
Abstract
Introduction
The muscle degeneration during aging has been associated with the mitochondrial dysfunction caused by the deletions in mitochondrial DNA (mtDNA) and an abnormal electron transport system with progressive shortening of telomeres and proliferative exhaustion of satellite cells. 3,6 However, phototherapy improves cellular activation via absorption of photons by chromophores present in the protein components of the mitochondrial respiratory chain – mainly NADH dehydrogenases and cytochrome C oxidase, which leads to increased electron transport, production of ATP, and tissue regeneration (skin, muscle, bone, and peripheral nerves). 7,8
The imbalance between reactive oxygen species (ROS) production and antioxidant capacity leads to a phenomenon in which the skeletal muscle of aged subjects becomes more susceptible to oxidative damage, mainly during physical exercise, as a result of mitochondria dysfunction. 9 It can result in inflammation, delayed-onset muscle soreness (DOMS) and muscle degeneration. 10 However, phototherapy stimulates the anti-inflammatory effect with analgesia and vasodilatation, 7 which can help reduce pain in muscles and articulations, so that physical exercises can be performed without difficulties.
High intensity treadmill training results in cardiovascular and osteomuscular improvement, 2 but also generates ROS. ROS not only are toxic but also play an important role in cell signalling and in the regulation of gene expression. These signals result in an upregulation of powerful antioxidant enzymes that can enhance muscle force and fatigue resistance. 11 Moreover, phototherapy has not only shown to reduce the release of ROS 12 but has also shown to generate ROS 13 that may increase antioxidant defense, 14 potentiating the effect of physical exercise.
Devices used for phototherapy, e.g., lasers and light-emitting diodes (LEDs) emit light with very specific properties. Whereas lasers are monochromatic and coherent and preserve collimation during propagation, the light originated from LEDs is neither coherent nor collimated and covers a much broader range of wavelengths. The advantages of LEDs versus lasers is that LEDs have a comparably low operational cost, allow irradiation of larger areas, 15 and can be configured to produce multiple wavelengths 7 with an absorption of photons by several chromophores. 16
A review of the literature shows that phototherapy has only been applied before 17 –21 or after 22 –24 physical exercise to enhance muscle performance. In a recent study, Ferraresi et al. 24 showed that the strength training associated with phototherapy (laser with six diodes, 850 nm) applied during 3 months, increased quadriceps performance. However, the cardiovascular adaptations to exercise performance remains to be investigated.
The objective of this study was to develop and evaluate the effects of a new clinical procedure: infrared radiation originated from LEDs associated with treadmill training in postmenopausal women. LED arrays were developed for an irradiation of a large area, such as hip and quadriceps muscles, main actuators during stance and swing phases. These body parts are furthermore areas where there is incidence of osteoporosis, mainly at the femur, localized fat deposits, and cellulite. Infrared radiation (850 nm) was selected because this spectral range shows better skin penetration compared to red interval.
Our hypothesis is that the infrared-LED illumination during treadmill training can enhance physical performance, as evaluated by the endurance exercise testing on a treadmill and strength exercise testing in postmenopausal women. The basis for such a hypothesis is based on the fact that the light therapy during the intense metabolic stage caused by exercise may be more efficient.
Materials and Methods
The current research has been approved by the National Ethics Committee of Ministry of Health in Brasilia, Brazil and by the Ethics Committee of Federal University of São Carlos (UFSCar) in São Carlos, Brazil. All subjects signed written informed consents before their participation in the study.
Subjects
This study was performed in 20 postmenopausal women, who were Caucasian, aged between 50 and 60 years, and non-users of hormone replacement therapy (the postmenopausal period was defined by absence of menstruation for more than 12 months). Subjects who had neurological, metabolic, inflammatory, endocrinopathic, pulmonary, malignant, and heart diseases were excluded from this study. The participants were instructed not to change their eating habits for the duration of this study.
The postmenopausal women were randomly divided into two groups: (a) the LED group that performed treadmill training associated with infrared-LED illumination (n=10), and (b) the control group that performed only treadmill training (n=10).
