
Abstract
Introduction
Endodontic failures are associated with gram-positive aerobic and facultative microorganisms. Several studies have shown Enterococcus faecalis resistance to antimicrobial agents such as sodium hypochlorite, 2 chlorhexidine, 2,3 calcium hydroxide, 4 and several antibiotics. 5 In addition, these species of bacterium are able to form biofilms in the root canal, 4 allowing their survival in harsh environments. 6
Techniques, instruments, and equipments have been developed to improve clinical work and achieve a high treatment success rate. In this context, high-power lasers have been shown to decrease the endodontic microbiota. 7,8 This decrease in the microbiota load is attributed to the high energy released through an intracanal optical fiber, destroying the microorganisms caused by an increase in temperature. 9,10 High-power lasers, however, have the potential to cause thermal injury to tissues, including carbonization of the dentin, root ankylosis, cementum melting, root resorption, and periradicular necrosis. For this reason, it is important that correct laser parameters are used to prevent damage to the attachment tissues. 11 High-power lasers seem to be very promising; nevertheless, the cost of such equipment still limits their application.
In recent years, photodynamic therapy (PDT) has been the subject of research as a new therapeutic modality to improve root canal disinfection, revealing important and satisfactory results with significant bacterial reduction in the root canal system. 12 –15 PDT is based on the association between a light generated by a low-power laser and a nontoxic photosensitizer (dye), in the presence of oxygen. The photosensitizer excited by the laser light reacts with the molecular oxygen (O2) to generate singlet oxygen ( 1 O2) and reactive oxygen species such as superoxide (O2 -), hydroxyl radical (OH) and hydrogen peroxide (H2O2). 16 Both free radicals and 1 O2 are capable of acting in several cellular components of the bacteria through oxidation or reduction reactions, causing cellular destruction. 17
In contrast to high-power lasers, the photodynamic inactivation of microorganisms with low-power lasers is not based on temperature increase. For this reason, the use of an optical fiber in direct contact with the root canal wall may not be as essential as in high-power laser therapy.
The major advantages of not using intracanal optic fibers would be to facilitate and to simplify the technique of the light delivery system and to reduce costs. Some studies have shown bacterial reduction when PDT was used in root canals, with intracanal optical fibers, 14,18,19 or only with a handpiece placed in the root canal orifice. 12 However, there is no register of a study comparing the effects of light delivery systems using intracanal optical fibers for photosensitizer activation and light delivery systems applied at the endodontic access opening. Therefore, the aim of this study was to evaluate the effectiveness of PDT in reducing E. faecalis in root canals of extracted human teeth, with and without the aid of an intracanal optical fiber, using two irradiation exposure times.
Methods
E. faecalis suspension
A strain of E. faecalis (ATCC 29212) was reactivated in Brain Heart Infusion (BHI) broth (Difco, Detroit, MI) and incubated in an anaerobic chamber at 37°C, at a partial pressure of 5% CO2, for 24 h. The culture was spread over agar plates and incubated for an additional 24 h, under previously described conditions.
After microbial growth, a suspension compatible with pattern 2 of McFarland's scale was prepared in sterile saline. Subsequently, 5 mL of the prepared suspension was mixed with 5 mL of BHI broth to obtain the final suspension. Serial dilutions were prepared and 0.1 mL aliquots were spread over BHI agar plates. These were incubated for 24 h (5% CO2 at 37°C) to determine the number of colony-forming units per milliliter (CFU/mL).
Tooth specimens
The root segments of 60 freshly extracted human single-rooted teeth (extracted for periodontal reasons) were prepared to a standard length of 15 mm with a diamond disc (Carbodent, Gysi S.A, Buenos Aires, Argentina). The tooth specimens were obtained from the tooth bank of the Department of Dentistry of the University of Taubaté (Taubaté/SP - Brazil) and the study protocol was approved by the Ethics Committee of the University of Taubaté (protocol # 0467/07).
The canals were instrumented with hand files (Maillefer Instruments SA, Ballaigues, Switzerland) using the crown-down technique, 1 mm short of the working length (WL), to a # 45 master apical file (Maillefer Instruments SA, Ballaigues, Switzerland); canals were irrigated with 2 mL 1% NaOCl solution after instrumentation with each file. NaOCl (1%) was delivered with a 30-gauge needle (ProRinse, Dentsply/Tulsa Dental, OK). At the end of the procedure, the root canals were irrigated with 5 mL 17% ethylenediaminetetraacetic acid (EDTA) (Formula & Ação Farmácia Magistral Ltda., São Paulo, Brazil) for 3 min for smear layer removal, followed by irrigation with 5 mL of sterile saline solution to remove the residues of the chemical adjuncts used during instrumentation.
