
Abstract
Introduction
In the last decade, the spectrum of treatments available for varicose veins has broadened with the introduction of minimally invasive treatment modalities, such as radiofrequency ablation, endovenous laser ablation (EVLA), and ultrasound-guided foam sclerotherapy. In particular, EVLA has been shown to be a highly effective technique with prominent occlusion rates. 2 –5
The aim of this prospective non-randomized study is to evaluate our results performing the EVLA procedure and to assess its safety and effectiveness in the ambulatory setting.
Methods
Patients
This prospective non-randomized study included symptomatic patients who underwent EVLA in our hospital between February 2008 and May 2010. All patients had great saphenous veins
A single cardiovascular surgeon (M.U.E.) saw and examined all patients. The principal examination included a detailed history of disease, a focused physical examination, and venous duplex ultrasound imaging. The patients with SFJ and GSV insufficiencies were evaluated as pre-candidates for EVLA. The patients who were excluded from the study included those patients with occlusive arterial disease, patients with a known thrombotic disease or hemorrhagic tendency (including oral anticoagulation use), patients with an inability to ambulate, and women who were pregnant or planning to become pregnant. The clinical, etiological, anatomical, and pathophysiological (CEAP) classification of varicose veins was determined for all patients. 6 In total, 98 patients (103 limbs) were included in the study.
Venous duplex ultrasonography examination was performed by the radiology department on each patient before and after their treatment (Acuson®, Malvern, PA, Siemens ultrasonography system, 5–12 MHz linear probe). Deep, superficial, and perforating venous systems were evaluated. The veins were examined with the patient in an upright position to determine venous reflux, which is defined as retrograde flow of >0.5-sec duration. 7 Patients with deep vein insufficiency as demonstrated by the venous duplex ultrasonography were not included in the study.
Procedure of EVLA
For all cases, a 600-μm ELVeS-plus kit (Biolitec AG, Jena, Germany) was used; the kit is suitable for the 980-nm diode laser (Biolitec AG, Germany). This kit consists of a bare fiber, a 70-cm guiding catheter with controlled pullback and guidance markings for cm, a 5-Fr sheath, an 0.035-J tip guidewire with length of 150 cm, and a 19-gauge entry needle.
The course of GSV, branch varicosities, and perforating veins were identified by inspection while the patient was in the upright position, and were marked on the skin with a surgical pen. For all cases, EVLA was performed along with general or local anesthesia using tumescent solution. The leg was disinfected with a povidone-iodine solution and was then covered with sterile cloths. Similarly, the transducer probe (8–10 MHz linear) of the ultrasonography machine was disinfected with the povidone-iodine solution and placed in a sterile sheath. The GSV was inserted at knee level via a percutaneous needle puncture (19-gauge, Seldinger technique) under ultrasound guidance. In case of tortuosity of the GSV, a 2–3-cm incision was made over the GSV to facilitate the procedure. A 5-Fr sheath was then passed over the J-tip guidewire 2–3 cm below the SFJ. Once we confirmed the position of the sheath with ultrasonography, a 600-μm bare-tipped laser fiber was inserted. The distal tip of the laser fiber was positioned 2–3 cm below the SFJ; we confirmed its position through ultrasound guidance and direct visualization of the red aiming beam of the laser fiber, which can be seen through the skin at the groin crease.
A tumescent local anesthetic solution was given, which consists of 35 mL of 1% lidocaine, 5 mL of sodium bicarbonate, and 5 mL of epinephrine (1:100,000) diluted in 500 mL of cooled (+4°C) saline. Under ultrasound guidance, the anesthetic solution was administered along the perivenous space using the Klein peristaltic infiltration pump (HKSurgical, Inc., San Juan Capistrano, CA).
