
Abstract
Introduction
One of many possibilities for how to modulate trachea healing may be the use of low-level laser therapy (LLLT). LLLT belongs to a group of photochemical interactions of low-energy laser radiation with the tissues and cells of living organisms. At the present time, however, there is no general agreement about the exact mechanism of how LLLT influences wound healing. Nevertheless, it has already been demonstrated that LLLT reduces pain; 9 –12 positively influences inflammatory, proliferative, and maturation phases of healing; 13 –15 increases wound tensile strength 16 and microcirculation; 17 and prevents cell/tissue death. 18–19 In addition, it was shown that LLLT is able to restore trachea smooth-muscle relaxation in an ex vivo model of tumor necrosis factor α-mediated airway muscle dysfunction, 20 and improves cartilage healing. 21 In spite of these facts, LLLT has never been used, either experimentally or clinically, as a possible treatment for trachea wound healing.
Previously, effects of 665-, 675-, and 810-nm laser light on the proliferation of fibroblasts and endothelial cells were compared. It was found that fibroblasts proliferated faster than endothelial cells in response to laser irradiation. The highest proliferation of fibroblasts after a single exposure of laser light at an energy density of 10 J/cm2 occurred at 665 and 675 nm, while irradiation at 810 nm inhibited proliferation. Endothelial cells showed increased proliferation after exposure to all wavelengths, with highest proliferation at 655 nm and with the smallest increase at 810 nm compared to untreated controls. 22 Accordingly, it may be suggested that the infrared laser irradiation may be a valuable tool in trachea wound healing modulation. During the therapy, acceleration of granulation tissue remodeling by means of earlier decrease in vascularity leading to acceleration of new cartilage formation from progenitor cells, needs to be achieved to prevent airway occlusion development. From this point of view, higher doses (20 J/cm2 and more) 23 need to be tested in an attempt to find an optimal therapeutic strategy for trachea healing modulation.
Moreover, it is known that longer wavelengths are associated with a greater depth of penetration. 24 As most of the LLLT-target cells/tissues of trachea are located deeper under the skin and subcutaneous tissue, we selected an infrared laser to be tested in our study instead of a red one. In our previous study, we found that a single point dose of 30 J/cm2 is able to improve skin wound healing by reducing inflammation without compromising re-epithelization and/or granulation tissue formation. 25 In a study using 0.784 mm thick human skin irradiated with 850 nm laser, the intensity of the radiation was reduced by 66%. 26 As trachea is located deeper under the skin, only a fraction of the energy (∼33%) reaches the target tissue. Therefore, in this present investigation, from a histological point of view, the effect of an LLLT at 830 nm and 60 J/cm2 on trachea wound healing in rats was investigated.
Materials and Methods
Animal model
This experiment was approved by the Ethical Committee of the Faculty of Medicine of Pavol Jozef Šafárik University and by the State Veterinary Administration of the Slovak Republic.
One year old male Sprague-Dawley rats (N = 24) were included in the experiment. Surgery was performed with all rats under general anesthesia induced by administration of ketamine (40 mg/kg; Narkamon a.u.v., Spofa, Prague, Czech Republic), xylazine (15 mg/kg; Rometar a.u.v., Spofa, Prague, Czech Republic) and tramadol 5 mg/kg (Tramadol-K, Krka, Novo Mesto, Slovenia). Rats were randomly divided into two groups: laser-treated group and sham-irradiated control group.
Prior to tracheotomy each rat was intubated (the tip of the intubation cannula was 2–3 cartilage rings deeper than the caudal end of the incision). Under aseptic conditions, skin and subcutaneous tissue were incised and strap muscles were separated and retracted laterally to gain access to the front tracheal wall. A median incision, ∼8 mm in length, was then performed using a scalpel (blade no. 15) from the second to the sixth tracheal cartilage ring. Subsequently, the incision was closed using two simple interrupted sutures that were placed on the third and fifth cartilage ring (Chiraflon 6/0, Chirmax a.s., Prague, Czech Republic). The surgical wound was then closed in anatomical layers. After surgery all rats were extubated.