The external root surfaces were covered with two layers of epoxy Araldite (Brascola Ltda., Taboão da Serra, Brazil) to avoid external leakage. The apical foramen was subsequently sealed with composite resin (Filtek Z 250; 3M, Campinas, Brazil). The specimens were then autoclaved at 121°C for 15 min.
Under laminar-flow conditions, the teeth were randomly assigned into six groups with 10 specimens in each group, and fixed with acrylic resin chemically activated in six plates of cell culture (Corning Incorporated Costar, New York, NY).
Inoculation of E. faecalis and biofilm formation
Specimen preparation and contamination was performed as previously described by Brito et al., 20 with some modifications. Twenty μL of E. faecalis final suspension (2,58 x 108 CFU/mL) were injected into the root canal of each specimen using a 0.3 cc insulin needle (BD Ultra-Fine, NJ). Subsequently, each specimen was placed in a well and fully covered with cotton pellets wetted in sterile distilled water to ensure a moist environment. The sample and the apparatus in which it was tested were kept at 5% CO2 and 37°C for 21 days. Twenty μL of fresh BHI broth were added every 2 days to the canals and the cotton pellets in the wells were replenished, to maintain the microorganisms in the exponential phase for the formation of biofilms.
Root canals were irrigated with 1.0 mL of saline solution and sampled before (T1) and after (T2) testing procedures. The samples were taken using sterile paper points # 20 (Protaper F3, Maillefer, Ballaigues, Switzerland) placed at the working length. Paper points were transferred into an Eppendorf tube and, after vortexing the tubes for 30 sec, serial dilutions of the contents were prepared and 0.1 mL aliquots were spread over the surfaces of BHI agar plates that were stored under 5% CO2 for 24 h. After incubation, colonies were counted to determine the initial (T1) CFU/mL of viable cells of experimental and control groups.
Testing procedures
The 60 specimens were randomly distributed into six groups (n=10): one control group (untreated), one conventionally-treated group (1% NaOCl) and four groups treated with PDT using four different parameters.
In the conventionally treated group a standardized irrigation protocol was used. A 30-gauge needle (ProRinse, Dentsply-Tulsa Dental, Tulsa, OK) was placed at the WL, and 10 mL of 1% NaOCl was delivered to the specimen over a period of 15 min.
In the PDT test groups, irradiation was performed either with or without the use of an intracanal optical fiber, using a output power of 90 mW and two exposure times (Table 1). Methylene blue (MB) was dissolved in deionized water to a concentration of 0.01% or 100 μg of the dye per 1 mL of distilled water (Fórmula & Ação, São Paulo, Brazil). The canals of all specimens in the experimental groups were filled with MB solution with a 30-gauge needle (ProRinse, Dentsply-Tulsa Dental, Tulsa, OK).