During activation of the laser, those in the treatment room wore protective laser goggles. The linear energy density (LEED) value, which is the energy in joules divided by the treated vein length in centimeters, was used in the procedure. 8 LEED values were used to calculate the laser energy, and these LEED values were based on the GSV diameter, which was measured 1.5–2 cm distal to SFJ. For GSV diameters between 4.5 and 6.9 mm, 60–70 J/cm of energy was used; for GSV diameters between 7 and 10 mm, 80–90 J/cm of energy was used. Laser energy was delivered endovenously in a continuous fashion. The Trendelenburg position and manual compression over the treated vein segment were used to help increase vessel wall contact with the laser heat. The laser energy delivery began 2–3 cm below the SFJ to prevent thrombus propagation into the deep vein system. The laser fiber was slowly withdrawn at a velocity of 1 mm/s until it reached a distance of 2–2.5 cm from the puncture site of the GSV at the knee level. Following laser ablation of the GSV from the groin to the knee, we made minimally invasive stab incisions of 2–3 mm over the previously marked branch varicosities if necessary. Ambulatory phlebectomy (Muller avulsion method) was then performed using Muller's hook. Minimal invasive incisions were closed with Steri-strips or 5/0 Prolene (Ethicon, Somerville, NJ), and sterile dressings were applied. Then, an elastic compression bandage was applied and kept over the length of the treated vein for 48 h. After patients were transferred to the recovery room, they were encouraged to ambulate immediately in accordance with the hospital sedation protocol. A thigh-high, class II graduated compression stocking (35–40 mm Hg) was applied for 6 weeks except when the patients were sleeping or showering. All patients were discharged on the day that the procedure was performed.
Diclofenac sodium, a non-steroidal anti-inflammatory medicine, was prescribed (100 mg, 5 days, twice daily, orally), and patients were instructed to use it routinely for 5 days after hospital discharge. The patients were told to avoid strenuous exercise for ∼2 weeks.
Assessment of outcome
All patients were followed up on an outpatient basis. If there were no complications, the first routine post-ablation evaluation was performed the first week after the patient was discharged. Subsequent follow-ups, which included clinical examination and venous ultrasound imaging, were performed at 3, 6, and 12 months after the laser ablation procedure. The purpose of the ultrasonography examination was to examine the ablated vein for venous reflux and thrombus recanalization and to also exclude deep vein thrombosis. The success of the ablation procedure was defined as lack of compressibility of the treated vein segment, absence of blood flow inside the vein, decreased vein diameter, and the palpation of the fibrotic vein during examination. Complications such as ecchymosis, skin burn, paresthesia, induration, or complaints related to EVLA were evaluated and recorded for each case.
Patient satisfaction was assessed at the 6-month follow-up with a simple scale ranging from 0 to 4. The patient satisfaction assessment consisted of two simple questions: (1) Are you satisfied with the ablation procedure? (0: very satisfied, 1: satisfied, 2: slightly satisfied, 3: not satisfied, 4: extremely dissatisfied) and (2) would you choose this treatment again? (0: absolutely, 1: probably, 2: don't know, 3: probably not, 4: absolutely not). The patients' responses were recorded.
Assessment of pain
Following the treatment, all patients were informed and asked to complete a diary card for 7 days to record their level of pain. They were asked to use the Visual Analog Scale (VAS) (0 cm for no pain andPE 10 cm for the worst pain possible), which was provided at the time of discharge. At the first post-ablation follow-up, patients were questioned about whether they took the recommended analgesic drugs and if so, on which day they perceived the maximum amount of pain.
Collection and evaluation of the data
The patients' data were prospectively collected and recorded with Microsoft Excel. The total laser energy (Joules), power of the applied laser (watts) and other parameters were recorded for each case. The length of the treated venous segment was measured on the skin using a sterile ruler and was subsequently recorded.
The tumescent local anesthesia solution quantity (mL), which was injected with a Klein pump® (HK Surgical, Inc., San Juan Capistrano, CA) into the perivenous space, was recorded for each case.
Statistical analysis
Statistical analysis was performed with GraphPad Prism 5 (GraphPad Prism Software, La Jolla, CA) statistic software. Continuous variables are reported as the mean±standard deviation (SD). Correlations were performed using the Pearson χ2 test.
Results
The EVLA procedure was technically successful in all patients (N=98). Demographic characteristics, clinical characteristics and CEAP, classifications of all patients are listed in Table 1. A family history of varicose veins was present in 45 patients (43.68%).
The mean GSV diameter, measured in an upright position at 2 cm below the SFJ, was 6.12±1.37 mm. The mean length of GSV was 29.93±6.36 mm. Data related to the EVLA procedure are listed in Table 2.
Side effects were quite common in the early post-ablation period, including paresthesia, ecchymosis, and induration over the treated vein. Ecchymoses were possibly caused by laser ablation or needle punctures from the tumescent anesthesia solution administration. These were self-limiting during the first week following EVLA. No major complications, such as skin burns, deep vein thrombosis, or pulmonary embolism, occurred.
