
Abstract
Introduction
Red blood cells were thought to be able to store large amounts of nitric oxide, partly in the form of nitrosothiols, 15,16 and hemoglobin has been found to be able to absorb this wavelength of photo energy. 3 Nitric oxide has been documented to be a powerful vasodilator, with only small amounts leading to an increase in cyclic guanosine monophosphate (cGMP) and resulting in the relaxation of contractile proteins found in the smooth muscle walls of vascular tissue. 17 MIRE could promotes the release of small amounts of nitric oxide from the hemoglobin in the red blood cells passing through the blood vessels underneath the diode array, causing vasodilation and an increase in microcirculation. 2 This increase in capillary blood flow would subsequently facilitate the process of oxygenation and the delivery of an endogenous growth factor and white blood cells to the healing tissues, thus promoting a positive healing environment. 2
Recently, it was demonstrated that near-infrared photo energy, similar to MIRE, could increase blood flow in rats, partly through an effect mediated by endothelial nitric oxide synthase or nitric oxide. 18 In humans, only one case study showed that MIRE increases microcirculation in the skin of the lower limbs. 2 The aim of the present study was to evaluate the immediate influence of MIRE on the microcirculation of the skin surface, using video capillaroscopy to measure blood cell velocity inside the capillaries of nailfold, and laser Doppler flowmetry (LDF) to record the superficial skin blood flow in healthy subjects.
Materials and Methods
Subjects
Thirty-five healthy subjects, aged 21–65 years, were recruited by convenience sampling. Five subjects (1 female, 4 male) were excluded because their capillary loop over the nailfold of the left big toe could not be identified by the use of video capillaroscopy; therefore, 30 subjects completed the study. Other exclusion criteria were people with diabetic mellitus, peripheral vascular disease, dermatological lesions over their feet, or those with a smoking habit, those taking medications that might influence platelet aggregation or vasodilation, those with a previous injury to the left lower limb that could affect blood circulation, and those with active malignancies or who were pregnant. The study was approved by the Ethics Committee of a local university (reference number: HSEARS20090209004). Written consent was obtained after explaining the purpose and procedures to each subject.