Phototherapy and treadmill training
For the phototherapy to be performed during treadmill training, the Optics Group from Instituto de Física de São Carlos (IFSC), University of São Paulo (USP), developed one system based on infrared-LEDs to be used during the physical exercises (Fig. 1).
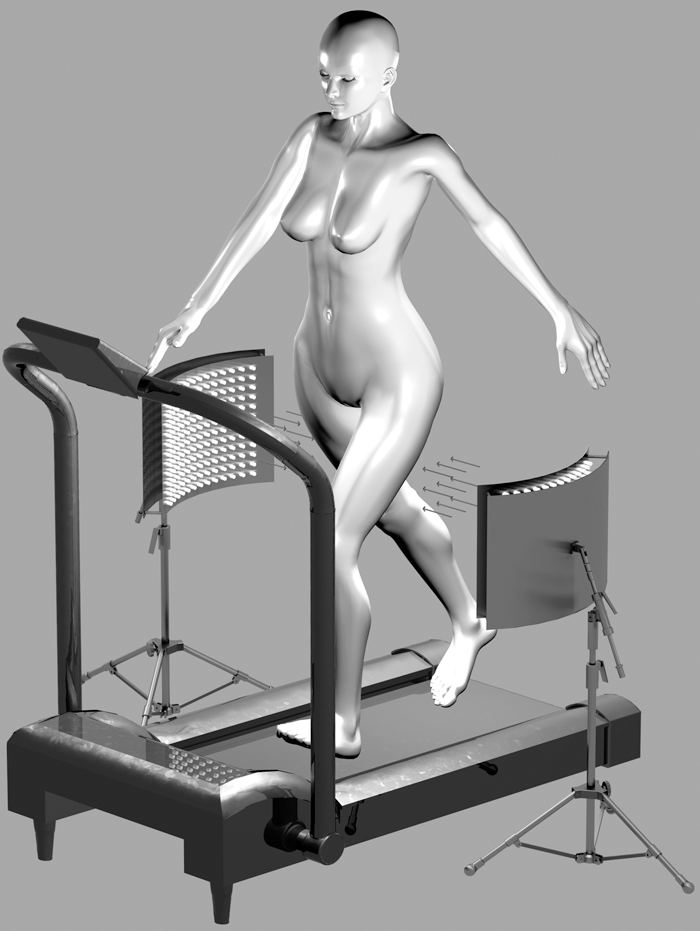
New clinical procedure combining infrared-LED with treadmill training.
Each illumination device with an area of 1110 cm2 has 2,000 LEDs (850 nm, Everlight Eletronics Co. Ltd., Taiwan, China). The LED array is angled and has a curvature radius of 57 cm with adjustable height and portability to allow adjusting the distance. We used the traditionally delivered dose in phototherapy. A power meter fieldmaster (Coherent Inc., Santa Clara, CA) in the milliwatt range was used. The average power density near the emitter was ∼28 mW/cm2. The distance between the LED devices and the volunteers' skin was 15 cm and the average power density on the skin was 31 mW/cm2. This small increase of the intensity at the skin surface occurred because of the geometry of the LED array. The curvature resulted in a small focusing effect of the light (as in curved mirrors) causing the observed increase of the power density. The treatment time was 30 min performed bilaterally on thighs. These parameters led to ∼14,400 J overall irradiation energy and a fluence of 55.8 J/cm2. The total energy delivered per limb is estimated to be 7,200 J.
The volunteers wore safety glasses and swimwear to ensure infrared absorption through the bare skin during the treadmill training with infrared-LED.
Treadmill training with and without phototherapy was performed twice a week, for 3 months. Each session lasted 30 min. The training began with low intensity and was gradually performed until reaching a high intensity, 85–90% maximal heart rate (HRmax) obtained during a previous maximal exercise testing. To monitor the HR during the training a cardio frequency meter monitor (Polar A3, Polar Electro, Inc., Woodbury, NY) was used. The values of HR are presented as mean values and standard deviations. The initial phase refers to the adaptation of physical training and it was maintained for 3 weeks [LED group: HR=125±9 beats/min (bpm) and control group: HR=124±9 bpm]. Subsequently, the treadmill speed was increased (LED group: HR=134±7 bpm and control group: HR=133±9 bpm) and the intensity was maintained for 3 weeks. After this period, the speed was increased again (LED group: HR=148±5 bpm and control group: HR=145±9 bpm) and was maintained until the end of the training.