In the immediate post-ablation period, successful occlusion was noted at 95%. This initial success rate remained constant throughout the follow-up period, reaching 97% at 12 months. Occlusion and minor complication rates during the follow-up period are listed in Fig. 1.
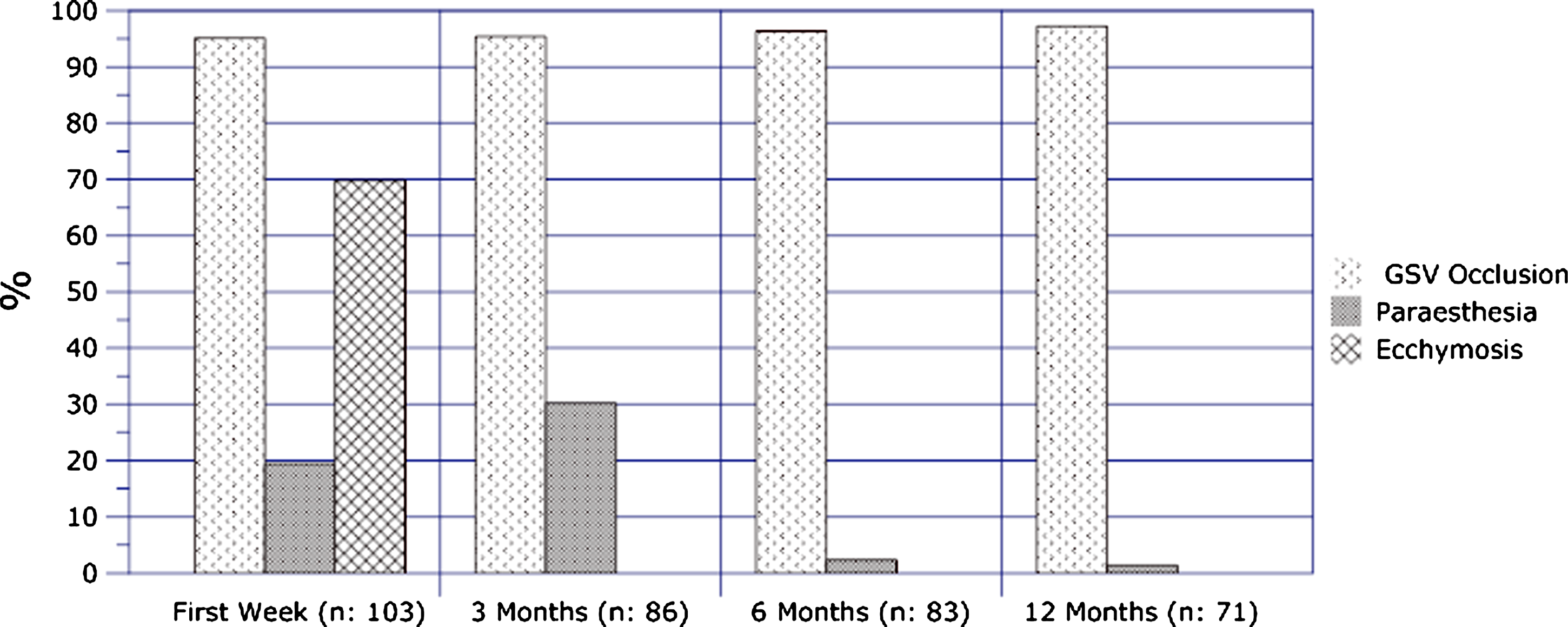
Occlusion and minor complication rates during follow-up periods.
The evaluation of pain scores recorded by patients during the first week post-EVLA is shown in Fig. 2. The majority of observed pain (N=98) was reported to have occurred between 1 and 5 days following the procedure. The mean VAS value for pain assessment was found to be 2.73±1.18 in the first week after the EVLA procedure.
