
Abstract
Introduction
Tissue repair and wound healing are complex processes that involve inflammation, granulation, and tissue remodeling. Interactions of different cells, extracellular matrix proteins, and their receptors are involved in wound healing, and are mediated by cytokines and growth factors. 3 Wounds are heterogeneous, and the wound healing process is of a multifactorial nature, influenced by many external factors and compounds. The use of models is inevitable in order to gain new knowledge about the complexity of this process. Experimental models are also necessary for investigating product safety and efficacy during the development of specific biological treatments for clinical use in wound healing. 11
Curcuma longa Linn, a tropical herb belonging to the ginger family (Zingiberaceae), is a well-known culinary agent and food additive used to produce a yellow color. Extensive research over the past three decades has clearly established the biological and pharmacological efficacy of curcumin. This drug is known to have potent antioxidant, anti-inflammatory, and anti-infectious properties that make it a unique molecule for wound healing applications and for treating a variety of inflammatory diseases including atherosclerosis, Alzheimer's disease, diabetes, osteoarthritis, and inflammatory bowel disease. 12 –14 Curcumin has been reported to be effective in wound repair in normal and diabetes-impaired healing, when used both orally and topically. 12 It exerts inhibitory activity against hydrogen peroxide-induced oxidative damage in human keratinocytes and fibroblasts, 15,16 and has also been reported to have potent antioxidant activity 12 –16 and to confer protection against irradiation in vitro and in vivo. 13,17 Some articles 18,19 have shown that curcumin-treated wounds heal much faster as indicated by improved rates of epithelialization, wound contraction, greater deposition of collagen, and an increase in transforming growth factor β-1. The apparent greater number of myofibroblasts in curcumin-treated wounds may be partially responsible for the fast wound contraction. 18
The present study was designed to evaluate the effect of topical curcumin on the healing of skin wounds produced by the CO2 laser in an animal model.
Methods
Study design
A prospective, randomized, experimental design involving three groups of mice was used to compare CO2 laser-induced skin wound progression with topical curcumin or application of its vehicle.
Animals
The animals used in this study were obtained from the Faculty of Medicine of the University of Murcia (Spain). Ninety adult (6 weeks of age) SKH-1/CRL mice (males) and with a mean weight of 25 g (range, 20–35 g) were used, following a protocol approved by the Bioethics Committee of the University of Murcia. The animals were individually housed in plastic cages in a monitored environment (21°C, 12:12 h light cycle), with free access to drinking water and a standard laboratory mice food pellet diet. The animals were monitored for signs of infection and discomfort before and after surgery, and up until euthanasia. Housing and care of the animals was in accordance with the Spanish National Research Council guidelines. 20
Materials
A Lasersat 20 W (10 J/cm2) Satelec® CO2 laser was used (Pierre Rolland, Satelec®, S.A. Barcelona, Spain) at a continuous power setting of 6 W.
Curcumin was purchased from Sigma-Aldrich Chemical, Co. (Madrid, Spain). The drug was accurately weighed and dissolved in dimethylsulfoxide (DMSO) to yield a curcumin end concentration of 10% W/V.
Surgical procedure
The 90 mice were randomized to 3 groups (30 animals per group), with the creation of 6-mm incisions in the skin of the dorsal region by means of the CO2 laser. No product was applied to the resulting wound in group I (control group); vehicle was applied immediately after irradiation in group II; and topical curcumin was applied to the mice in group III.
The animals were anesthetized with a mixture of ketamine and xylazine (50%). All incisions were made in the skin of the dorsal region by a single surgeon, and using the same laser technique in all cases (perpendicular to the dorsal skin surface). An adhesive plastic ring measuring 6 mm in diameter was affixed to the surface to ensure that all wounds were of the same size. The distance of the laser probe from the skin was 20 mm.
The CO2 laser was equipped with a straight probe with a 1.25-mm diameter spot size, and was applied for 5 sec to a 6 mm2 surface. The laser operating in continuous pulse mode at 6 W delivered a total energy density of 50 J/cm2 to the skin of the animal.
