
Abstract
Introduction
The microbial etiology of periodontitis has been extensively studied and it has been found that it is not associated with a single micro-organism, but rather is a consortium of bacteria that participate in the initiation and progression of the disease. In order for periodontopathic bacteria to cause periodontal diseases, it is essential that they are able to colonize subgingival pockets and produce virulence factors that directly or indirectly damage host tissue. 14,15 The major goal of periodontal therapy is to significantly reduce or eliminate oral microbial biofilms and periodontopathogens. 9,16 The appropriate therapy for patients with periodontitis includes procedures such as scaling and root planing (SRP); however, the optimal therapy varies considerably with the extent and pattern of attachment loss, local anatomical variations, type of periodontal disease, and therapeutic objective of the treatment. The goal of periodontal therapy is to halt disease progression and stabilize periodontal attachment levels. The use of systemic antibiotics as additional support for periodontal treatment regimens is necessary at times. However, systemic antimicrobial drugs may be associated with adverse reactions, such as nausea/vomiting, hypersensitivity, photosensitivity, and diarrhea. 17 In addition, the production of drug-resistant organisms following antibiotic therapy has been observed, 18 and it is well known that the overuse of antibiotics is a major factor in the production of drug-resistant periodontal organisms. 19
Antimicrobial strategies that act in combination with mechanical periodontal therapy (MPT) may markedly improve the outcome of periodontal treatment. Some subgingival irrigating agents, such as 10% povidone-iodine, 0.1% sodium hypochlorite, and 0.12–2% chlorhexidine, can be useful adjuncts for MPT. 20 More recently, photodynamic PDT has been used as a new treatment approach for localized infectious diseases, including periodontitis. 1 –8 PDT consists of the combination of a PS and a resonant light source to produce localized photo damage and subsequent cell death. The mechanism of action is based on the interplay of PS, light, and oxygen. 9 –13 The initiating step is the absorption of a photon by the PS, which goes from a stable ground state to an unstable excited singlet state with an extremely short life span. The excited singlet compound may decay back to its ground state and thereby emit light fluorescence, or it can transform into the longer-lived triplet excited state. In a triplet state, the drug readily interacts with surrounding molecules and oxygen, causing the formation of peroxides, superoxide ions, hydroxyl radicals, and singlet oxygen. The presence of singlet oxygen is believed to play a key role in photodynamic microbial cytotoxicity, as the high reactivity produces an oxidizing interaction in biological tissue.
Despite tremendous progress in the use of PDT for periodontal disease in recent years, very few studies to date have described the role of this therapy in the killing of bacterial cells and periodontium recovery. Therefore, we used a histomorphometric and microbiological assessment to evaluate the corroborative effects provided by PDT in periodontal tissue in rats. Cytotoxic effects, collagen organization, and inflammatory factors were evaluated in the host tissue. In addition, the use of rodents to investigate host–bacteria interactions related to periodontal disease is useful as a reproducible model of a standard response. A rat ligature model and rat Aggregatibacter actinomycetemcomitans feeding model have been reported. 21 In the rat A. actinomycetemcomitans feeding model, periodontal disease is observed after 84 days. To increase the challenge and reduce this time period, we developed a rat periodontal disease-induced model in this study using a ligature imbibed in an A. actinomycetemcomitans suspension in order to investigate colonization and general microbial reduction. To confirm the presence of this bacterium in our model, polymerase chain reaction (PCR) was performed.
Methods
This study was conducted in two different phases: (1) investigation of the histomorphometrical changes provided by PDT in periodontal tissue, and (2) analysis of the microbiological reduction provided by the therapy. The experiments were approved by the Ethical Committee for Animal Research of IPEN-CNEN/SP. All rats were housed under the same conditions and maintained on food and water ad libitum.
Histomorphometrical analysis
Ligature induction of experimental periodontitis
Thirty healthy male Wistar rats (Rattus norvegicus) with a body mass of ∼250 g were used for histomorphometrical analysis. The rats were anesthetized with ketamine (80 mg/kg) and xylazine (10 mg/kg) by intraperitoneal injection. A cotton ligature was placed around the upper left second molar in a submarginal position to induce periodontal inflammation 22 (n=27). A control group without periodontitis induction (n=3) was housed and maintained under the same conditions as the experimental animals. Seven days after the cotton ligature was inserted around the teeth, it was removed from the animals and they were randomly divided into three groups. The positive control group (n=3) was immediately euthanized without treatment. One group received scaling and root planing (SRP group; n=12) and were irrigated with 100 μL of distillated water. The other group (SRP+PDT group; n=12) received SRP as treatment and PDT as subsequent adjuvant therapy.
The experimental schedule is illustrated in Fig. 1, which shows the induction of periodontitis on day −7. All treatments were performed on day 1. The animals were euthanized in a CO2 chamber at 8 h, 24 h, 72 h, and 7 days post-induction, and the maxilla was removed from each animal for analysis (n=3 animals per group).

Induction of periodontitis on day −7. After 7 days, all treatments were performed. The animals were euthanized after 8 h, 24 h, 48 h, and 7 days.
PDT
One hundred microliters of methylene blue (MB) (Sigma Ltd, Poole, UK) in a water solution was used as a PS at a final concentration of 100 μM under dark conditions. 10 The PS was applied around the upper second molar and a pre-irradiation time of 5 min was set. The tested area received the laser irradiation through the palatal side. PDT was performed with a diode laser (QUANTUN, Ecco Fibras, Campinas, Brazil), which emitted a wavelength (λ) of 660 nm and output power of 100 mW. An energy of 6 J was applied punctually in an area of 0.8 cm2, during 1 min of irradiation, which delivered a fluence of 7.5 J/cm2.