Evaluations were performed on the baseline and after 3 months and each evaluation was made on different days. As heart disease was an exclusion criteria, the electrocardiogram (ECG) and clinical evaluation were performed first. In the second week and on different days, body composition and submaximal constant-speed testing were performed, and in the following week, the concentric isokinetic exercise testing was performed.
Assessment HR at rest and during maximal effort testing
Under cardiology medical surveillance, the volunteers underwent evaluation of a 12-lead conventional ECG (Ergo, HeartWare Ltda, Belo Horizonte, MG, Brazil) in resting and ergometric test. For the maximal effort test using the treadmill, continuous function protocol (Modified Bruce Protocol) was used. 25,26 The initial stage was set at 0% of inclination and speed of 1.7 mph or 2.7 Km/h. Two stages later, the slope was increased to 5% and the rate kept at 1.7 mph (2.7 Km/h). From the third to the seventh stage the tilt was increased 2% and the speed was 0.8 mph (1.28 Km/h) and 0.5 mph (0.8 Km/h) from the seventh to the ninth stage. Each stage lasted 3 min. R-R interval was continuously registered during all tests in a ECG monitor. The test was stopped if the patient showed signs and/or limiting symptoms or when it reached the HRmax for the patient's age.
Submaximal constant-speed testing
The test began with 5 min of rest with the subject in a sitting position. After this, the subjects started the exercise on a treadmill with constant speed 27 (85% HRmax and 15° tilt). The subject performed the exercise up to the maximal time of tolerance (Tlim) or to a maximum of 20 min when evaluated after 3 months of the treadmill training. The HR was measured using the cardio frequency meter monitor (Polar S810i).
Isokinetic concentric exercise testing
Peak torque, power, work, and fatigue of the dominant quadriceps were measured using the isokinetic dynamometer 28 (Biodex Multi Joint System III, Biodex Medical Systems Inc., New York, NY). Prior to the test the load cell was properly calibrated using standard weight and dynamometer lever arm horizontally positioned and stabilized in relation to the ground, according to the manufacturer's recommendations. Positioning and stabilization of the participants was standardized and the tests were applied. Protocol 1 for the analysis of the maximum isokinetic strength: the participants performed five maximal efforts to determine maximal peak torque (N.m) at low angular velocity (ω) of 60°/s. Protocol 2 for the analysis of the isokinetic endurance: the subjects performed efforts during 1 min at high angular velocity of 300°/s to determine average power (W), total work (J) and fatigue index (%). The muscle fatigue was determined by the following formula: Percent decrease=100 – [(work last third/work first third) × 100].
Body composition assessment
To evaluate the body composition, anthropometric measurements and bioelectrical impedance were performed. The anthropometric evaluation 29 consisted of performing measurements of height in centimeters (cm), body mass in kilograms (kg) and the anatomical landmarks to measure the circumference (cm), in the upright position of the body were: (a) waist: measured at the midpoint between the lowest rib and the iliac crest.; (b) hip: measured at the level of maximum extension of the buttocks. 30 Anthropometric data were used to determine the body mass index [BMI: body weight (in kg) divided by height (in m) squared] and the waist-hip ratio [waist (in cm) divided by hip (in cm)]. 29 –31 For measurement of body fat and lean mass, the bipolar impedance of the upper limbs (OMRON®, Kyoto, Japan) 31 was performed, and the participants were instructed not to exercise, not to use metals in the body, and to maintain normal hydration status.
Statistical analysis
Measurements were expressed by mean and standard deviations. The Shapiro–Wilk test was used to analyze the normality. Two-way repeated measures ANOVA with Bonferroni adjustments were used to compare changes before and after treatment. The Δ between situations before and after the treatment (post-pre=Δ) was used to compare groups via one-way ANOVA with Bonferroni adjustments. Data were analyzed using Statistica for Windows Release 7 software (Statsoft, Inc., Tulsa, OK) and the significance level was set at 5% (p<0.05).