In all three groups, the CO2 laser was used to produce three wounds spaced 4 cm apart. In group I (control) the laser was applied without subsequent wound treatment; in group II the wounds were treated with DMSO vehicle immediately after irradiation (5 mg/day by wound); and in group III the animals received topical curcumin (5 mg/day by wound at a concentration of 10% W/V) until euthanasia. The wounds were not covered with gauze, because of the difficulty of keeping the dressing in place (Fig. 1).

Application of curcumin treatment on wound in dorsum mouse with a cotton-tipped applicator.
The mice in each group were killed 2 (10 animals by group), 7 (10 animals by group), and 14 days (10 animals by group) after surgery by CO2 inhalation, to compare the degree of re-epithelialization and inflammation in each group. A biopsy was obtained using an 8-mm punch. The samples were placed in individual containers with 10% formaldehyde solution, marked with the number assigned to each animal.
Histopathological study
The biopsy specimens were embedded in paraffin and cut into 5–7 μm sections along a plane perpendicular to the incision. The sections were stained with hematoxylin and eosin, and examined under magnifications of ×20, ×40, and ×100. All samples were studied by a single individual blinded to the study.
The criteria developed by Sinha and Gallagher 9 were used to measure the degree of re-epithelialization: grade 0=re-epithelialization at the edge of the wound; grade 1=re-epithelialization covering<50% of the wound; grade 2=re-epithelialization covering>50% of the wound; grade 3=re-epithelialization covering the entire wound, with irregular thickness; and grade 4=re-epithelialization covering the entire wound, with normal thickness.
The degree of inflammation in turn was measured using the inflammation resolution phases described by Cotran et al.: 21 grade 1=acute inflammation (a pyogenic membrane is formed); grade 2=predominance of diffuse acute inflammation (predominance of inflammatory cells); grade 3=predominance of chronic inflammation (fibroblasts begin to proliferate); and grade 4=resolution and healing (reduction or disappearance of chronic inflammation, although occasional round cells may persist).
Statistical analysis