Histological procedure and evaluation
The maxilla of the treated and control rats was removed and the samples were immediately fixed in 4% paraformaldehyde. The maxillas were placed in small glasses and identified according the respective groups. The specimens were then submitted for histological processing and the fragments were stained using hematoxylin & eosin (H&E).
Collagen organization was evaluated by visual scoring (1 to 4) and three slides of each rat were evaluated by Motic microscopy, with a score of 1 being the worst, representing 25% of collagen organization; a score of 2 representing 25–50%; a score of 3 representing 50–75% of organization; and a score of 4 being the best, representing 100% of collagen fibers organization. Concurrently, the inflammatory infiltrate was analyzed according to the cell type and classified as acute or chronic; and according to the density of leucocytes and scored from 1 to 4, with a score a 1 representing the least infiltrate and 4 representing the most infiltrate. 8
Bone loss was evaluated using Motic Images software (National Optical & Scientific Instruments, San Antonio, TX). The analysis was made by measuring the distance of the coronal margin of the bone crest to the enamel-cementum limit. Each sample was evaluated and a percentage value of the amount of bone loss was calculated. The frequency of group scores was statistically compared by the Wilcoxon matched test and bone loss was compared by the Student's t-test. Samples were considered statistically significant if p<0.05.
Microbiological analysis
Twenty, 12-week-old specific pathogen-free adult male Wistar rats with a body mass of ∼250 g were selected for this phase of the study. The animals were maintained in individual cages with a regimen of 12/12 h day/night light cycle and received food and water ad libitum. To suppress the host resident microbial flora before disease induction, the animals were subjected to systemic antibiotic therapy for 5 days and received a daily dose of 1 mL ampicillin at a concentration of 50 mg/mL in their water.
The induction of periodontal disease was initiated after 2 days of systemic antibiotic therapy. For this purpose, the animals were anesthetized with an intraperitoneal injection containing xylazine (10 mg/kg) and ketamine (80 mg/kg). The induction was accomplished by subgingival placement of a cotton ligature around both maxillary second molars that had been submerged in a culture of A. actinomycetemcomitans.
Periodontal infection induction and bacterial quantification
A clinical isolate of an adherent wild-type A. actinomycetemcomitans strain was collected from a Brazilian patient with aggressive periodontitis. 23 Catalase and morphologic Gram stain tests were used to establish the presumptive species identification. 1,23 PCR was used to qualitatively identify the species.
A. actinomycetemcomitans was subcultured in tryptic soy agar (TSA) containing 6 g/L yeast extract and incubated under microaerophilic conditions at 37°C for 48 h. Bacteria colonies were harvested from the TSA and the strains were suspended in phosphate buffered saline (PBS) in an optical density No. 4 McFarland standard solution (∼1.2×109 cfu/mL). The cotton ligature was submerged in 1 mL of bacteria suspension, placed around the teeth, and then maintained in position for 15 days (Fig. 2). Clinical observation during this time period confirmed the presence of inflammation. The animals were then randomly divided into the following two groups: mechanical periodontal therapy (MPT) alone (n=10), and MPT with PDT (MPT+PDT) (n=10).
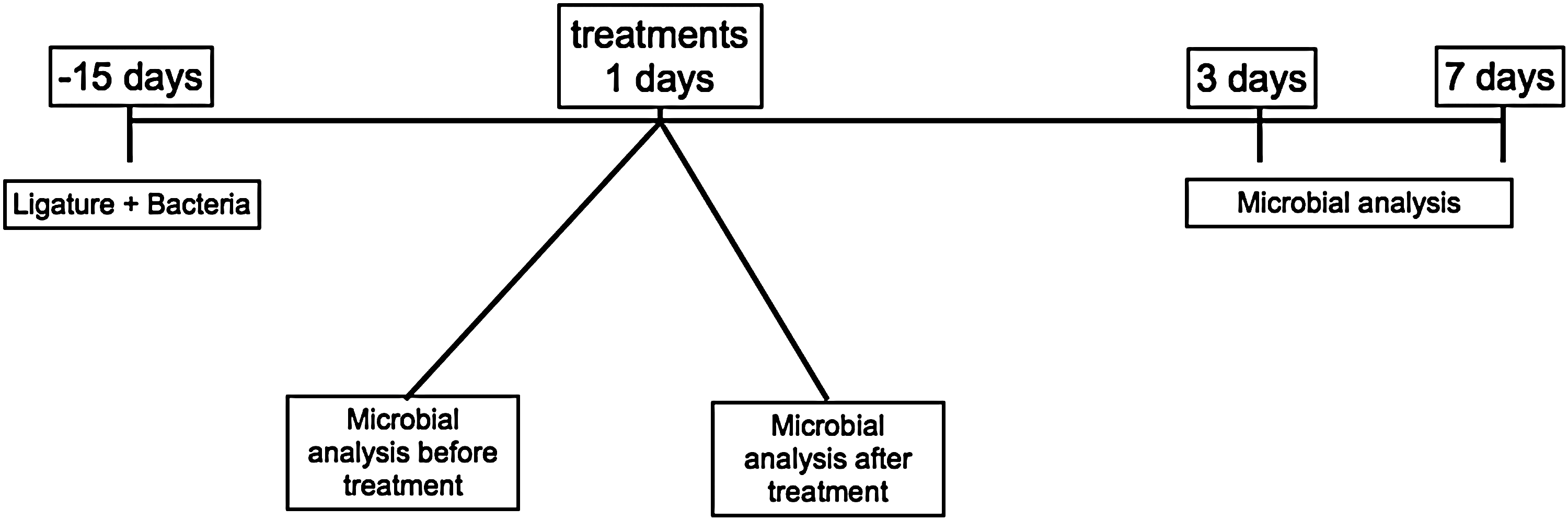
Induction of periodontitis on day −15. After 15 days, all treatments were performed and microbiological analyses were subsequently performed.