The subjects were then randomly allocated into: (1) the active MIRE group (n=10), (2) placebo group (n=10), or (3) control group (n=10) by drawing lots using the non-replacement method (Fig. 1). Throughout the study, both the subjects and the investigator were blinded to the group allocation.
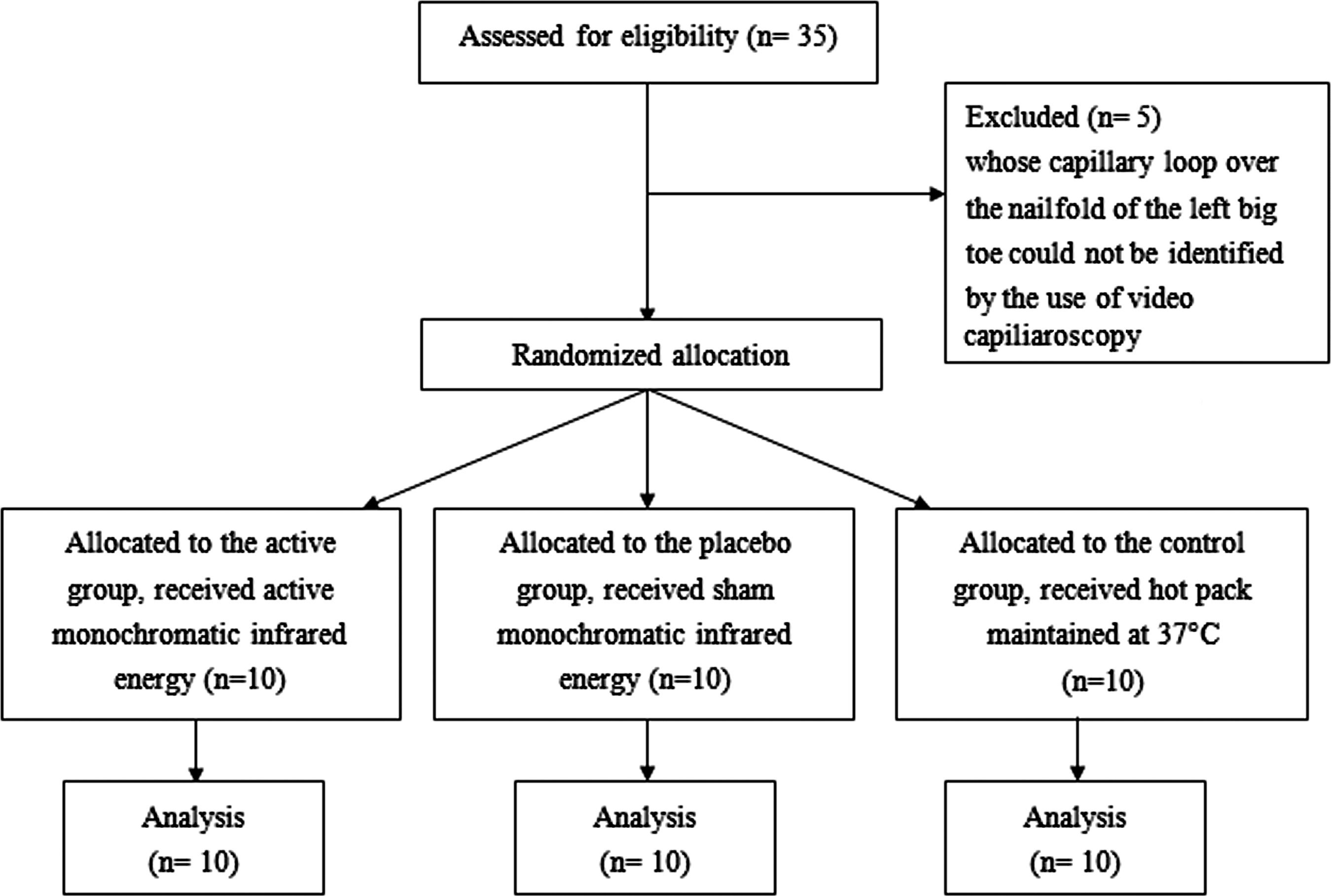
The consort diagram.
Procedures
The study was conducted in the same investigation room, in which the temperature was kept at 24±1°C, the relative humidity was kept at ∼40–60%, and the environment was quiet. All of the participants were asked to refrain from caffeine for 12 h. They were told to avoid having meals, taking hot baths, using topical agents or creams, or exercising vigorously 2 h prior to the experiment. Demographic data about the age, gender, body weight, and height of the participants were recorded. For acclimatization, the subjects were asked to take a 30-min rest in a supine lying position on a plinth.
Interventions
In the active MIRE group, the subjects received a single 30-min session of MIRE. Four array diode therapy pads of the Anodyne Therapy System (Model 480, Anodyne Therapy Professional System, FL) were placed on the lower left limb of each subject (see Fig. 2). The MIRE device comprised an array of 60 x 890 nm LEDs attached to flexible pads (3×7.5 cm). Each diode spot size was 0.2 cm2, and each LED power was 12 mW with a power density of 60 mW/cm2. The arrays were placed in direct contact with the skin for 30 min delivering a total fluence of 108 J/cm2 over an area of 22.5 cm2. The MIRE system was calibrated before the study, and the output of each diode functioned properly. The four pads were placed on the dorsal aspect of the foot, the plantar aspect of the foot just proximal to the third metatarsal head, and the medial and lateral sides of the calf. The wavelength was 890 nm, and the dosage of the MIRE unit was set at 21.67 mW/cm2. 10 During the treatment, the participants were asked to rest in a supine lying position with the left foot and ankle supported and stabilized in a neutral position with a footrest holder. For the placebo group, the procedures were the same except that the sham Anodyne Therapy System (no MIRE output was emitted) was used by turning the switch of a switch box in which the output circuit was disconnected. No MIRE was given to the control group. Instead, four warm packs similar in size to the MIRE therapy pads were placed at the same sites on the left foot, and the temperature was maintained at 37°C for 30 min, mimicking MIRE's mildly warm sensation on subjects during its operation. This was done to rule out the possible confounding factor of the mild warming effect itself, rather than the photo energy of MIRE, in changing blood circulation.