The data were analyzed using the SPSS version 12.0 statistical package (SPSS® Inc., Chicago, IL). A descriptive study was made of each variable, and the associations between the different qualitative variables were examined using Pearson's χ2 test. Statistical significance was considered for p ≤ 0.05.
Results
Re-epithelialization
Two days after wound induction, most of the samples presented incomplete re-epithelialization, in all three study groups. After 7 days, 73.33% of the wounds treated with curcumin presented grade 3 re-epithelialization; nevertheless, only 37.50% of the wounds in the control group and 41.67% in the vehicle group showed this re-epithelialization grade, showed statistical significance (p=0.048). After 14 days, all the wounds had completed re-epithelization (grades 3 and 4) (Table 1) (Fig. 2).
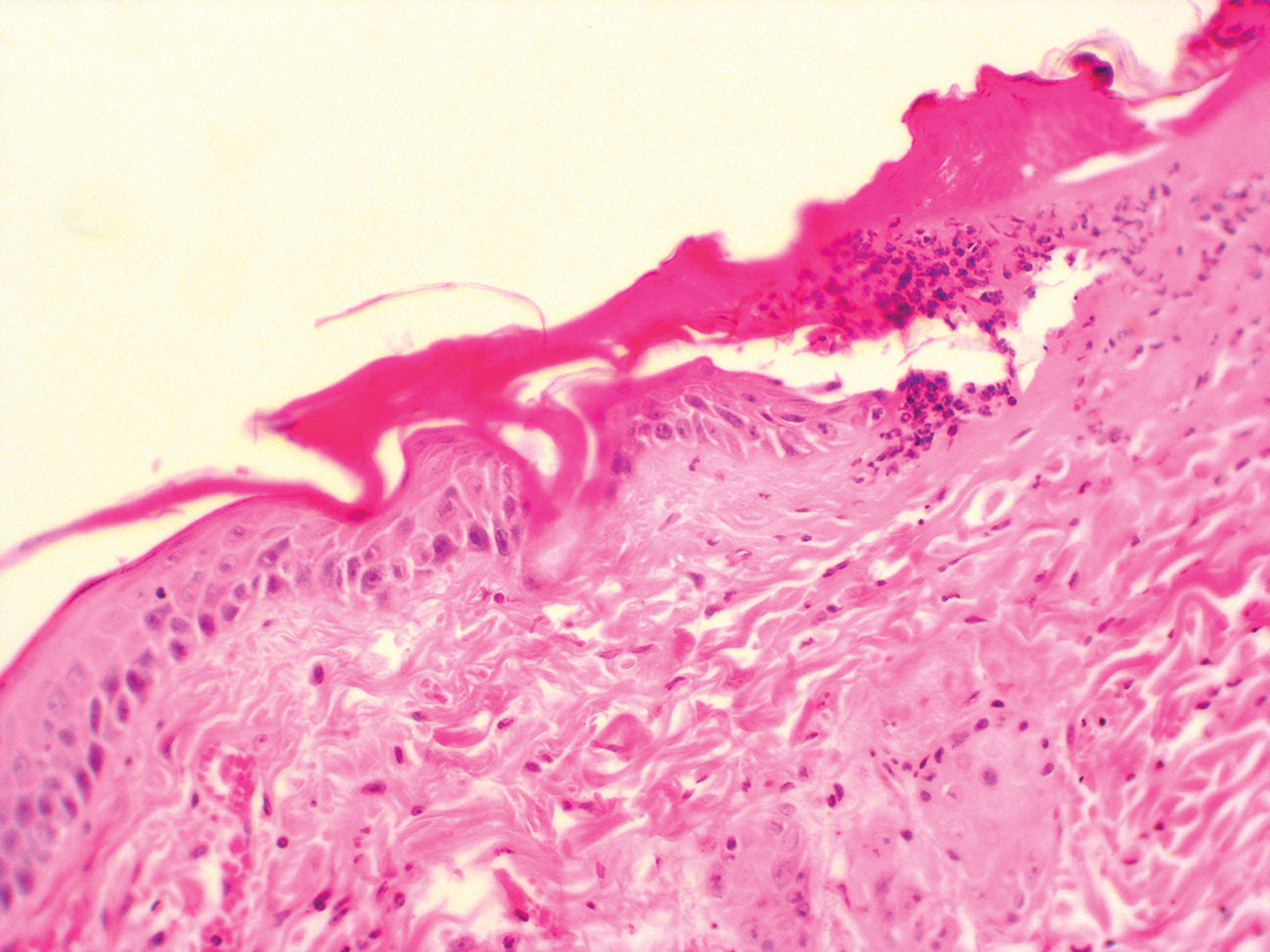
Histopathological image showing a wound after surgery grade 1 (curcumin group, 2 days after surgery) (hematoxylin and eosin, original magnification ×20).
Vehicle=DMSO (dimethylsulfoxide)
Grade 0, re-epithelialization at the edge of the wound; Grade 1, re-epithelialization covering>50% of the wound; Grade 2, re-epithelialization covering>50% of the wound; Grade 3, re-epithelialization covering the entire wound, with irregular thickness; Grade 4, re-epithelialization covering the entire wound, with normal thickness.
Inflammation
Two days after wound induction, none of the groups showed complete resolution of the inflammatory process. After 7 days, 36% and 40% of the mice in group III (topical curcumin) presented grade 3 and grade 4 resolution, respectively, although no statistically χ2 test). significant differences were observed. After 14 days, grade 4 resolution was recorded in all three groups (Table 2).
Vehicle=DMSO (dimethylsulfoxide).
Grade 0, coagulative necrosis (imperceptible inflammatory response); Grade 1, acute inflammation (pyogenic membrane is formed); Grade 2, predominance of diffuse acute inflammation (predominance of inflammatory cells); Grade 3, predominance of chronic inflammation (fibroblasts begin to proliferate); Grade 4, resolution and healing (reduction or disappearance of chronic inflammation, although occasional round cells may persist).
On examining the width of the damage lateral to the incision, pseudoepitheliomatous hyperplasia was noted in the different groups (Table 3) (Fig. 3).