Twelve rats were killed by ether inhalation 7 and 28 days after surgery, respectively.
LLLT
The whole incisions of laser-treated rats were daily, for at most 7 days, irradiated in a contact mode in one point with a commercially available GaAsAl diode laser (Maestro/CCM, Medicom Praha, Prague, Czech Republic; λ = 830 nm; laser beam oval – spot size ∼1 cm2, power density 450 mW/cm2, daily dose 60 J/cm2, irradiation time 133 sec). During treatment, irradiated rats were restrained in a Plexiglas cage with an oval opening beneath stimulated trachea, whereas the control rats were sham irradiated for the same time period as laser treated rats. The laser output power was measured before and after each experiment and remained stable during the whole experiment.
Histology
Tracheas were removed from six control and six laser-treated rats killed 7 and 28 days after surgery, respectively. Specimens were routinely processed for light microscopy (fixation, dehydration, paraffin embedding, sectioning, and staining). Paraffin sections made from the injured tissue that was placed between the two sutures were used for histological examination. Slides were stained with hematoxylin-eosin (HE – basic staining) and van Gieson (VG – non-specific collagen staining).
Morphometric and semi-quantitative evaluation of histological sections
Areas of the granulation tissue were measured in one section removed from each animal. The specimen analysis was performed using the Olympus BX51 microscope (Olympus, Tokyo, Japan) with DP71 CCD camera and QuickPHOTO MICRO 2.2 (Promicra, Prague, Czech Republic) software. Data are expressed as mean ± standard deviation (SD).