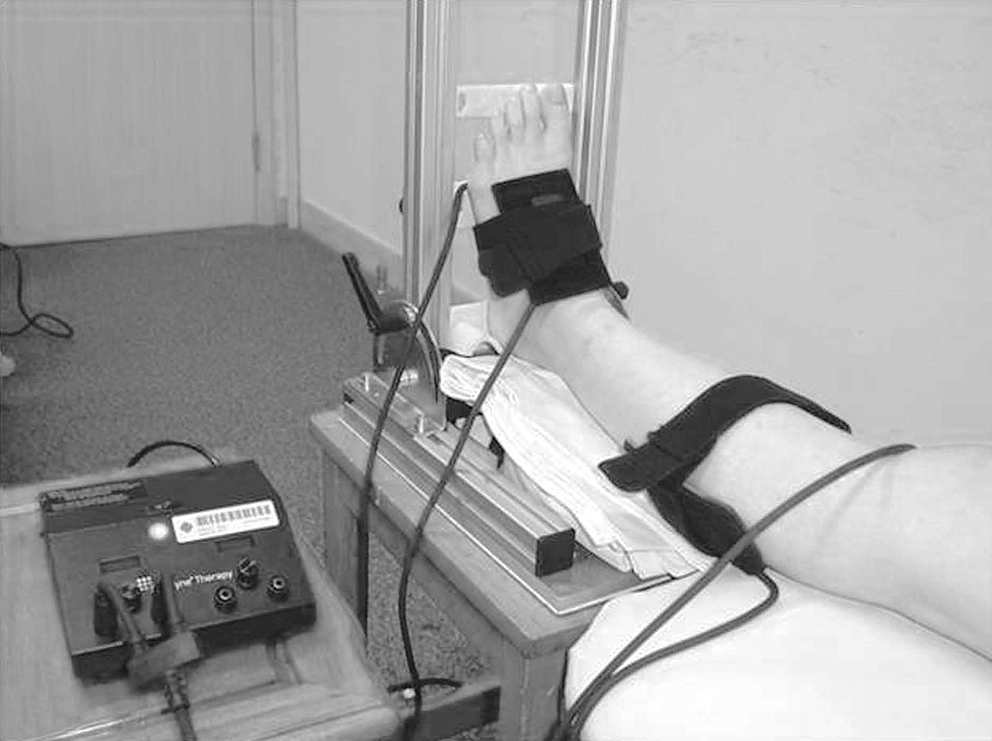
The placement of the four array diode therapy pads of the monochromatic infrared unit.
Outcome measures
Capillary blood cell velocity (μm/s)
A video capillaroscopy (CAM1 Capillary Anemometer CapiScope System, KK Technology, England) was used to measure the capillary blood cell velocity (CBV) in the nailfold parallel to the surface of the skin when the subject lay in a supine position (Fig. 3). Video capillaroscopy has been validated in previous studies and is commonly used to investigate skin microcirculation by assessing the localized blood cell flow through a direct view of the capillary loops of the nailfold parallel to the surface of the skin of fingers or toes (Fig. 4). 19,20 The left foot was stabilized by the use of a footrest holder. The location of the skin under investigation (the midpoint of the nailfold of the left great toe) was identified and highlighted with a permanent marker. To minimize laser beam reflections, a drop of paraffin oil was applied to the skin. In order to analyze the capillary blood cell velocity, five capillaries with good optical signals were located. They all showed a good contrast difference between the moving objects and the surrounding tissue. 21 Precise focusing on the nailfold capillaries were performed and their CBVs were recorded for a period of 1 min. The mean CBV of the five identified capillaries of the individual was reported in each before or after the intervention.

Nailfold capillaries captured by video capillaroscopy for a subject lying in a supine position.
A typical image of capillary loop shown by video capillaroscopy (original magnification ×200).
Superficial skin blood flow (flux) and skin surface temperature (°C)
A LDF (DRT4, Moor Instruments Ltd., England) was used to measure the superficial skin blood flow (flux) and skin surface temperature (°C). LDF is a validated tool for examining microcirculation in superficial tissues. 22 The skin blood flow is presented in flux, which is an arbitrary unit that is directly proportional to the volume of blood flowing in tissues underneath the probe. 23 The two LDF probes were adhered to the dorsal and plantar surface of the third metatarsal head just distal to the therapeutic pads by means of double-sided adhesive tape. The flux and skin surface temperature were recorded for 3 min and the averaged data obtained in the last 2 min were calculated. The two LDF probes were kept in place throughout the whole study period to ensure that the measurement sites remained the same before and after the intervention.