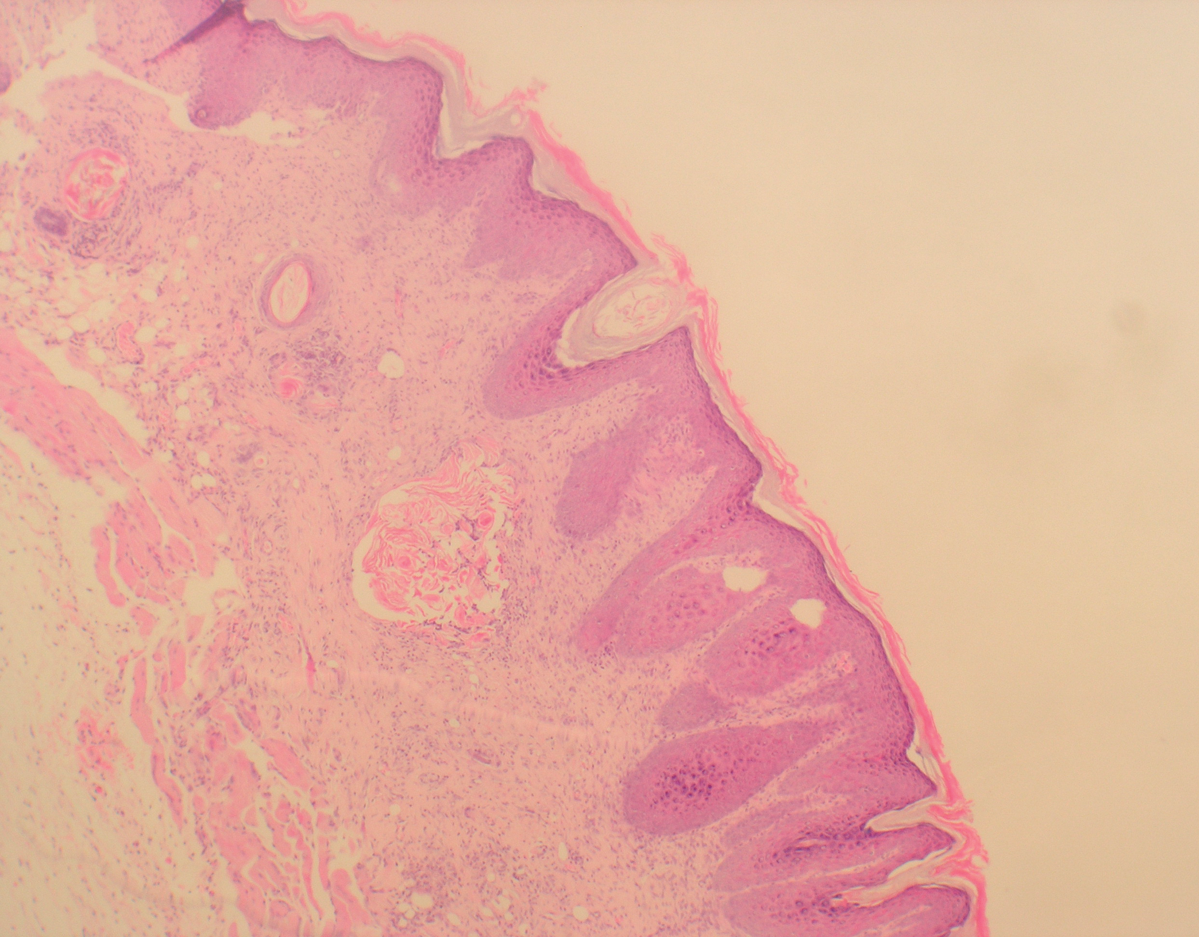
Histopathological image showing pseudodysplastic epithelial artefacts (vehicle group, 14 days after surgery) (hematoxylin and eosin, original magnification ×40).
Vehicle=DMSO (dimethylsulfoxide).
Discussion
The wound healing process comprises a series of coordinated responses to tissue injury, resulting in tissue contraction, closure, and restoration. The longer it takes for spontaneous wound healing, the worse the outcome tends to be, with an increasing likelihood of hypertrophic scarring and unsightly alterations. In the present study, the rats in which the CO2 laser was used to produce skin wounds that were subsequently treated with topical 10% curcumin showed faster re-epithelialization than the rats in the other two groups, with statistically significant differences after 7 days.