Results
Baseline characteristics, HR at rest and during maximal effort testing
The mean values and standard deviation were 55±3 years old for age, and 9±6 years for the duration of menopause. The values of HR baseline and HRmax for the LED group were 73±9 and 162±11 bpm, and for the control group were 74±9 and 153±17 bpm, respectively. The Bruce protocol stage reaching was 3±0.5 for the LED group and 2.5±0.5 for the control group.
Submaximal constant-speed testing
The mean value of the speed in the submaximal test for the LED group was 5.9±0.6 km/h and for the control group it was 5.4±0.9 km/h. There was a significant increase in Tlim after 3 months of treatment for both groups (LED group: from 3±1 to 9±4 min [p=0.001] and control group: from 3±7 to 7±4 min [p=0.01]). No significant difference was found between the groups in the Δ change between post- and pretreatment (p≥0.05).
Isokinetic concentric exercise testing
The results of the isokinetic concentric exercise testing during the dominant knee extension in ω=60°/s and the fatigue test results in ω=300°/s are shown in Table 1. There was a significant increase in average power (p=0.002) and total work (p=0.006) for the LED group, but not for the control group (p≥0.05). There was also a significant increase in fatigue for the control group (p=0.04), whereas the LED group maintained the fatigue index (p≥0.05). No significant difference was found between the groups in the Δ change between post- and pretreatment (p≥0.05), except for the results of average power (p=0.04) for LED group (Fig. 2). Negative values in the Δ (average power) for the control group can be seen in Fig. 2.
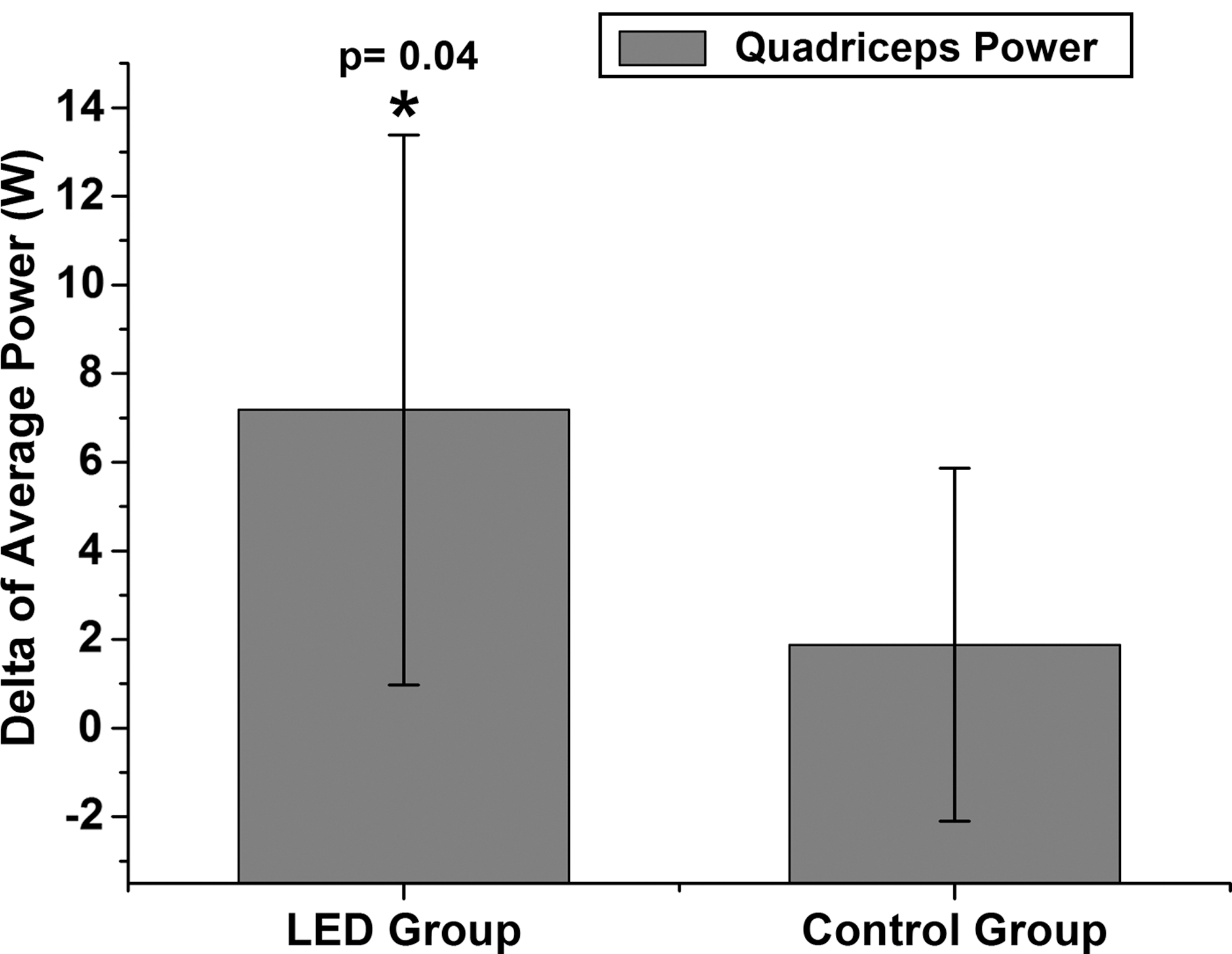
Δ of average power between post- and pretreatment.
Significant difference for pre- vs posttreatment (repeated measures ANOVA with Bonferroni adjustments, p<0.05).
Significant difference for pre- vs posttreatment (repeated measures ANOVA with Bonferroni adjustments, p<0.01).
Body composition assessment
There was no significant difference in body composition results for either group (Table 1).
Discussion
This is the first study evaluating the effects of infrared-LED illumination associated with treadmill training in postmenopausal women. The main findings were that in these women the association of LED illumination with treadmill training improved peripheral strength without producing fatigue of the quadriceps. These results suggest that LED illumination with treadmill training could be used as an aid during high-intensity physical exercise for postmenopausal women. In addition, treadmill training associated or not associated with LED can improve the submaximal performance of these subjects.