Mechanical periodontal therapy replaced SRP because of the bleeding and trauma caused by SRP in the rat gingival tissue. A previous pilot study demonstrated a poor recovery of periodontal bacterial species from sites that had been subjected to SRP in the rats, which could have affected the microbiological measurements immediately after the treatment (data not shown).
As no mineralized deposits were observed on the experimental teeth, the MPT was adopted in this model and was performed using a toothbrush with slow vibration movements for 20 sec in both groups. One hundred microliters of saline solution was applied into and around the periodontal pockets following the MPT procedure.
MB (300 μM; Sigma Aldrich, USA) was used as a PS, and 100 μL of this solution was topically applied into and around the periodontal pockets after MPT and maintained for 5 min without illumination. A red low-power laser (QUANTUN, Ecco Fibras, Campinas, Brazil) was subsequently used to punctually irradiate the periodontal pockets for 60 sec (λ=660 nm; P=100 mW; and E=6 J).
Microbiological samples were collected using sterile No.15 point paper, which was placed inside the periodontal pockets for 60 sec before and immediately after treatment. Thereafter, the points were placed into a 3 mL vial containing Viability Medium Götenborg Anaerobically (VGMA) III transport medium. All samples were collected by the same operator, coded by an assistant to mask identification, and processed in <3 h.
Semi-solid VMGA III medium was incubated at 37°C for 15 min before being agitated by vortex for 60 sec. The samples were then serially diluted in peptonated water to provide dilutions of 10−1–10−5 times the original concentration. Aliquots of 100 μL of the dilutions were placed in Petri plates containing tryptic soy-serum-bacitracin-vancomycin (TSBV) agar, 24 and then incubated in microaerophilic jars with a 5–10% CO2 atmosphere at 37°C for 48 h. Additional 100 μL aliquots were plated on 5% sheep blood brucella agar plates and incubated in an anaerobic chamber for 48 h at 37°C. 18
Qualitative analysis PCR
Samples from vial stock plates were qualitatively analyzed by PCR to confirm that the bacterium species was the A. actinomycetemcomitans species prior to periodontal inflammation induction. The same test was also performed on colonies recovered before treatment in order to confirm the presence of A. actinomycetemcomitans in the induced periodontal infection, and following the treatment regimens (MPT and MPT+PDT). For this purpose, three colonies were removed from each plaque and inserted into a 0.1 mL TE solution (10 mM Tris-Cl, pH 7.5; 1 mM EDTA, pH 8.0). DNA extraction was performed according to Dewhirst et al. 25 Oligonucleotide species-specific primers were designed with the following sequences: 5′-GTT TAG CCC TGG TGC CCG AAG-3′ (forward primer) and 5′-TGA CGG GCG GTG TGT ACA AGG-3′ (reverse primer) (Invitrogen, Brazil). Negative and positive controls were included with each batch of sample analysis. The positive control was composed of genomic DNA extract from A. actinomycetemcomitans (HK 1651) and the negative control contained sterile, ultrapure water. Aliquots of 5 μL of the clinical template or 1 μL of the reference DNA were amplified. PCR amplification was performed in a 25 μL reaction mixture containing 25 nmol of each specific primer, 2.5 μL of 10×PCR buffer, 0.75μL of 1.25 mM MgCl2, 2.5 U of Taq DNA polymerase (Invitrogen, Brazil), and 5 mM of each deoxynucleoside triphosphate.
The PCR amplification was performed in a DNA thermocycler (MJ Research, Minnesota, MN). Cycling parameters included an initial denaturation step at 95°C for 5 min followed by 25 cycles of 95°C for 30 sec, a primer annealing step at 55°C for 30 sec, and an extension step at 72°C for 45 sec. A final cycle at 72°C for 5 min concluded the reaction. The results of the PCR amplification were examined by electrophoresis in a 1.5% agarose gel (Sigma Chemical C., St. Louis, MO). DNA was stained with ethidium bromide and visualized under short wavelength UV light. A 100 bp DNA ladder was used as a molecular size standard. Samples were considered positive for A. actinomycetemcomitans when a single band was visualized at 547 bp.
Statistical analysis
To assess the effect of the treatments on bacterial killing, bacterial colonies were counted and converted to colony form units for analysis. A Student's t-test was used and p<0.05 was considered a statistically significant difference.