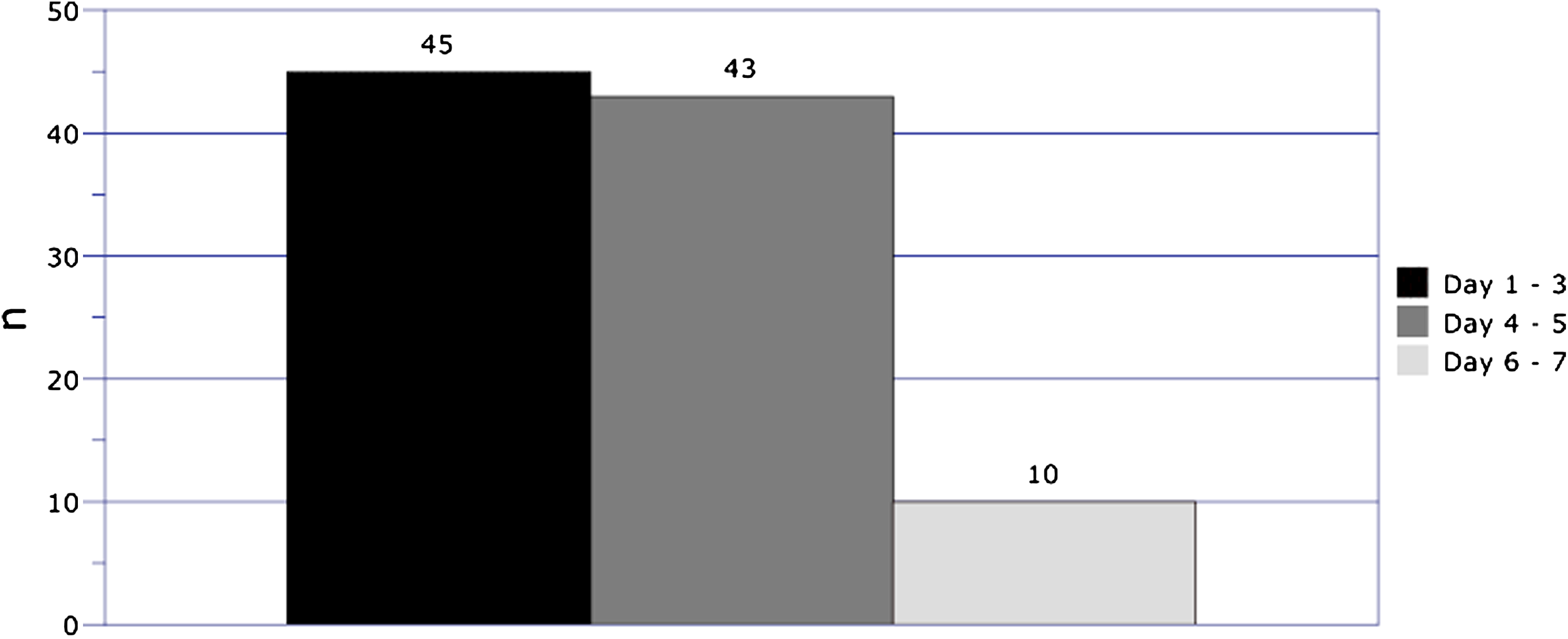
Observation of pain after EVLA during the 1-week follow-up.
The applied laser energy quantity (LEED) and observed pain scores after EVLA were evaluated. The Pearson correlation test was used to find the correlation, and the result of the analysis is shown in Fig. 3. No correlation was observed between the energy delivered per centimeter and the pain after EVLA (Pearson r value: 0.01632).

Pain after EVLA and its correlation with LEED.
The cases with recanalization identified in thrombus during the post-EVLA follow-up period are summarized at Table 3. One of the two patients who required recanalization at the 12-month follow-up was symptomatic, and this patient refused another operation and decided to be treated with conservative methods. The second patient who required recanalization and was asymptomatic had flow inside the thrombosed vein segment without insufficiency at the SFJ.
The procedural satisfaction was assessed at the 6-month follow-up evaluation. The results are shown in Figs. 4 and 5. Whereas 96.38% (n=80) of these cases reported that they were satisfied with the procedure, 3.6% (n=3) of the cases reported that they were not satisfied with the treatment. All patients who completed the satisfaction assessment had a successful EVLA procedure.