A semi-quantitative method was used to evaluate re-epithelization; presence of inflammatory cells (polymorphonuclear leucocytes [PMNL], monocytes/tissue macrophages [M/TM]); presence of chondroblasts; presence of newly formed vessels. Sections were evaluated in coded slides by two examiners according to the scale 0, 1, 2, 3 (Table 1).
Statistical analysis
Median values were calculated for the semi-quantitatively evaluated histological parameters. A non-parametric Kruskal–Wallis test was employed to compare the semi-quantitative data. Mean ± SD values were calculated for the morphometric data. The unpaired Student's t-test was used to compare the morphometric data. For both tests significance was accepted at p < 0.05.
Results
During the postsurgery period, animals remained healthy, without clinical evidence of infection and/or airway occlusion. The results of our histological investigation are summarized in Fig. 1.
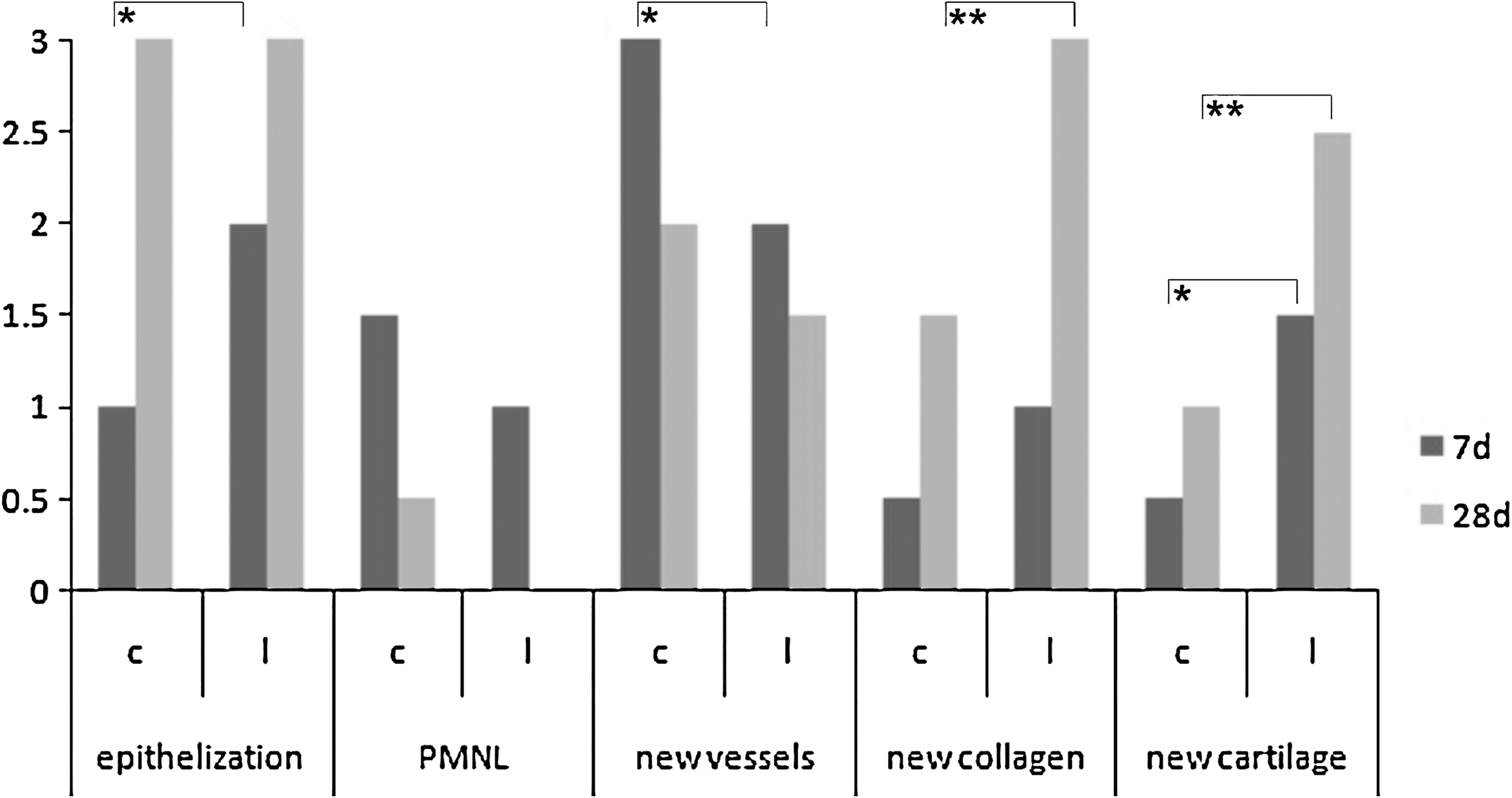
Semi-quantitative evaluation of histological sections. Data are expressed as median (PMNL—polymorphonuclear leukocytes; *p < 0.05; **p < 0.01).
Seven days postsurgery
In both control and laser-treated tissues, the proliferation phase was prominent 7 days after surgery. The number of PMNL was minimal, therefore the inflammatory phase was almost finished in both groups. The granulation tissue in control animals was rich in new vessels and mesenchymal cells (Fig. 2a). Interestingly, a significantly lower amount of granulation tissue was observed after LLLT (Fig. 2b and 3). The regeneration of tracheal epithelium was not yet finished as cells did not always completely bridge the wound. In contrast, in laser-treated animals in most cases the wounds were bridged by cylindrical ciliated epithelium. In contrast to sham-irradiated control tracheas, the laser-treated tissues started to produce new cartilage in a significantly higher amount (Figs. 1, 2a, and b).