Submaximal constant-speed testing
Both groups significantly improved submaximal exercise performance, as shown by the increase in Tlim for both groups. These results can reflect beneficial adaptations promoted by treadmill training, 27 independent of the LED illumination. Our findings showed potential effects of the phototherapy on anaerobic performance during isokinetic endurance compared to aerobic performance via submaximal constant-speed testing. Studies with phototherapy showed formation of the giant mitochondria 32 that may contribute to the greater energy availability in high-intensity exercise. 24 This is based on the hierarchical and ramp recruitment of the muscle fibers (from oxidative fibers to glycolytic fibers), as well as the fact that the aerobic energy production (oxidative) is supplemented by anaerobic energy production (glycolytic) as exercise becomes more intense. 24
Isokinetic concentric exercise testing
There were no significant changes in the peak torque of the knee extensor for either group. However, the peak torque is an indicator of the muscle's strength capabilities and shows generally significant increases caused by muscular resistance training. 33
The increase in muscle power found in the LED group indicates greater functional capacity to generate force quickly over time during motor tasks requiring consecutive muscle actions (in particular concentric muscle contractions, such as stair climbing and walking or running) with reduced fatigue compared to the control group. In this context, the present study is very important, because the decline in fast powerful movements with aging requires less recruitment of fast motor units that may contribute to a loss of these motor units (type II) with muscular degeneration and fatigue. 34
The therapeutic effects of phototherapy on the neuromuscular system can generate reinnervation 35 with early functional nerve recovery, 36 as well as muscle regeneration. 37 Moreover, the high-intensity training requires use of aerobic and anaerobic metabolism with recruitment of oxidative slow-twitch muscles (type I) and glycolytic fast-twitch muscles (type II). 38
Peripheral fatigue is an exercise-induced reduction in maximal voluntary muscle force-generation capacity with metabolic, ionic, and electrical changes at or distal to the neuromuscular junction. 39 Therefore, fatigue prevention observed in the LED group can be related to the increased power and work of quadriceps. Moreover, the negative difference between pre- and posttreatment power values indicates that some women in the control group did not improve quadriceps power, and it may explain the increase of fatigue in the control group.