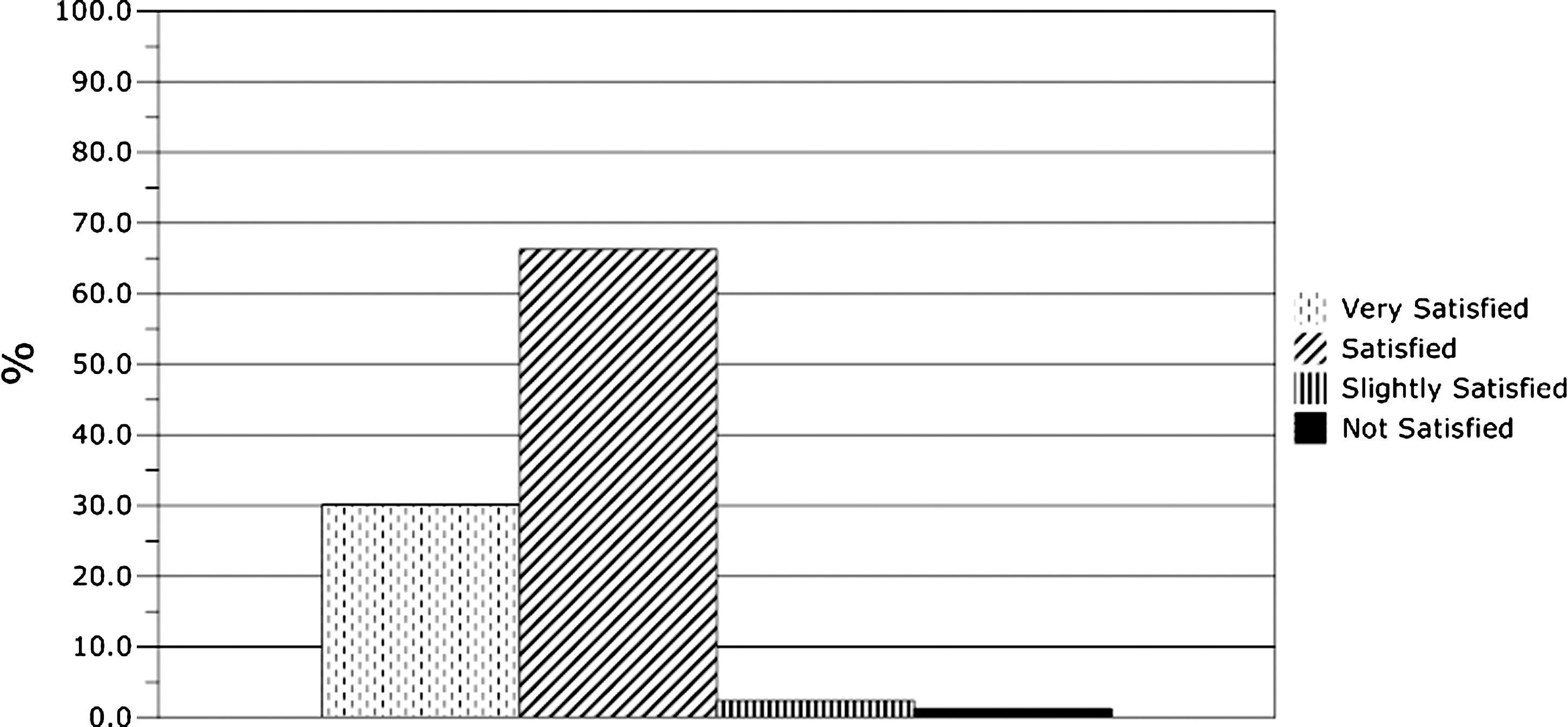
The patient satisfaction assessment after EVLA at 6 months, as determined by the question “Are you satisfied with the ablation procedure?”