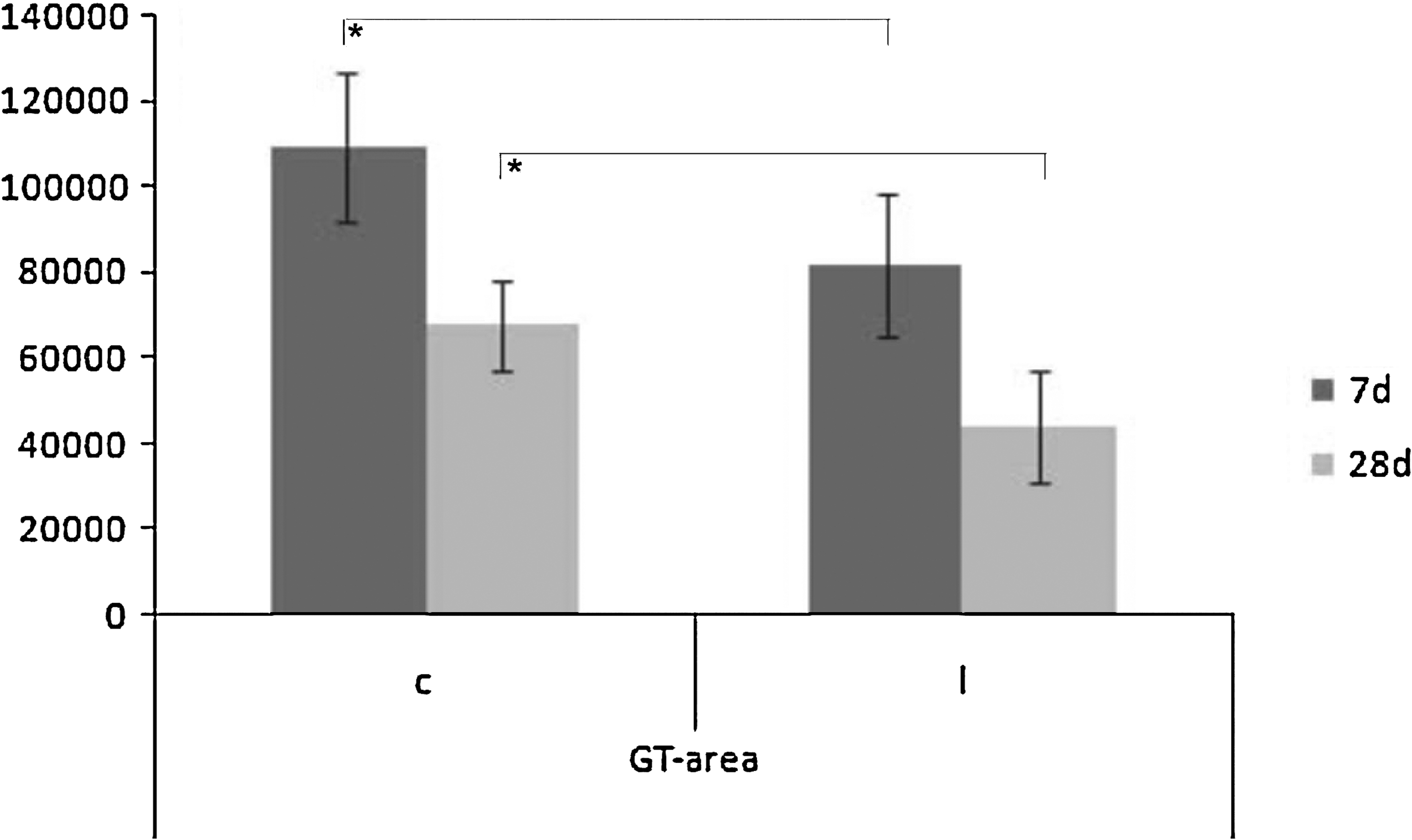
Morphometrically measured granulation tissue area in μm. Data are expressed as mean ± SD (*p < 0.05).