The abovementioned assessment tools were used to examine different aspects of skin microcirculation. Video capillaroscopy can directly assess the local blood cell velocities at the capillary level. Nailfolds are rich in capillaries, where the nutritive blood flow can be assessed. In contrast, LDF examines the compartment flow occurring in various structures including arterioles, venous plexuses, and arteriovenous anastomoses. 24 Furthermore, the assessment site of the video capillaroscopy was relatively distal to the treatment site, whereas the LDF was next to the treatment site, and therefore relatively more proximal.
Statistical analysis
The data were analyzed using the Statistical Package for Social Science (SPSS) version 16. Demographic data (age, weight, and height) and the baseline characteristics of the active MIRE group, placebo group, and control group were compared using one-way ANOVA. The changes in the pre- and post-intervention measurements of the CBV, flux, and skin surface temperature of the three groups were compared by using one-way ANOVA. The α level was set at 0.05. Post-hoc comparisons were performed if significant differences existed among the groups.
Results
Demographic characteristics of the participants
Thirty healthy subjects from 21 to 62 years of age were recruited. Their body weight ranged from 42 to 90 kg, and their height from 140 to 180 cm. There were no significant differences in demographic data or baseline measurements among the three groups (Table 1).
Data are mean±SD; no significant difference was found in any of the demographic characteristics and baseline measurement.
CBV
Figure 5 shows the changes in the mean CBV (CBV of post-intervention – CBV of pre-intervention) of the active MIRE group, placebo group, and control group. The intra-individual variability determined by the coefficient of variation ranged from 15 to 22% before and after treatment in the three groups. We found positive changes in CBV in both the active MIRE group and the control group, indicating