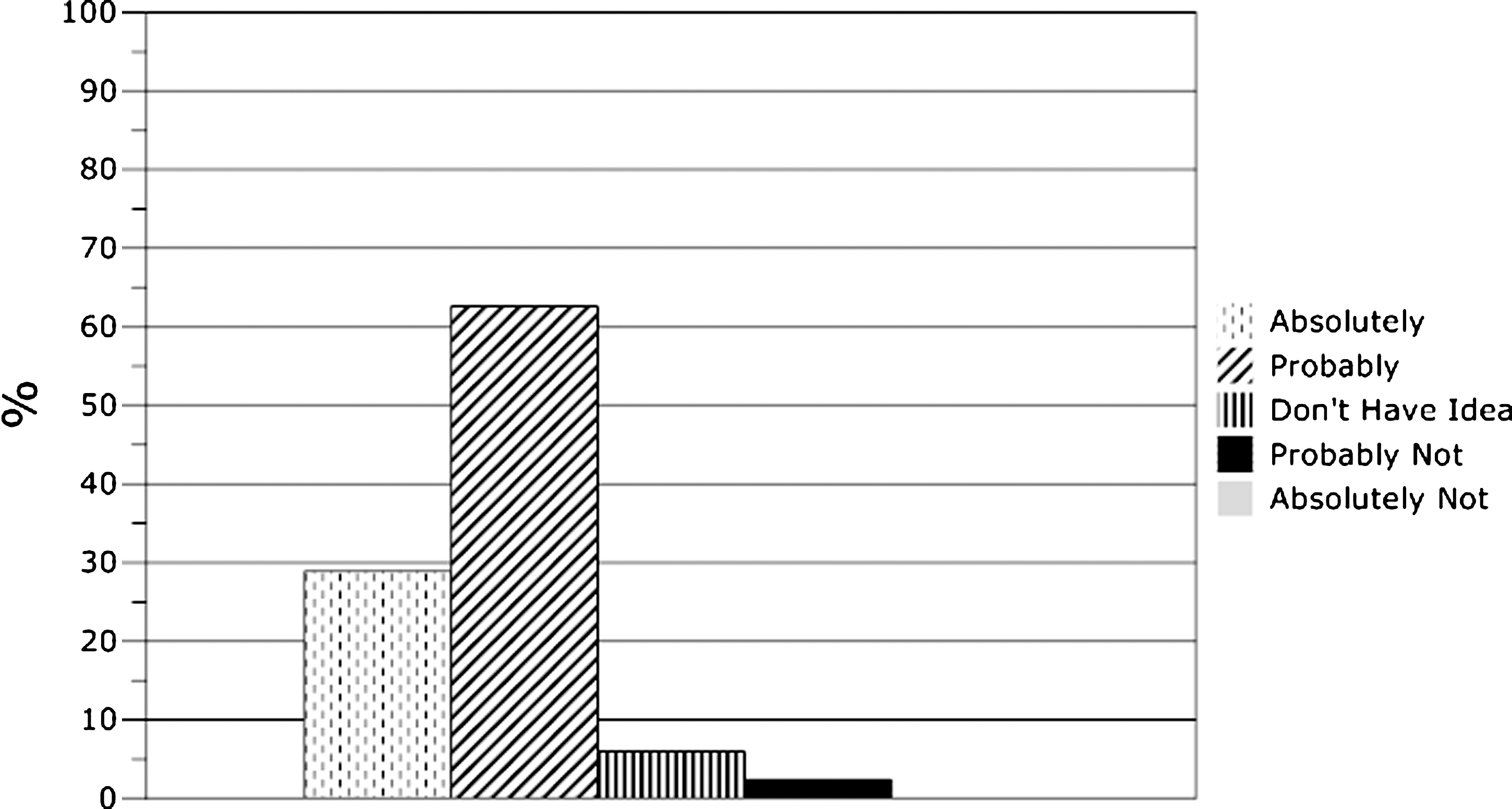
The patient satisfaction assessment after EVLA at 6 months, as determined by the question “Would you choose the EVLA treatment again?”
Discussion
Venous insufficiency of the GSV is the most common contributor to varicose veins. Although it does not directly cause mortality, it affects and impairs the patient's quality of life. 1 Historically, surgical treatments, such as high ligation or stripping of an incompetent GSV, have been used to treat varicose veins resulting from SFJ reflux. The surgical ligation, with or without stripping, is the classic and most recognized intervention for GSV varicosity. 9 This procedure is associated with an excellent early outcome because the incompetent vein is completely removed. However, 20–40% of the cases present with recurrence within 5 years because of neovascularization. 10 In addition to this important problem, the surgical stripping has a number of disadvantages, such as risk of deep vein thrombosis, requirement of longer hospitalization, prolonged return to daily activities, and unwanted postoperative scarring. 9
EVLA was introduced as an alternative method and rapidly became the treatment of choice for venous insufficiency of the GSV. 11 EVLA avoids stripping the incompetent vein and instead is based on the thermal ablation of the incompetent vein with laser energy via fiberoptic catheter. Several wavelengths have been proposed, respectively 810, 940, 980, 1064, 1320, 1470, 1500, and 1560 nm, with 810, 940, and 980 nm the most commonly used. Simply put, the laser energy causes initial damage to the incompetent vein by heating the collagen of the venous wall, which results in permanent occlusion followed by fibrosis. 12 The energy, main determinant of success, is administered endovenously in pulsed or continuous fashion. LEED, which was based on the measured GSV diameter near to SFJ, was used. For GSV diameters between 4.5 and 6.9 mm, and between 7 and 10 mm; 60–70 J/cm, and 80–90 J/cm of energy were used, respectively. 8
The efficacy of EVLA in obliterating the GSV has been reported to be >90%. 13 –16 However, EVLA's success may vary, because of the unique characteristics of treated varicose veins, and therefore, the occlusion degree may decrease to <90%. 17 Our study shows successful early occlusion and low recanalization rates, which support the literature remarkably well. 4 Reoperation attempt has not been required for the patients with recanalization during follow-up.