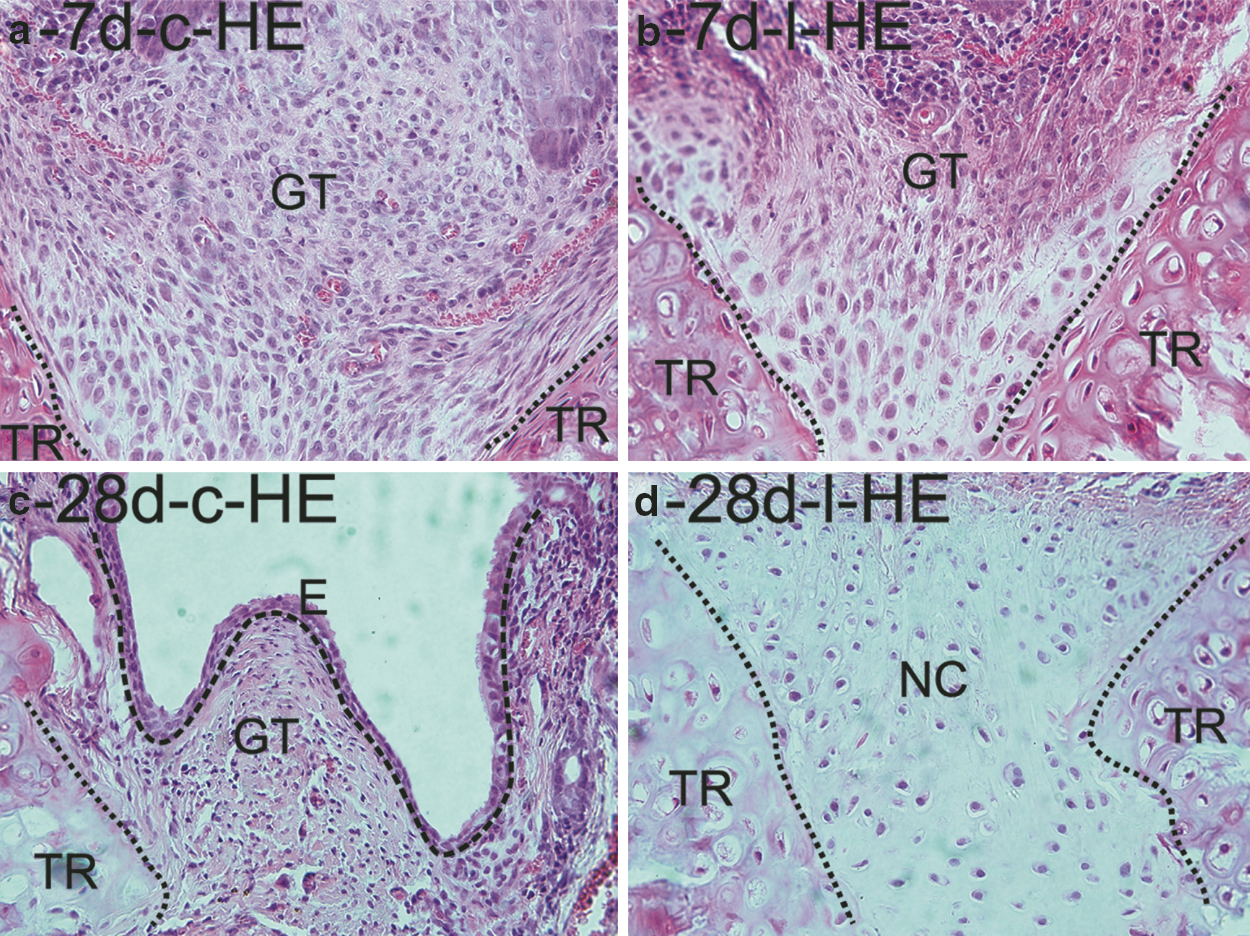
Histological sections of healing tracheas at 7 and 28 days [(
Twenty-eight days postsurgery
A month after surgery the inflammatory phase was completely finished in both groups, therefore, the maturation phase of healing was observed. The regeneration of epithelium was completely finished in both laser-treated and sham-irradiated control animals. Accordingly, cylindrical ciliated epithelium was present over each wound. Only a minimal number of newly formed vessels was present in the granulation tissues of wounds (Fig. 2c). The granulation tissue area was significantly smaller in laser-treated animals when compared with their control (Fig. 3). The second main difference between laser-treated and control animals was observed in new cartilage formation, as this process was significantly accelerated in laser-treated rats (Figs. 2c and d, and 4c and d).