an increase in microcirculation. In contrast, there was a negative change in CBV in the placebo group, indicating a decrease in microcirculation. The group difference reached significance (F=11.98, df=2,27, p<0.001). Post-hoc Tukey Honestly Significant Difference (HSD) test showed that the differences mainly came from the comparisons made between the active MIRE group and control group (p=0.032), and the active MIRE group and placebo group (p<0.001). No significant difference was found between the control group and the placebo group (p=0.089).
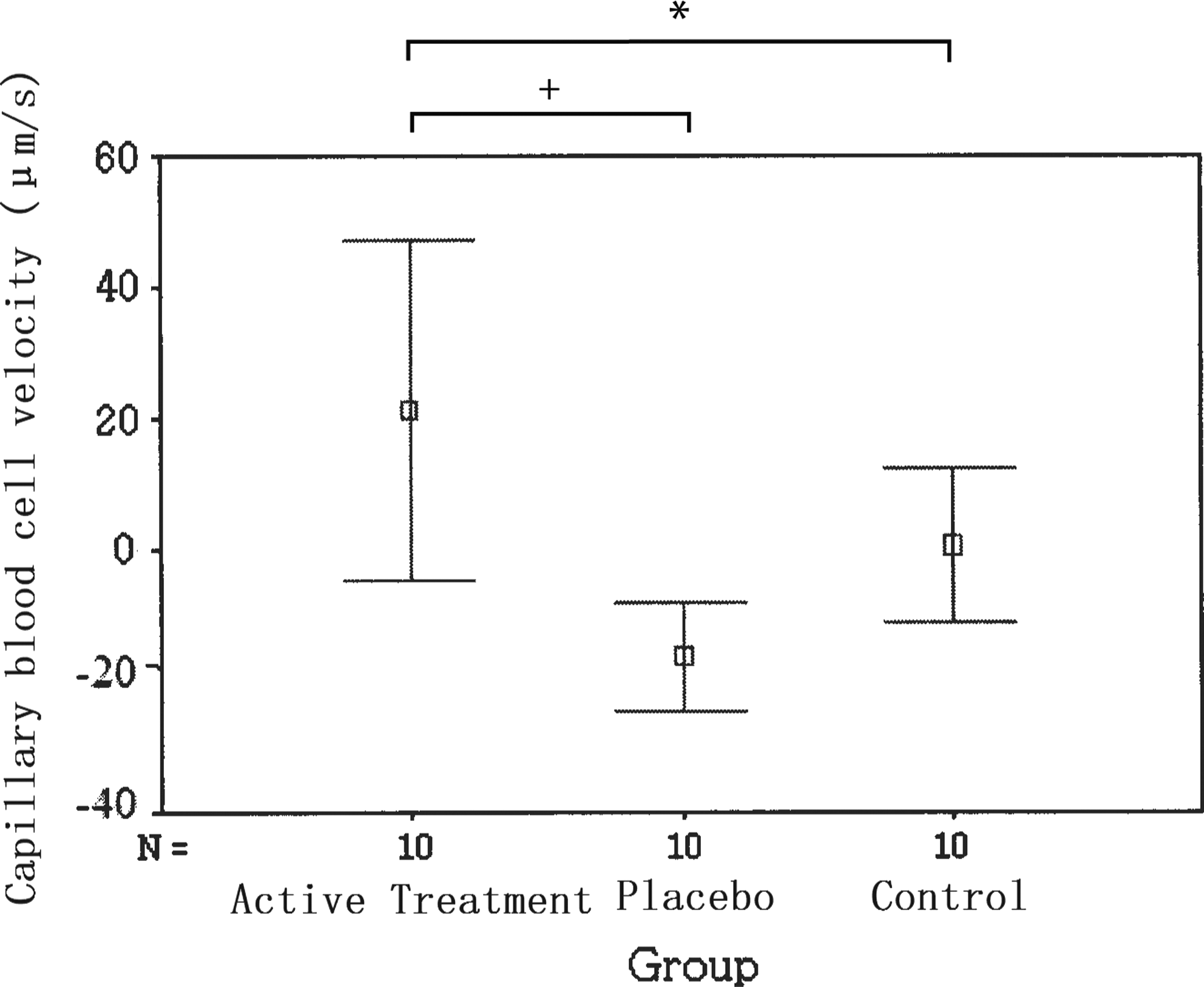
The changes in the mean capillary blood cell velocity (CBV) of the three groups. The error bars correspond to the standard deviation *p<0.05; + p<0.001.
Superficial skin blood flow (flux) and skin surface temperature (°C)
Flux and skin surface temperature were measured on both the plantar and dorsal aspects of the left foot before and after the intervention. Figure 6 shows the changes in the mean of the flux (flux obtained post-intervention – flux obtained pre-intervention) of the active MIRE group, placebo group, and control group. We found a positive change in the flux of the active MIRE group, indicating an increase in microcirculation. In contrast, there was a negative change in the flux of both the control group and the placebo group over both the plantar and dorsal aspects, indicating a decrease in microcirculation. One-way ANOVA demonstrated a significant difference among the three groups over both the plantar and dorsal aspects (plantar aspect: F=6.08, df=2,27, p=0.007; dorsal aspect: F=5.46, df=2,27, p=0.010). Post-hoc Tukey HSD test showed that the differences mainly came from the comparisons between the active MIRE group and control group (p=0.028/0.009), and the active MIRE group and placebo group (p=0.045/0.012) for the plantar and dorsal aspects, respectively. No significant difference was found between the control group and placebo group for either the plantar or the dorsal measurements (p=0.872/0.832).
