea peroxide present in the paste and the water facilitated the photodynamic mechanism by increasing the production of oxygen-reactive species.
In the present study, the urea peroxide cream, when used with NaOCl, might have increased the release of oxygen bubbles with a continuous and lasting sparkle, because of the presence of carbowax that mechanically cleaned the dental crown. Perhaps the continuous oxygen release may have been the reason why the group in which both NaOCl and Endo-PTC cream were used demonstrated slightly better results (greater negative values among the averages of T2-T1). Gonçalves 20 also verified that the association of Endo-PTC cream and NaOCl as endodontic irrigant solutions after PDT minimized the possibility of dental discoloration.
In the ethyl alcohol group the values were similar to those in the control group (treated with saline). MB is cationic and soluble in alcohol and water, 21 however, 70% ethyl alcohol quickly evaporates and perhaps the contact time was not sufficient for the alcohol to penetrate into dentin and remove the dye from the pulp chamber in a satisfactory fashion.
Several dyes from different colors (blue, green, brown, purple) have been tested for PDT. 22, 23 However, the disadvantages of photosensitizing agents derived from the phenothiazine family (toluidine blue and MB) include the possible staining of the dental structure. Trying to minimize tooth staining, recent studies have evaluated different types adjuncts used for cleaning and shaping of the root canal system, 10,20,22 or have indicated the use of formulations with lower concentrations, in an attempt to minimize such side effects. 24
The concentration of 0.01% of MB was selected for being low but still having proven bactericidal effects. 19,25,26 The results showed an increase in K values (dental staining) from T0 to T1 in all groups, demonstrating that even at a very low concentration, the MB was able to penetrate into the dentinal tubules and stain the tooth structures after PDT. Gonçalves also demonstrated dental staining after PDT when using 0.01% MB. 19
To our knowledge, there are no studies that assessed how MB can be eliminated from the tooth after PDT. Our study demonstrated a simple protocol to be used to avoid dental staining caused by MB. Therefore, further studies should be performed with other dyes and concentrations to determine potential protocols to minimize dental staining after PDT.
Conclusions
Protocols to remove photosensitizing dyes should be applied after PDT in order to minimize or avoid tooth staining. The protocols tested in this study using 2.5% NaOCl, with or without Endo-PTC cream, were effective in avoiding tooth staining caused by MB dye during PDT.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest in relation to any methodology, equipment, or supplies utilized in this investigation.