The increase of physical performance has been investigated in several studies that showed the immediate effect of phototherapy (laser or LED) applied to athletes before exercise, such as increasing the number of contractions 17,18,20 and the decrease of blood lactate (BL), 19,20 creatine-kinase (CK) and C-reative protein levels 20 postexercise. Similar results in CK 23,40 and BL 40 levels were found in a study with rats.
Furthermore, another study shows the failure of the results (number of contractions and BL levels), whereas a positive result was the reduction of CK only in the group subjected to the application of LEDs (660/850 nm), because the large area irradiated with LEDs was compared to fewer points irradiated with laser (810 nm). 21 These results are important because they show that the irradiated area is vital to improving physiological responses after a high-intensity physical exercise, and our new procedure allows the irradiation of a large index area.
LED based devices constitute an attractive alternative for phototherapy. The emission is not monochromatic, nor coherent. Concerning monochromaticity, is narrower than most absorption bands of endogenous chromophores 42 and therefore no energy is irrelevant. In fact, studies comparing the action of lasers and LEDs operating at equivalent fluence rates, show that they produce equivalent effects. 42 Concerning coherence, certain studies 7,21,43 have shown that this property of the light source is not exclusively responsible for cellular response or that it has only little influence on the outcomes for phototherapy. 44,45
Although we only used infrared radiation, many studies have used multiple wavelengths 7,21 through devices that contain many different LED emitters. The idea in these cases is that different wavelengths can act on different sites of the tissue. 16,41 For example, red light acts on mitochondria whereas infrared acts on membrane of mitochondria and the combined effect can be of advantage for the final biostimulation. For any multiple wavelengths used, LEDs will be easier to be implemented than laser, because the present technology allows for production of a large variety of wavelengths, not yet possible for lasers. 7,46 According to Enwemeka, 47 “treating patients with appropriate wavelengths of polychromatic light or a combination of red and infrared wavelengths offers the following advantages: (a) the ability to effectively treat deep and superficial lesions simultaneously, and (b) the ability to cover a broader spectrum of the therapeutic window of wavelengths for tissue repair and pain relief; which, based on the literature, appears to lie within the 600–1000 nm range”.
Body composition assessment
LEDs plus treadmill training or exercise alone did not promote changes in body composition. During the aging process loss of muscle and accumulation of fat (subcutaneous abdominal, intramuscular, and visceral—for example heart and liver) occurs. 4,5 However, both groups showed maintenance of lean mass, body fat, BMI, waist circumference and waist-to-hip ratio. These data are important for the prevention of cardiovascular diseases. The high-intensity aerobic training is believed to increase the calorie intake as a compensatory mechanism to increase metabolic rate, resulting in maintaining and even increasing of fat percentage, 48 except when a low-calorie diet is imposed. 31 However, clinical studies that investigate the reduction of fat mass are difficult because they require diet control and monitoring. Therefore, future animal studies with phototherapy and exercise should be performed.
Conclusions and Summary
The current study showed that the developed infrared-LED device associated with treadmill training can be useful in improving outcomes related to muscle power and leg fatigue for postmenopausal women. In this context, we considered that a phototherapy associated with treadmill training can be potentially used for sports and rehabilitation protocols where the main objective is muscle strength. Moreover, LED arrays can be considered as an efficient alternative to the use of lasers. Future studies will be performed to investigate morphological and cellular adaptations of infrared-LEDs associated with physical exercise and will try to investigate other physiological outcomes.
Footnotes
Acknowledgments
The authors acknowledge the Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP) – Grant no. 98/14270-8 and 05/59427-7, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
This study was published in part at the Latin America Optics and Photonics Conference (LAOP), September 27–30, 2010, Golden Tulip Recife Palace, Recife, Brazil.
Author Disclosure Statement
No competing financial interests exist.