OF, optical fiber; NOF, no optical fiber; IT, exposure time.
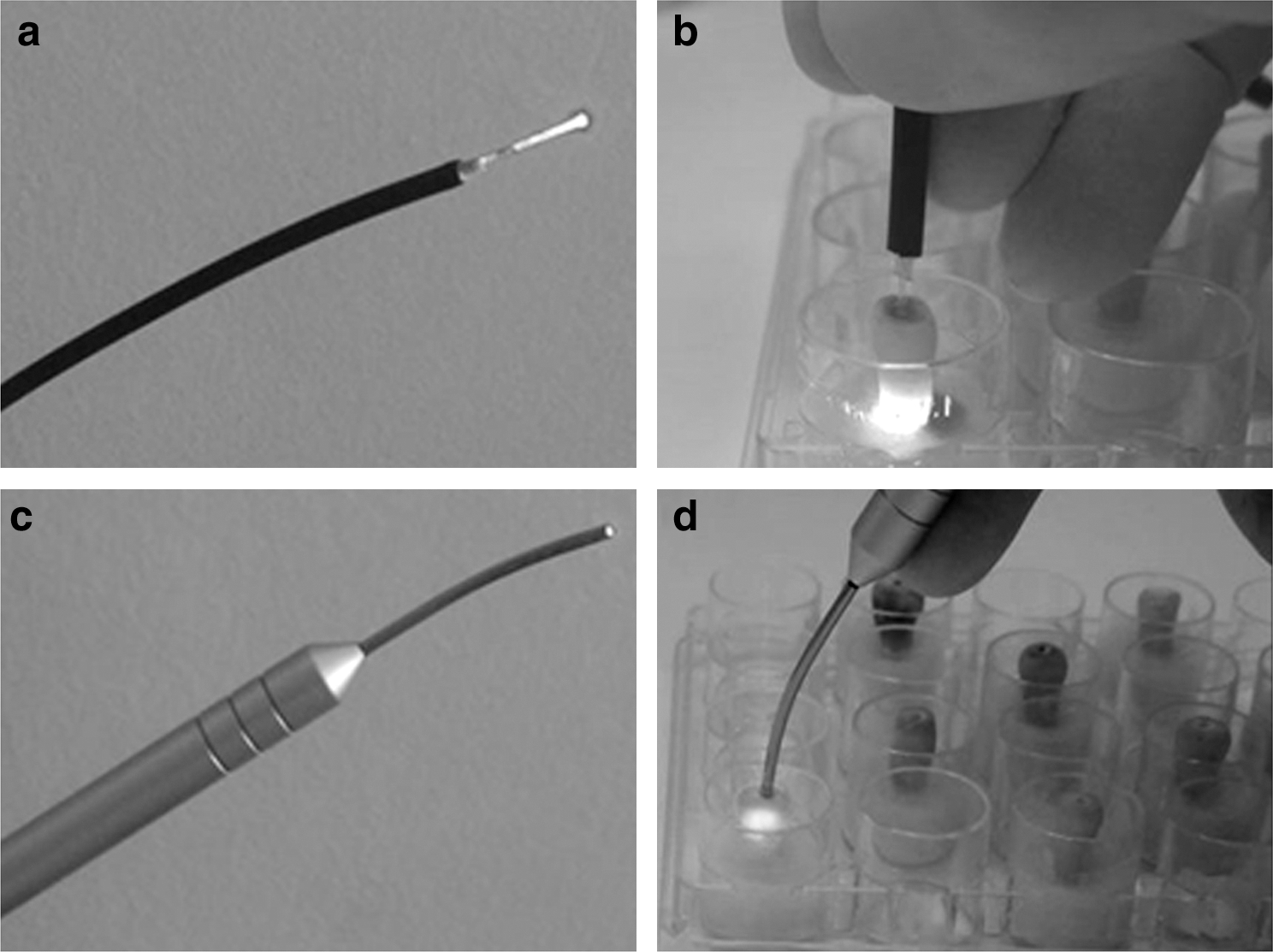
After a 5-min pre-irradiation time, the specimens were irradiated with a diode laser (Thera Lase, DMC Equipments Ltda., São Carlos, Brazil) with a 660-nm wavelength, adjustable to work at power settings between 35 and 100 mW. The system has a handpiece with 600 μm and a 216-μm conventional flexible cylindrical intracanal optical fiber with a plain tip (Fig. 1a and b). Power outputs were previous quantified with a power meter device (Power Max 600, Molectront, Portland, OR) and were set at 90 mW. When irradiation was performed with the optical fiber, it was placed in the apical portion of the root canal (at the established WL) and spiral movements, from apical to cervical, were applied to the fiber to improve the diffusion of the red light throughout the root canal. 21
Light delivery systems:
Immediately after the testing procedures, the contents of the root canals were collected, diluted and plated, as previously described. After incubation for 24 h, the CFU/mL of viable cells from each specimen was calculated (T2).
Statistical analysis
Microbiological data (CFU/mL) were transformed into logarithms and parametric tests (dependent t-test for paired samples) were performed for intra-group analysis (T1 to T2). The Kruskal-Wallis test, complemented by Dunn test, was used for the intergroup comparative analysis of these percentage reductions. Analyses were performed using BioEstat 5.0 (Universidade Estadual de Maringá, Maringá, PR, Brazil) and the significance level was set at 0.05 (p<0.05). 22
Results
The results of the antimicrobial effect of the test procedures on E. faecalis are presented in Table 2.
Percentage of bacterial growth, exhibited by the control group.
Intra-group analysis of the quantitative data was performed to investigate the ability of each procedure to reduce bacterial counts, when compared with the previous condition. Analyses showed that the number of CFU in T2 was significantly reduced in comparison to T1 in all experimental groups (dependent t-test for paired samples, p<0.05).
All specimens of the control group demonstrated an increase in the number of CFU/mL, confirming that the methodology used in this study provided sample contamination (Table 2).
The intergroup comparisons revealed that the highest percentage of E. faecalis reduction was achieved with conventional procedures by irrigation using 1% NaOCl (99.99%), with no statistical t difference (p>0.05) between NaOCl × OF/ IT180 and NaOCl × NOF/IT180. PDT- treated groups also presented high reduction percentages, in the following decreasing order: OF/IT180 (99.65%), NOF/IT180 (99.64%), OF/IT90 (99.48%) and NOF/IT90 (99.41%). No statistical difference was found among the groups treated with PDT (p>0.05).