Results
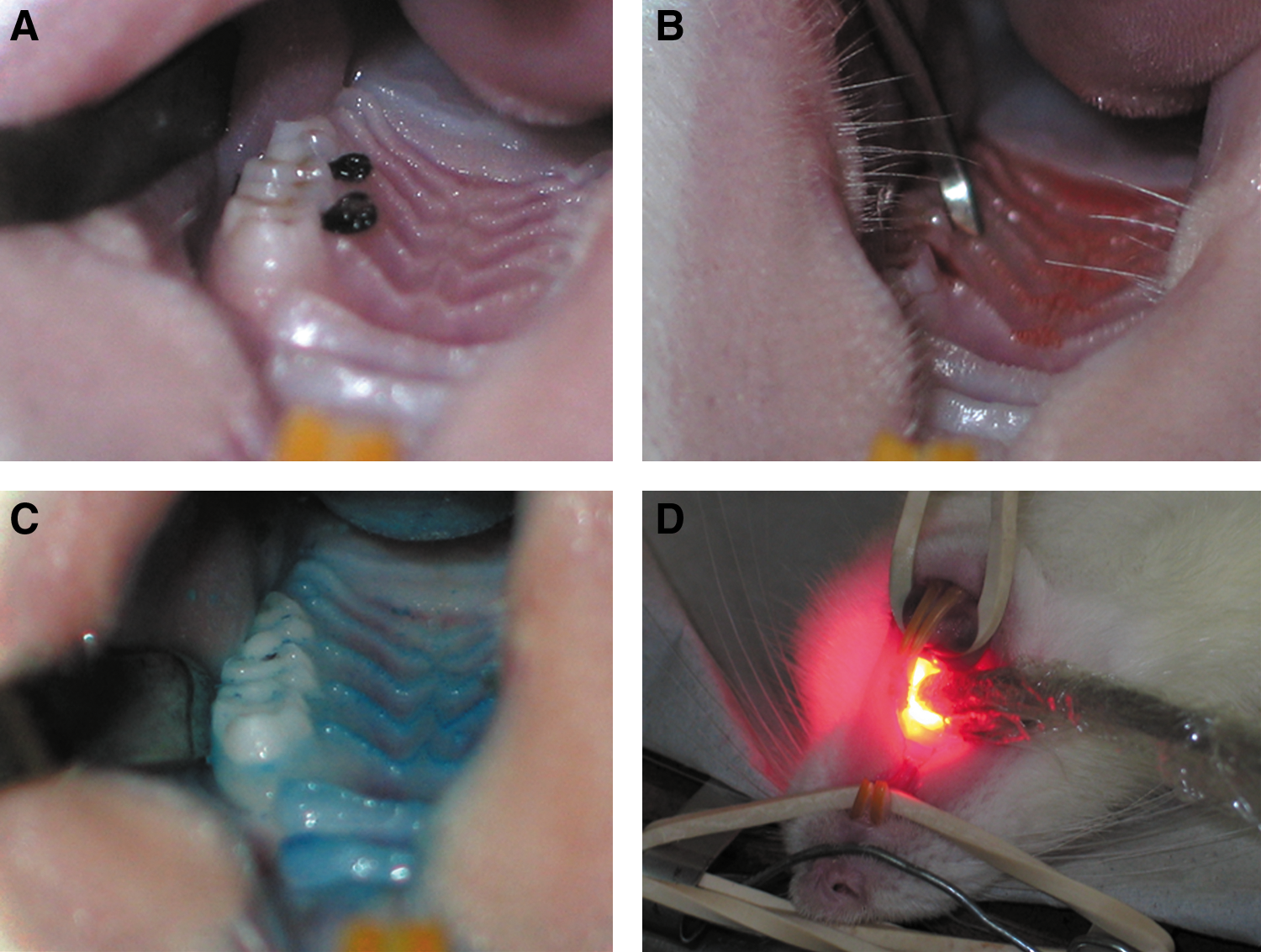
Clinical signs of periodontal disease were observed 7 and 15 days post-induction for both portions of the study. All animals showed inflammatory signs, such as redness, edema, and gingival bleeding upon probing. No mineralized deposits were observed on the experimental sites, and a mature biofilm was observed on the tooth surface (Fig. 3). During the entire experimental period, the rats gained body mass and did not show any signs of complication.