We have used the same re-epithelialization criteria as Sinha and Gallagher 9 in 2003. According to Cotran et al., 21 cutaneous wound repair consists of a well-defined series of events arbitrarily divided into three overlapping phases. The defining features of phase 1 are inflammation and resorption (0–7 days), with edema as the earliest manifestation, followed by the infiltration of inflammatory cells (neutrophils followed by macrophages and lymphocytes) that clear the wound of damaged cells and foreign material and, in turn, release growth factors and biochemical compounds that activate tissue regeneration. Neovascularization and provisional matrix formation (3–14 days) in turn define phase 2, with new blood vessels growing in primarily from tissues subjacent to the wound. Provisional matrix is characterized first by proteoglycan secreted by connective tissue cells, followed by collagen synthesis by activated fibroblasts. The early collagen fibers are relatively thinner and aligned parallel to the blood vessels (perpendicular to the wound surface). During this time, and particularly in rodents, there is connective tissue contraction and epidermal growth over the wound surface. Phase 3 is a period of wound remodeling (10 days to 6 months) characterized by the obliteration of new blood vessels, reduction of proteoglycan matrix, and collagen remodeling with resorption of early collagen and the formation of new collagen fibers oriented along the stress lines.
According to the review published by Peplow et al., 3 rodents are attractive for wound healing studies because of their availability, low cost, and easy handling characteristics. Murine models of wound healing offer several advantages over models in other species, including the fact that mice are inexpensive, therefore allowing studies to be performed with large sample sizes. Despite such advantages, however, mouse skin healing does not perfectly mimic human skin wound healing, because the skin is morphologically different. Developing an animal model that has all the complexity of human chronic wounds may be an unattainable goal, because nonhealing and delayed- healing wounds in humans are often the result of combinations of impaired circulation, inadequate nutrition, age, limited physical activity and/or chronic physiological imbalances.
We decided to use curcumin in accordance with the studies of Sidhu et al. 11 and Singer et al. 16 This substance been shown to enhance wound healing in a mouse model of full-thickness injuries. Curcumin-treated biopsy wounds showed an increased presence of neutrophils, macrophages, and fibroblasts. Also, myofibroblasts demonstrated faster wound contraction in wounds treated with curcumin. Such treatment has resulted in an enhanced expression of fibronectin and collagen, leading to increased formation of granulation tissue, neovascularization, and faster re-epithelialization. When multiple wounds are made in experimental animals, there is always the possibility that subsequently made wounds will be affected by bioactive mediators released from the initial wounds. This represents a possible weakness in the design of this study.
Our results further support the effectiveness of curcumin in wound healing. In this sense, Panchatcharam et al. 19 have described that topically administrated drugs are effective in faster wound contraction and healing because of the larger availability at the wound site. Curcumin treatment was shown to decrease the levels of lipid peroxides (LPs), whereas the levels of superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) activities were significantly increased exhibiting the antioxidant properties of curcumin in accelerating wound healing
We have used the topical curcumin concentration recommended by Gopinath et al. 15 and Singer et al., 16 although different concentrations and vehicles should also be tested. Unfortunately, curcumin does not seem to be well absorbed when taken orally, and high doses of the drug have apparently failed to yield clinically or pharmacologically relevant blood concentrations. 11 –16
The CO2 laser offers great precision, minimal intraoperative bleeding, sterilization of the surgical area, healing with minimal scarring, and decreased postoperative swelling. As a result, it is widely used in surgery. 3 The disadvantage of laser systems is represented by histologically evident thermal destruction around the laser beam incision and thermal damage. According to Seoane et al., 22 and taking into account the inherent limitations of experiments of this kind, the CO2 laser generates epithelial thermal damage that can simulate mild dysplastic changes with cytological atypias affecting mainly the basal and suprabasal layers. These changes must be taken into account in order to avoid erroneous diagnoses and therapeutic approaches.
Conclusion
In conclusion, our results suggest that 7 days after skin wound induction with the CO2 laser and subsequent treatment on a daily basis with topical curcumin, wound re-epithelialization is significantly more advanced than in the rest of the groups. Nevertheless, further studies are needed to produce data allowing the extrapolation of such effectiveness to wound repair in humans.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.