Although there are many studies on the effectiveness and reliability of EVLA, there is still no consensus on the optimal laser parameters, including the laser wavelength that is used to treat venous insufficiency, the laser energy type to be applied, the fluence time, and the energy quantity required. Proebstle et al. and Timperman et al. have advocated the use of higher energy for greater clinical responses. The ideal laser energy parameters for achieving permanent vein occlusion without unwanted thermal injury to adjacent structures are currently unknown. 18, 19 However, the standardization of these laser parameters was not the aim of this study.
The proper tumescent anesthetic technique is essential to ensure that the EVLA procedure is safe and less painful. Perivenous fascial space containing the tumescent anesthesia solution provides a margin of safety and prevents thermal injury to adjacent structures. 20 In our observation under ultrasonography assessment during the ablation procedure, the Klein peristaltic infiltration pump provided a more homogenous distribution of tumescent anesthesia solution than a manual 50-mL syringe system. The use of the Klein peristaltic infiltration pump may have contributed to the lack of skin burn or nerve damage in our patients.
The conventional treatment of GSV insufficiency by surgical ligation with or without stripping leads to appreciable trauma, cessation of activities, scarring, and, most importantly, a high rate of recurrence. Alternative techniques are gaining increased acceptance by patients. Our study confirms that patients with high satisfaction rates would choose the EVLA treatment again.
The most frequently observed situation at our follow-ups was pain over the treated vein segment. We hypothesized that the length of ablated vein segment would correlate with the amount of post-ablation pain. However, this was not supported by our results (Figure 6, Pearson r value: 0.02202).

Correlation of ablated vein segment and post-ablation pain during the 1-week follow-up.
The incidence of self-limiting minor complications, such as ecchymosis, pain, and paresthesia, was similar to the results of previously reported studies. 4, 12, 15, 21 Ecchymosis may be associated with various causes, such as multiple subcutaneous injections of the tumescent anesthetic solution, and needle and wire or introducer manipulation.
Major complications following EVLA are rarely observed in the literature and were similarly not seen in our study. 22 Incidence of deep vein thrombosis, which is one of the most significant complications in the literature, occurs in 0–5.7% of patients. 15, 23 –25 In our study, deep vein thrombosis was not observed. We believe this may be explained by our use of early ambulation to maintain deep vein and SFJ tributary flow and the use of the correct position for the fiberoptic catheter during the ablation, which prevented thrombi from extending into the deep venous system.
Hyperpigmentation after EVLA is a rarely observed complication. 22 In our study, we had one patient with hyperpigmentation that began 1 month after ablation. After dermatologic examination, topical treatment was started, and hyperpigmentation disappeared within 6 months.
In Turkey, the EVLA procedure is not on the refund list of the social security system and was not redeemable by the system. The total cost of the procedure is higher than the standard surgical ligation. However, cost analysis was not the aim of this study. Further studies on this issue and comparison with standard surgical techniques may be helpful.
The principal finding of this and other similar clinical studies is that EVLA with a 980-nm diode laser system, when performed under properly distributed tumescent anesthesia, is safe, clinically feasible, and well tolerated. 26 , 27 Limitations of this study include a modest number of study participants, a single laser wavelength, and no comparison. A larger study with randomization for treatment using different laser energies and wavelengths would help clarify the ideal or lowest energy threshold to use. This study only presents the midterm follow-up results of the patients; there are insufficient data on the long-term results. In addition, although our study used different laser energy quantities, it is not possible to make an interpretation on optimal laser parameters.
Conclusions
In conclusion, we consider EVLA with a 980-nm diode laser to be a safe and effective method that can be performed in an outpatient setting with good patient satisfaction and low complication rates.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.