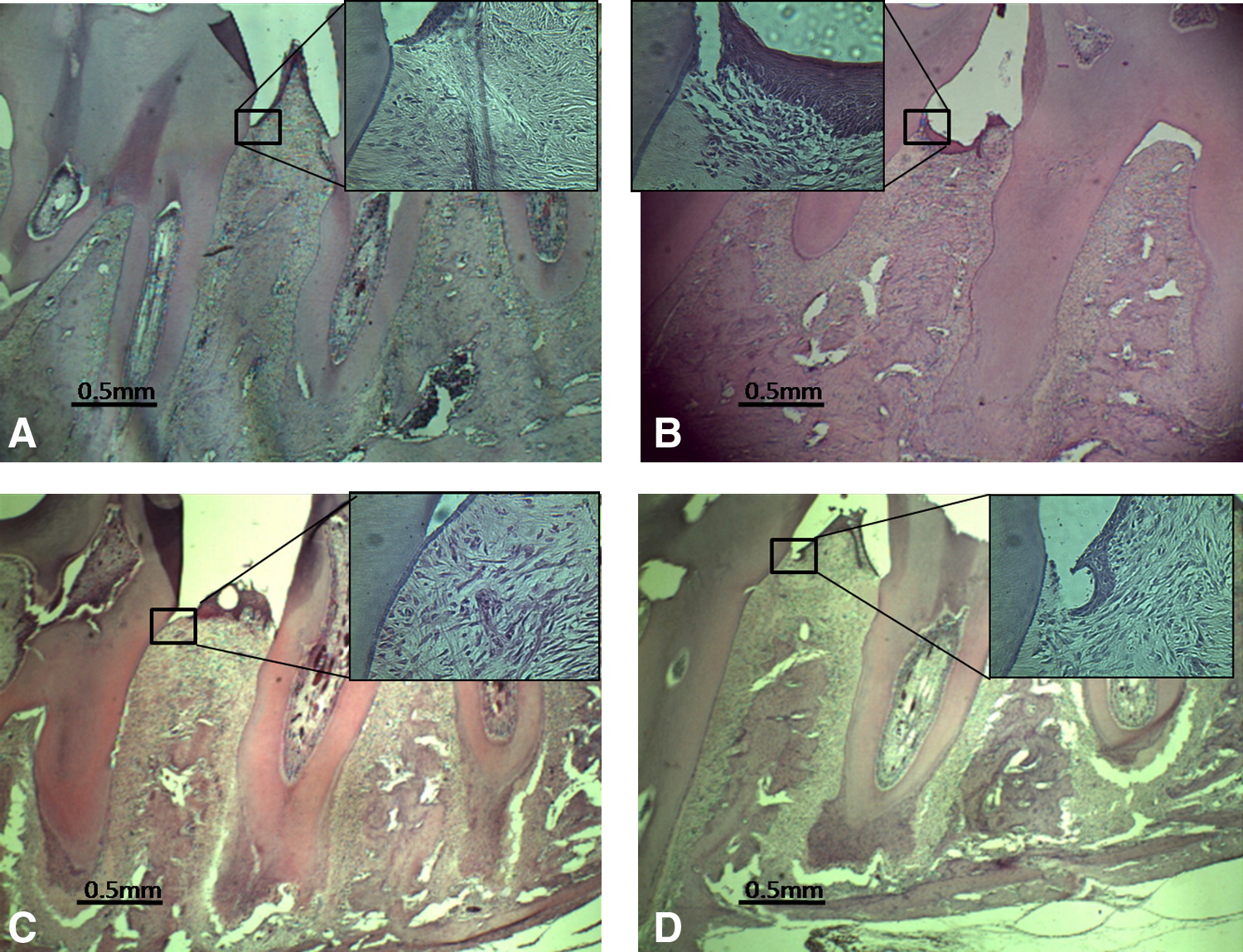
The histological evaluation of the periodontal inflammatory infiltrate showed that all specimens developed a nonspecific chronic inflammation, characterized by the presence of plasma cells and lymphocytes. Evaluation of the collagen fibers on the slides showed an improvement in organization for both groups (Fig. 4 and Table 1).
Statistically significant difference between groups (p<0.05; Wilcoxon matched test).
n=total number of slides evaluated.
SRP, scaling and root planing; PDT, photodynamic therapy.
Eight hours after treatment, the collagen fibers of the group that received SRP+PDT were significantly (p<0.05) more organized than the group that received SRP treatment alone. In addition, the number of inflammatory cells in the SRP group was significantly higher (p<0.05) than in the SRP+PDT group 8 h after treatment (Table 2).
Statistically significant differences between groups (p<0.05; Wilcoxon matched test).
n=total number of slides evaluated.
SRP, scaling and root planing; PDT, photodynamic therapy.
The crest bone evaluation refers to the percent change in bone level for the two groups of this study. The control group represents the percentage of bone loss on the treatment day. Differences between the groups were not observed at 8, 24, or 48 h after treatment (p>0.05). Interestingly, after 7 days, the SRP+PDT group showed a significant gain (p<0.05) in bone level compared to the control and SRP groups (Fig. 5). In contrast, the SRP group exhibited a significantly greater loss (p<0.05) in bone level 7 days after the treatment compared to the control group (Fig. 5).
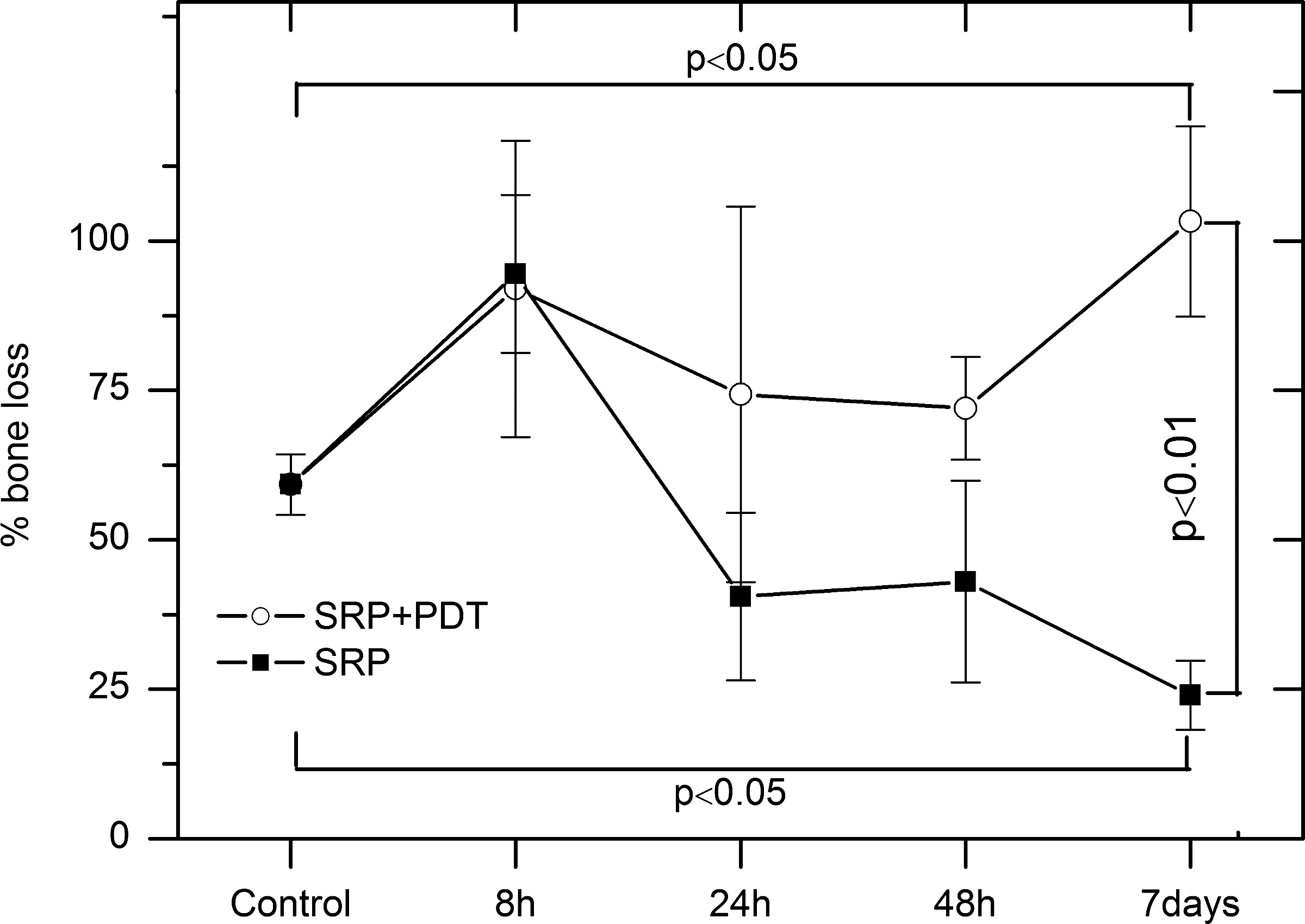
The data are means of bone loss and standard deviation. The Y axis represents the percentage of bone loss of the two groups evaluated in this study. The control shows the bone level after periodontitis induction and before treatment. Differences between the groups were not observed at 8, 24, and 48 h after treatment. After 7 days, the SRP+PDT group presented a statistically significant gain in bone level compared to the control and SRP groups (p<0.05). The SPR group showed additional bone loss compared to the control group.