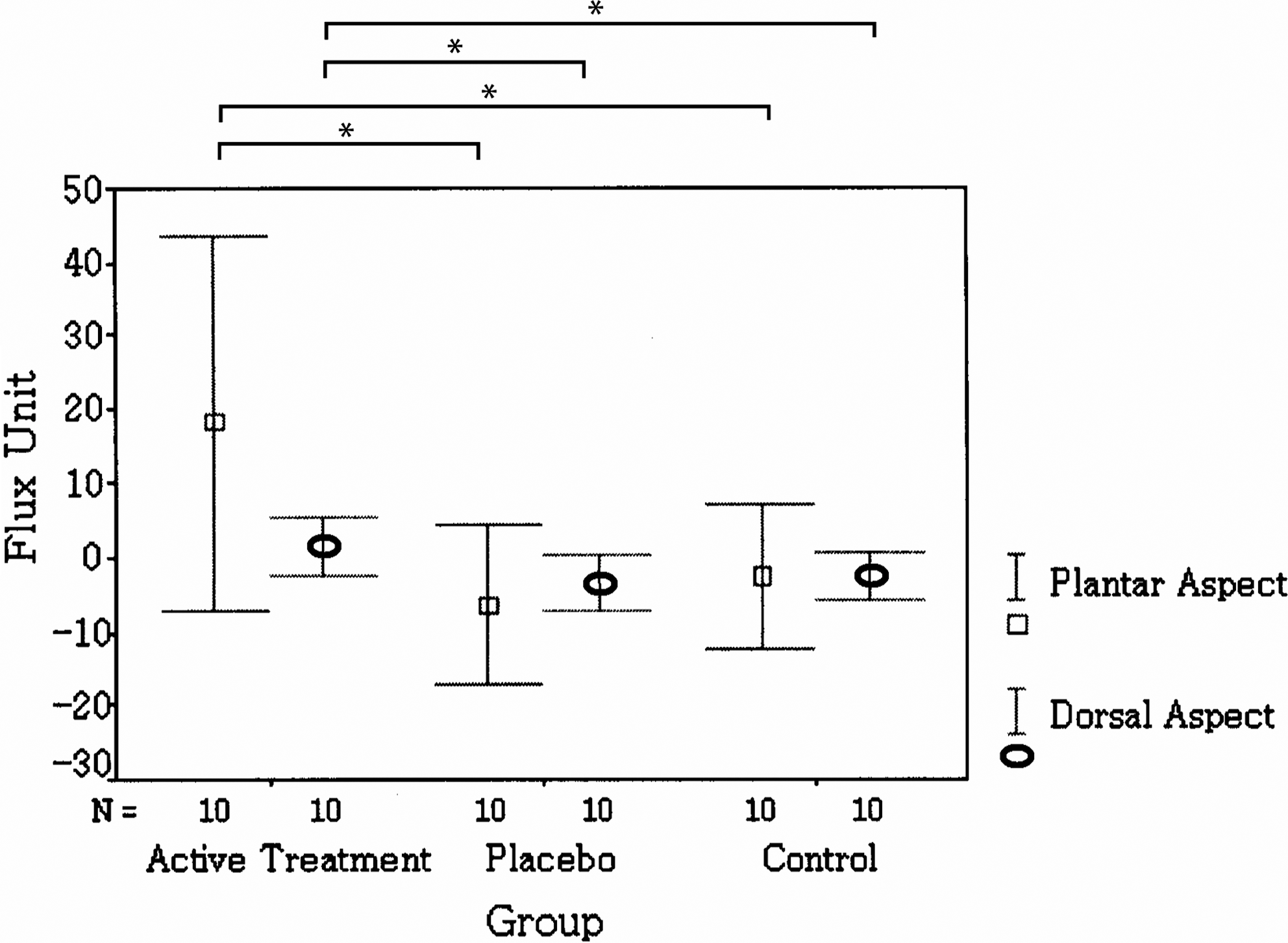
The changes in the mean flux unit of the three groups. The error bars correspond to the standard deviation *p<0.05.
For skin surface temperature over the plantar aspect of the foot, no noticeable changes in mean temperature were recorded in the active MIRE group and control group (0.02°C/0.06°C), but a small decrease was recorded in the placebo group (-0.33°C). For the dorsal aspect of the foot, a small decrease was observed in all three groups (active MIRE group: −0.14°C, placebo group: −0.32°C, and control group: −0.05°C). However, no significant difference in skin temperature was found among the three groups on either aspect of the foot (all p>0.05).
Discussion
Our findings demonstrated that a 30-min application of MIRE can significantly increase the microcirculation of the skin of the foot at both the capillary and compartment levels, as compared to a placebo group and control group. This was the first randomized, controlled study to investigate the effects of MIRE on microcirculation and show positive findings. Previously, a case study showed that a 30-min treatment of MIRE produced a 400% increase in local blood flow of the tissues as compared to the baseline, using scanning laser Doppler as the assessment tool. 2 In our present study, the 30-min MIRE treatment only produced an increase of ∼30% in microcirculation as measured by video capillaroscopy and a 20% increase as measured by LDF. Unfortunately, the dosage of MIRE used in Burke's study 2 was not clearly mentioned, and therefore it was difficult to compare their results with our findings. The increase in microcirculation in the foot can improve blood supply to nutritive capillary blood flow, which may be useful for promoting wound healing in people with diabetic ulcer.