Discussion
In recent years, in vitro and in vivo model studies have suggested that PDT may hold potential as an alternative antimicrobial approach or as an adjunct to standard endodontic antimicrobial treatment, 15,23,24 associating safety with the ease of application of a low-power laser, regardless of the manner of delivery. 25
The present study confirms that PDT significantly decreases (99.41% to 99.65%) the load of microorganisms in infected root canals. However, higher reductions were obtained after irrigation with 1% NaOCl (99.99%), when comparing this group with the PDT groups that were treated with lower irradiation times (p>0.05). Other studies have compared the disinfecting abilities of PDT and NaOCl in different concentrations, and have presented controversial results. Silva Garcez et al. 26 verified that PDT was more efficient than 0.5% NaOCl in reducing bacteria in root canals. On the other hand, Seal et al., 12 using 3% NaOCl for 10 min, and Meire at al., 19 using 2.5% NaOCl for 15 min, showed that chemical agent irrigation was more efficient than PDT. Such differences can be attributed to the diversity of methodologies, NaOCl concentrations, and PDT parameters.
In terms of irradiation exposure time, the reports show great variability, from 30 sec 26 up to 10 min. 23,27 However, the more frequently periods used are 2 min, 13 3 min, 15 and 5 min. 14,18 Based on the literature, two different exposure times (1 min and 30 sec and 3 min) were selected to assess their impact on the final results. It seems that the antimicrobial effectiveness of the PDT is better when the energy dose is increased. 12,15,28 As the energy dose is proportional to the power and irradiation time, we tried to increase the power and reduce the irradiation time, in order for the photosensitizer to remain in the root canal system for a shorter period of time, minimizing the chances of tooth staining.
The groups that were irradiated for 3 min (energy dose of 16.2 J) presented slightly higher disinfection rates when compared to the groups irradiated for 1 min and 30 sec (energy dose of 8J); however, this was not found to be statistically significant. These findings indicate that the use of the higher power settings (90 mW) allows the decrease in the exposure time without significantly compromising the antimicrobial efficiency.
The need for the association of light with photoactive dyes to achieve better antimicrobial effects is well established in the antimicrobial PDT literature. 15,23,26,27 MB was selected for this study because it is a synthetic non-porphyrin compound (phenotiazine) with maximum absortion in the visible red area, compatible with the wavelength of the laser selected (λ=685 nm) and has a high rate of generation of reactive species, generating high concentrations of 1O2. 29,30 A lower concentration of MB (100 μg/mL) was chosen to minimize the chances of dental discoloration, while preserving its photo-antibacterial properties. 25,31,32
In the present study, we compared the photoactivation of MB using two light delivery systems. Our results suggest that the use of a conventional intracanal optical fiber during PDT does not contribute significantly to the final reduction of E. faecalis, when compared with the use of a handpiece placed in the root canal orifice.
Although some studies have indicated the use of optical fibers with multiple cylindrical diffusers to uniformly distribute light at 360 degrees, 14,23 comparisons between these fibers with a conventional intracanal design optical fiber tip or other types of delivery systems were not performed. Therefore, at the present moment, there are no studies in the antimicrobial PDT literature to compare with our results.
Infiltration of dentinal tubules by MB has been shown by light microscopy, as well as by confocal scanning laser microscopy, 33 and there is strong evidence that light propagates in dentin 34 with dentinal tubules being the main scatterers. 35 Therefore, the generation and diffusion of the reactive-free radicals responsible for the photodynamic effect will be able to fully penetrate dentinal tubules, including the conventionally unreachable areas, and eliminate residual microorganisms. 14 Although the present study did not performed a microscopic analysis, our findings are in agreement with these statements and suggest that the activation of MB occurs at a distance, regardless of direct contact of the light delivery system with the photosensitizer. As such, in contrast to high-power lasers, for PDT the direct contact of the optical fiber with the root canals may be not a decisive factor for achieving the best antimicrobial effects.
Although we achieved high percentages of reduction of E. faecalis (99.41% to 99.65%) with the parameters used in this study, regardless of the use of an optic fiber, PDT was not able to achieve total bacterial elimination (100%). These findings are also reported by other studies in the literature 14,26,36 and one possible explanation for such results may be the low concentration of oxygen available in the canals, especially in irregularities and in dentinal tubules. Under such conditions, the formation of cytotoxic oxygen derivatives may be precluded or minimized. 37 Another point to consider is energy density; in this study we used an energy density of 300 mW/cm2. Soukos et al. 14 reported that the incomplete sterilization of the root canal system by PDT was not caused by the failure of MB and/or light in penetrating dentinal tubules, but caused by the high power density (740 mW/cm2) used in their study, which may have caused a rapid consumption of molecular oxygen in the low oxygenated dentinal tubule microenvironments.
PDT is a new technique. The factors responsible for the antimicrobial effects of this modality, including the penetration of the photosensitizers into the root canal system, the range of free radical activity, the light delivery system, and the energy doses used, have not been established. Further studies are required to elucidate these issues, to find consistent parameters for the application of PDT to maximize the disinfection of root canals.
Conclusion
On the basis of the results of this study, it can be concluded that PDT, used under the conditions described, was effective against E. faecalis, independently of whether or not an intracanal optical fiber was used.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.