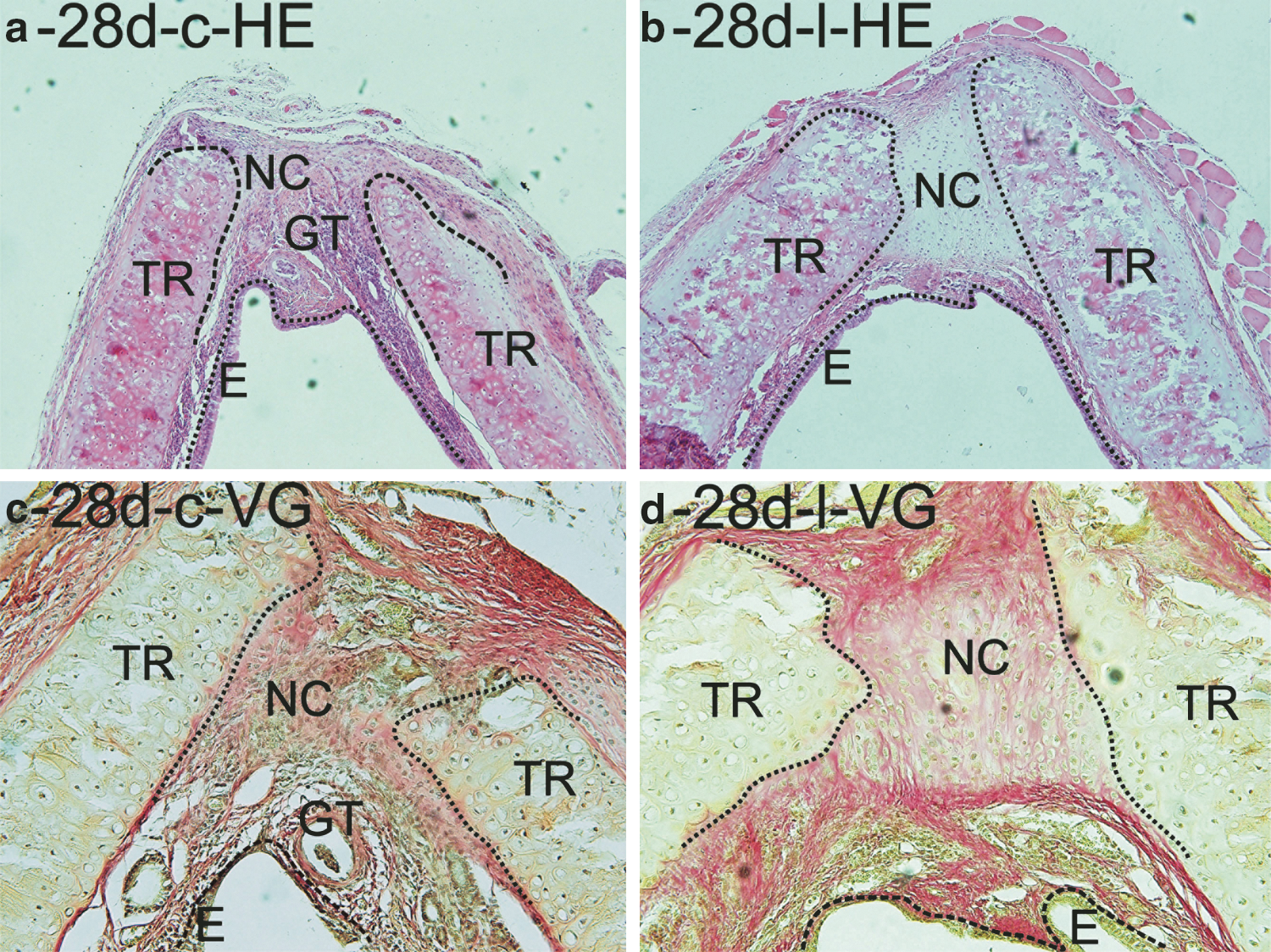
Histological sections of healing tracheas 28 days after surgery [(
Discussion
The exact mechanisms at the cellular level by which LLLT stimulates tissue repair and regeneration are still not fully clarified. Nevertheless, it has been demonstrated that the therapy effect depends upon adjustment of basic laser parameters, such as wavelength, power density, and dose. The wavelength used in the present study was within the ideal wavelength range identified by Karu as being near 760, 810, and 840 nm, becausee in those bands of the electromagnetic spectrum, superficial chromophores have weak absorption, and therefore, there is greater energy penetration through the skin. 27 Deeper penetration of light results in stimulated microcirculation and lymphatic drainage. 17 This observation might be the main reason why in clinical practice, near infrared lasers are the most frequently used light sources for deep injuries. 28,29
Among infrared lasers it has been documented that GaAIAs laser of 904-nm wavelength (33 J/cm2) accelerated the inflammatory process and epithelization, and positively influenced collagen deposition in healing skin wounds on both steroid-treated and non-treated rats. 30 Kawalec et al. reported a beneficial effect of laser treatment at low levels with the 980-nm GaAlAs diode laser at 18 J/cm2 on wound healing in diabetic mice, however, treatment with 36 J/cm2 decreased the healing process. 31 Moreover, it was shown that LLLT at 904 nm stimulates condylar growth, which was demonstrated by both increased chondrocyte proliferation and extracellular matrix formation. 32 Similarly, 830-nm GaAlAs (5 and/or 15 J/cm2) diode laser stimulated chondrocytes proliferation in epiphyseal cartilage thickening model in vivo, but did not induce changes in bone length. 33 We found that LLLT at 830 nm (60 J/cm2) improves trachea wound healing. The therapy significantly stimulated new cartilage formation and simultaneously reduced granulation tissue formation at both evaluated time intervals. However, it has been shown that ∼66% of the radiation is absorbed within the first 1 mm of skin. 26 Accordingly, we may suggest that even a higher dose to that used on epiphyseal cartilage 33 stimulated trachea healing in our current investigation, which correlates with our previously published data on the effect of LLLT on wound healing using a skin incisional model. 25