Figure 4A shows a healthy example of periodontal tissue with few inflammatory cells and well organized connective tissue. However, in rats with ligated periodontal tissue, we observed a loss of interproximal architecture and periodontium destruction before treatment (Fig. 4B). As shown in Fig. 4C, a reorganization of the tissue architecture was observed in the SRP group 48 h after treatment. However, the SRP+PDT group displayed a higher tissue organization and more protuberant interdental papilla at the same time point than did the group receiving SRP treatment alone (Figs. 4C and D).
Qualitative analysis by PCR
PCR amplification of reference genomic DNA of the target species (positive control) with the respective taxon-specific primers resulted in a single band of the predicted size (547 bp). Clinical samples that were positive for A. actinomycetemcomitans also had only one band of the predicted size. Figure 6 shows a representative gel of the specific amplicons for the reference DNA and clinical samples of A. actinomycetemcomitans. The A. actinomycetemcomitans species was detected in all samples collected from colonies in each positive culture before and after treatment. These results validated our model and showed that the bacterium was present and detected in all samples analyzed.

Representative amplicons of A. actinomycetemcomitans reference DNA (left) and clinical samples (right). PCR generated amplicons in the electrophoresis gel (1.5%). DNA from A. actinomycetemcomitans HK 1651 strain as positive control (+) and clinical samples (lane 1, before treatment; lane 2, after treatment) are characterized by a specific amplicon of 547 bp.
Quantitative analysis of bacteria
The described methodology was sufficient to induce a reproducible A. actinomycetemcomitans periodontal disease model. This bacterium was recovered from all samples. Figure 7 shows the bacterial viability of microaerophile and anaerobic micro-organisms before and after treatment. Prior to treatment, the microaerophile samples exhibited 3.1×104 CFU/mL and 2.4×104 CFU/mL for the MPT and MPT+PDT groups, respectively.