Recently, a randomized and controlled study examined the effects of a 12-session treatment of MIRE on peripheral circulation and sensation in people with diabetic peripheral neuropathy. Peripheral circulation was indirectly evaluated by measuring the perfusion of oxygen in local tissue. 25 The authors of that study reported that MIRE might produce a greater increasing trend in the perfusion of oxygen in local tissue as compared with the sham group, but the between-group difference was just short of significance (p=0.07). They explained that the lack of significance could be partly caused by the small sample size and unequal baseline measurement of the oxygen perfusion values between groups. The present study was performed on healthy subjects who were free from any disease that could influence their circulation; no difference was found in any baseline measurement among the groups. This allowed for comparisons to be made more easily among the groups after the intervention. However, patients with disease may respond differently from healthy subjects.
The present study recruited the warm pack group as a control group. The warm pack that we used was a disposable type of warm pack, in which the heat energy was released by chemical reaction and the temperature was supposed to be able to keep warm for 4–6 h. We only observed mild elevation in skin temperature at the plantar of foot after intervention in both the active MIRE group (0.02°C) and control group (0.06°C). Note that the warm packs were delivered at 37°C, to mimic the warm sensation produced by the MIRE. The room temperature of the study room was controlled at ∼24°C. The heat energy provided by the four warm packs or MIRE treatment pad were adequate to compensate for the heat loss caused by the cool temperature in the room or the 30-min resting for acclimatization. This may explain why a mild decrease in microcirculation but no significant changes in mean temperature were recorded in the feet of the control group who received the warm pack treatment.
Interestingly, even though the skin temperature for the MIRE group was similar to that of the control group, the microcirculation in the active MIRE group was significantly greater than in the control group. This indicates that the increase in microcirculation by MIRE cannot be explained by the warming effect of MIRE alone. Instead, it is caused by the photostimulation produced by MIRE, which may the result of an increase in the release of nitric oxide to the blood vessels. 2 As suggested by previous studies, nitric oxide may be released by endothelial cells or red blood cells, or both. 26,27 This release in nitric oxide may improve microcirculation via an alteration of cGMP-mediated vasodilation at the site of the treatment. 28 Nitric oxide was not measured in any subjects during MIRE treatment in our study. Future study examining the change of nitric oxide content will be needed to confirm this postulation.
Our findings demonstrated that active MIRE produced a greater increase in flux over the plantar surface after the intervention (change in mean flux: 18.1 unit), as compared to the dorsal surface of the feet (change in mean flux: 1.5 unit). The change in flux observed at the dorsal and plantar aspects of the feet were to a different extent, probably because of the structural difference in the skin. The apical (glabrous) skin is present at the plantar surface of the foot where numerous arteriovenous anastomoses are present, which are controlled by sympathetic vasodilator nerves for thermoregulation. 29 In contrast, predominantly non-apical (hairy) skin is present over the dorsal aspect of the foot. Within this type of skin, very few arteriovenous anatomoses are found and they are innervated by both sympathetic vasodilatory and vasoconstrictor nerves. 29 Our findings demonstrated that MIRE appears to produce greater change in flux at the plantar surface of the foot, which seems to be mainly the result of the influence on the arteriovenous anatomoses.
Small sample size is a limitation of the present study. It is well known that there are individual differences in the measurement of flux by LDF. The variation of the baseline flux can be attributed to individual differences. Therefore, the present study calculated the changes of flux before and after intervention, and the differences among groups were compared. Hence, each subject served as his or her own control, and this can minimize the impact of individual difference on the experimental findings.
The present study only examined the effects of a single session of MIRE treatment on microcirculation. A future study can evaluate the effects of a course of MIRE on microcirculation with a longer follow-up period.
Conclusions
Very limited studies have examined the effects of MIRE on microcirculation. The present study evaluated the influence of MIRE on the microcirculation of the skin surface of the feet in healthy subjects. We found that 30 min of MIRE produced a significantly greater increase in both the CBV and flux of the feet of healthy subjects than in the placebo group or control group (all p<0.05).
Following 30 min of active treatment with MIRE, a significantly greater increase in both the CBV and flux of the feet was observed in healthy subjects, as compared with a sham MIRE group and a control group.
Footnotes
Author Disclosure Statement
No competing financial interests exist.