In vitro studies are performed either to better understand the biological processes/mechanism of LLLT on the cellular level or to perform preliminary experiments prior to animal and human studies. Mesenchymal cells, such as fibroblasts, chondroblasts, and/or osteoblasts, play an important role in wound healing and therefore are considered as target cells of LLLT in many studies. In this context Guzzardella et al. in his ex vivo study with a GaAlAs laser with 780-nm laser radiation (300 J/cm2) observed positive effects of LLLT on bone tissue healing. 34 Positive effects of 809-nm diode laser radiation (1.96–7.84 J/cm2) on human gingival fibroblast (HGF) was documented, as well. When compared with the control, irradiated HGF revealed a considerably higher proliferation activity after a single irradiation. 35 Moreover, an in vitro study showed that laser irradiation at 632.8 nm (4–6 J/cm2) stimulates chondrocyte proliferation and extracellular matrix production, which is in agreement with our results obtained in the presented in vivo experiment. 36
Based on all these observations, LLLT should be tested in further preclinical and clinical research, as a potentially positive modulatory approach, which could eventually prevent stenosis development and simultaneously accelerate cartilage healing in humans. Furthermore, economics play an important role at the present time. We may hypothesize that the demonstrated procedure could shorten the hospitalization time and, therefore, reduce costs per patient, which has already been shown by a multidisciplinary approach. 37
Conclusions
In conclusion, LLLT treatment at 830 nm (power density 450 mW/cm2, daily dose 60 J/cm2) was demonstrated to be a valuable tool in modulating trachea healing. Nevertheless, a correlation to the clinical situation would be possible only if no inter-species variability would exist. Therefore, presented results cannot unambiguously be extrapolated to the clinical situation. Further detailed investigations of LLLT parameters in other animal models are therefore encouraged by our study in the rat model.
Footnotes
Acknowledgment
The authors thank Professor Richard L. Magin, Ph.D. (University of Illinois at Chicago) for his editorial help in preparing the manuscript. This study was supported by Pavol Jozef Šafárik University (VVGS 53/09-10 and 54/09-10).
Author Disclosure Statement
No competing financial interests exist.