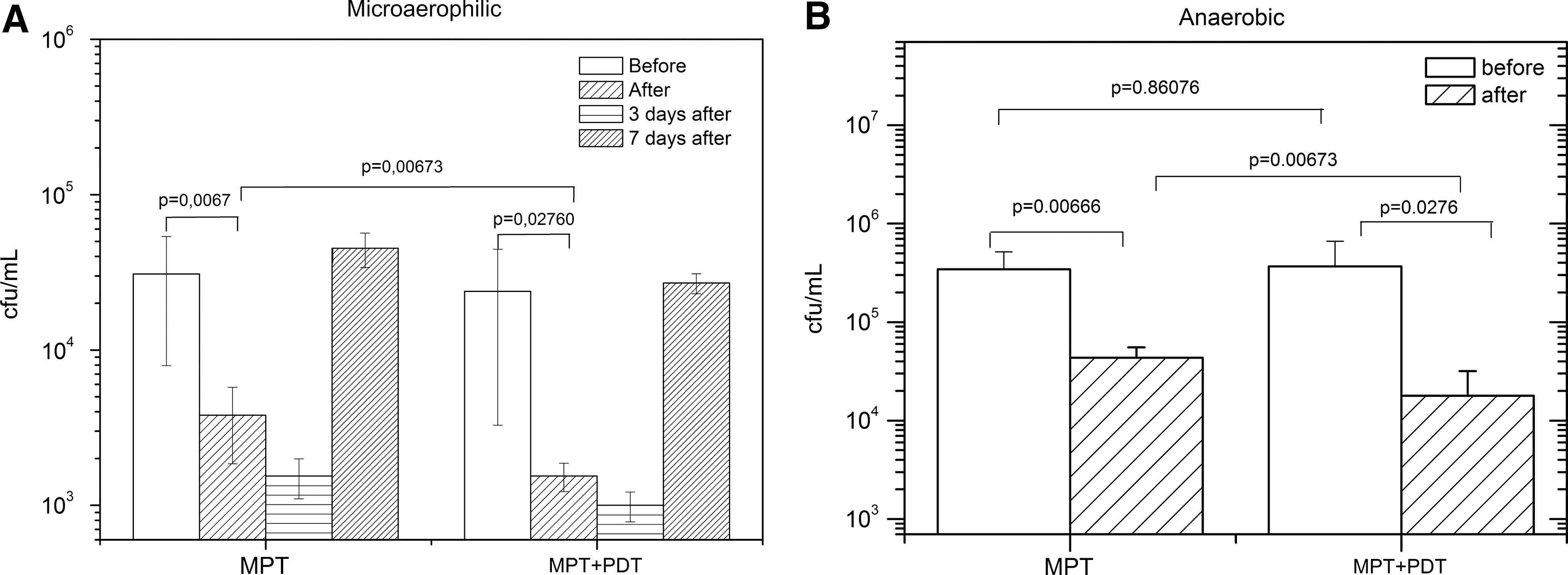
The mean recovery of
Our experiments demonstrated that both treatments significantly reduced microaerophylic bacteria viability. A reduction of 87.7% was achieved in the MPT group, whereas a significantly higher diminution was observed (93.5%) when MBwas used in conjunction with red light as an adjuvant to MPT. Supporting PDT resulted in a reduction of 1.2 log10 compared to 0.9 log10 obtained with MPT alone (Fig. 7A).
On the 3rd day following treatment, the bacterial viability was significantly lower (p<0.05) for both groups compared to the previous day. However, both groups still exhibited a small bacterial population. A mean of 1.5×103 CFU/mL (3.2 log10 units) was recovered from the MPT group, whereas the MPT+PDT group showed a mean of 1.0×103 CFU/mL (3 log10 units) of bacterial cells. No significant reduction was achieved between these experimental groups (Fig. 7A). At day 7, no statistically significant differences were observed between the groups. Interestingly, the viability of the bacterial population increased to the level observed at the beginning of the experiment, suggesting that bacterial recolonization or regrowth had occurred (Fig. 7A).
Regarding anaerobics, a statistically significant (p<0.05) decrease in viability was observed in the MPT+PDT anaerobe group compared to the MPT anaerobe group (1.32 log10 vs. 0.9 log10, respectively) (Fig. 7B). In addition, anaerobe bacteria recovery on days 3 and 7 showed similar results to microaerophylics (data not shown).
Discussion
During the last few years, several attempts have been made to introduce the concepts of PDT to the field of dentistry. Research groups have confirmed that laser radiation can have lethal effects on micro-organisms associated with dental caries, periodontitis, and peri-implantitis. 26,27 In fact, the application of an alternative method to eradicate bacteria from periodontal pockets is extremely advantageous. In the model presented in this study, PDT significantly reduced A. actinomycetemcomitans as well as anaerobic micro-organisms compared to mechanical removal of the biofilm alone. However, it can by questioned if a decrease of ∼6% of microaerophils and 8% of anaerobes is clinically significant. In this regard, it is important to note that the treatment of periodontal disease does not aim to eliminate all bacteria in the oral cavity. The best therapy option for treating periodontal disease is to guide the composition of the microbiota to one that leads to sustained freedom from the effects of oral infections. 15 In fact, our histomorphometric analysis showed a notable difference between the two experimental groups regarding periodontal disease after PDT up to 7 days post-treatment. The periodontal regeneration was improved by this technique when it was used as an adjuvant to the conventional periodontal therapy. The results of this study showed that rats receiving PDT after SRP had a better repair of the periodontal tissue, which can be attributed to the additional antimicrobial effect induced by PDT. Another hypothesis to explain the enhanced effect of SRP+PDT treatment is to assume that low-level laser therapy (LLLT) could stimulate the periodontal tissue and improve the regeneration in periodontal areas. In fact, de Almeida et al. have shown that LLLT may cause a minor bone loss in nondiabetic rats compared to SRP. However, they also demonstrated that PDT on periodontal tissue has a better effect when it is compared to LLLT. 28
The use of PDT on the tissues in this study was found to be safe, as a loss of connective tissue and necrosis were not observed. Our results confirm the findings obtained by de Almeida et al. 8 and Luan et al., 29 which demonstrated the safety of PDT on host tissues. Therefore, PDT was an effective and safe adjuvant for the inactivation of A. actinomycetemcomitans in a rat model of induced periodontal disease. The experimental design proposed in this study appears to be suitable for this purpose, and the data confirmed the presence of the micro-organisms 15 days after induction. However, further clinical evaluation will be necessary to confirm these findings and to focus on the application of antimicrobial PDT as a technique for the periodontal clinic. This study suggests that the combination of PDT with mechanical periodontal treatment induced a moderate reduction of A. actinomycetemcomitans and anaerobic viability.
Periodontal techniques can benefit from the combination of mechanical periodontal therapy and PDT. There are several advantages of PDT over conventional antibiotic therapy. First, PDT is a topical treatment, which only affects the sites that require antimicrobial-specific treatment. Therefore, unlike antibiotics, PDT would not disrupt the normal microflora of unaffected sites. Second, there is no evidence to date of the development of antimicrobial resistance to PDT. Therefore, this technique may be helpful in patients who possess multi-drug-resistant bacteria at periodontal sites. 30 Moreover, patients with leukemia who do not show a response to conventional treatments 31 may benefit from PDT, which is a technique that can affect oral micro-organisms without inducing oral trauma.
Black-pigmented anaerobe periodontopathogens, such as Porphyromonas gingivalis and Prevotella intermedia, are very susceptible to PDT, as they require iron for growth and contain the endogenous PS protoporphyrin for the sequestration of this metal. 32 In addition, A. actinomycetemcomitans can be 99.9% inactivated using 0.01% w/v MB for 5 min before irradiation with an energy of 5.4 J from a 660-nm laser. 33 In addition, Tannerella forsythia (formerly Bacteroides forsythus) and A. actinomycetemcomitans are less predisposed to PDT effects. 34,35 Nevertheless, these findings may not be true in vivo. It has been established that the presence of organic materials (e.g., blood or nutrient broth) as well as saliva and serum offer some protection to bacteria against lethal photosensitization. 36 In this study, a complete eradication of A. actinomycetemcomitans was not obtained after PDT. Many factors may interfere with the effectiveness of PDT, such as PS–micro-organism interactions, light distribution on the target area, laser parameters, and the presence of an extracellular matrix.
Some studies have reported that PDT can kill A. actinomycetemcomitans in vitro using a range of PS and light sources. 1,33,35 It was shown that ∼95% of A. actinomycetemcomitans could be eliminated, depending upon the PS concentration and light wavelength. In this study, we showed that it is possible to decrease A. actinomycetemcomitans and anaerobic micro-organisms in an induced periodontal disease model by using topically applied MB and red light after SRP or MPT.
There are conflicting results in the literature regarding the effects of PDT on periodontal disease. 3,8,29,37 A randomized, controlled clinical trial showed no additional reduction in pocket depths, bleeding on probing, or eradication of bacteria when a single cycle of PDT was combined with ultrasonic periodontal treatment. 37 In contrast, the effects of PDT on periodontal micro-organisms demonstrated high-quality prevention of periodontal progression in rats. 38 In addition, PDT was shown to be an effective auxiliary periodontal treatment in immunosuppressed rats. 3 Furthermore, PDT reduced probing pocket depths when used as an adjuvant to periodontal patient maintenance following a 6- month evaluation.
It is clear that the selection of an effective PS is essential for the success of PDT. MB, which belongs to the phenothiazinium family, is a well-known PS. Some studies have demonstrated the effect of PDT with MB against oral pathogenic bacteria. 39 MB shows strong absorption at 660 nm, and the best irradiation of this dye is in the resonant wavelength band with a maximum absorbance at λ=660 nm. 40 In contrast, the PS tolouidine blue, which is another dye from the phenothiazinium family, has a maximum absorption at 630 nm. Quin et al. showed that the best wavelength to irradiate this PS was 635 nm. 22 Therefore, the bactericidal effects are improved when the absorption band of the PS is resonant with the emitted radiation. 40 Unfortunately, the choice of a viable PS is not the only factor for optimal photodynamic effects. It is well known that optical characteristics of the tissues must be observed before irradiation. The tissues provide the extinction of light in an exponential process, which is directly related to the distance that that light propagates through. The light absorbed and scattered by the tissue may strongly affect the net amount of useful irradiation and significantly decrease microbial killing. It has been well established that successful PDT includes the optimization of the PS (type and concentration), parameters of irradiation (wavelength and light power), protocol of phototherapy (exposure time and delivered energy), and type of micro-organism. 10 Because PDT can kill micro-organisms in biofilms 26,41 and planktonic bacteria, 1,42 the microbiological evidence in this study shows that it may be useful as an adjuvant to SRP. However, additional animal studies are required to establish effective protocols for the use of PDT in clinical trials. 43 Additional research into the use of antimicrobial PDT in periodontitis is required for a greater understanding of this therapy, and additional clinical trials are encouraged to introduce PDT as a clinical procedure. 8,22,38
Conclusions
This study demonstrated that PDT presents a moderate but significant killing of anaerobic and microaerophylic bacteria under the parameters used. In addition, a short-term observation of the treated tissue showed a significant improvement in gingival healing following PDT.
Footnotes
Acknowledgments
Renato A. Prates is supported by a scholarship from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (Grant no. 500409/2010-2). This work was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP grant no. 05/01756-5). The authors kindly thank Silvia Cristina Núñez for her professional reading of the manuscript and Priscila F. Chaves for technical support in the laboratory.
Author Disclosure Statement
No conflicting financial interests exist.