
Abstract
Introduction
Many therapeutic options have been suggested for the treatment of vitiligo, including nonsurgical and surgical modalities, most of them directed toward increasing melanocyte melanin production, and fewer addressing the immunologic nature of the disease. 4
Surgical modalities, such as autologous transplantation (split-thickness epidermal grafting, epidermal blister grafting, and grafting of cultured of melanocytes) are invasive and not well accepted by most of the patients. Nonsurgical modalities, considered the first line therapy, include topical, intra-lesional, and systemic corticosteroids, topical and oral psoralen plus ultraviolet A (PUVA), topical khellin 3–5%, broad band and narrow band (NB-UVB 311 nm UVB phototherapy), and, more recently, topical immunomodulators (i.e., tacrolimus, pimecrolimus). 4 –8
A validated and novel therapeutic option is represented by monochromatic excimer light (MEL) Micro, which is a 308-nm XeCl device capable of emitting a power density of 50 mW/cm2 on a maximum irradiated area of 30 cm2 (from 0.8 to 30 cm2). 8
A novel localized treatment of vitiligo is represented by the application of topical immunomodulators (TIMs). Tacrolimus modulates the immune system by inhibiting T-cell activation via downregulation of the transcription genes encoding pro-inflammatory cytokines (IL-2, IL-3, IL-4, IL-5, interferon-γ, tumor necrosis factor-α, granulocyte-macrophage colony stimulating factor). 9 –11 Some authors have highlighted the possible synergistic activity of topical tacrolimus plus UVB phototherapy, with either NB-UVB or excimer radiation through the activation of pathways influencing the process of melanocyte mitogenesis, melanocyte migration, and melanogenesis. 12 –14
The aim of this prospective, controlled, randomized, pilot study was to evaluate the efficacy and safety of the association of 0.1% tacrolimus ointment plus the 308-nm excimer light compared with 308-nm excimer light monotherapy in the treatment of vitiligo.
Patients and Methods
The study was approved by the “Policlinico Tor Vergata” ethical committee. All patients enrolled in the study provided written informed consent.
Fifty-three patients (27 male and 26 female), aged between 13 and 56 years (mean age 28 years), affected by localized and generalized vitiligo (acrofacial and segmental type) were enrolled in this open pilot prospective study. Those with vitiliginous patches ≥2 cm2 that had been stable over the last 6 months were randomly selected for treatment, and one to three symmetrical patches were irradiated.
MEL Micro (MEL, Excilite®μ DEKA Medical Lasers, Florence, Italy) is a 308-nm XeCl device capable of emitting a power density of 50 mW/cm2 on a variable area from 0.8 to 30 cm2, in order to concentrate treatment only on affected skin.
Patients were randomly divided into three groups: (1) Group I (MEL + vitamin E) included 20 patients treated with MEL Micro 308 twice a week and oral vitamin E 400 IU twice a day; (2) Group II (MEL + 0.1% tacrolimus + vitamin E) included 20 patients treated with MEL Micro 308 twice a week, 0.1% tacrolimus ointment once a day, and oral vitamin E 400 UI twice a day; and (3) Group III (Vitamin E - control group) included 13 patients treated with oral vitamin E 400 UI twice a day.
Exclusion criteria included: topical or systemic treatments and phototherapy during the previous 3 months, photosensitivity, photomediated disorders, radiotherapy, systemic immunosuppressive treatments, immunosuppressive diseases, history of skin cancer, pregnant and breast-feeding women, and age <10 years.
Group I and II patients were phototested with MEL on normally pigmented and unexposed skin. The minimal erythemal dose (MED) was determined at increasing light dosages following the initial dose of MEL, which was calculated according to patient's skin type (Table 1).
An initial dose of 75% of the MED reported for MEL was applied and increased at subsequent treatments by 0.25–0.75 J/cm2 of the dose used in the previous session, according to the erythematous response. The peripheral area of each single patch was protected from irradiation with a topical sunscreen applied 1 h prior to treatment. During therapy, when marked erythema occurred, the next dose was reduced by 25% of the previous dose.
Tacrolimus 0.1% ointment (Protopic®, Astellas) was topically administered once daily on single patches of patients included in Group II. Patients continued application of tacrolimus 0.1% regardless of phototherapeutic erythematous reaction. Minimizing or avoiding natural or artificial sunlight exposure during tacrolimus ointment treatment was recommended.
Two oral daily vitamin E capsules (Sursum® 400 UI, Abiogen) were prescribed to all patients for the whole period of the study, according to the role of oxidative stress in several cutaneous diseases including vitiligo. 15
During the pre-treatment visit and after 12 weeks of therapy, patients were assessed by physical examination, photographic documentation, and monitoring of adverse events.
Assessment of treatment efficacy performed by two independent physicians was based on the percentage of repigmentation in the treated area. Repigmentation was assessed in four categories: “no changes–poor repigmentation” (=25%), “moderate repigmentation” (25–50%), “good repigmentation”(51–75%), and “excellent repigmentation” (76–100%), as reported by various authors. 8,16
Safety assessments, including adverse events and vital signs, were assessed throughout the study and spanned a period through 120 days after the last treatment.
Statistical analysis
The significance of difference between percentages in groups was evaluated with the χ2 test. A p value of <0.05 was considered to indicate statistical significance. Statistical analyses were performed using SPSS for Windows (version 15.0).
Results
All patients treated with excimer light monotherapy or in combination with tacrolimus 0.1% completed the 12 weeks of treatment whereas in the control group, one patient discontinued the study after 3 weeks. Clinical features of treated patients are reported in Table 2.
Patients had a Fitzpatrick skin phototype ranging from II to IV. Considering each study group, the results were as follows: (1) Group I (MEL + vitamin E) showed moderate repigmentation in 7/20 (35%) patients, good repigmentation in 6/20 (30%) patients, excellent repigmentation in 5/20 (25%) patients, and poor repigmentation in 2/20 (10%) patients; (2) Group II (MEL + tacrolimus 0.1% + vitamin E) presented moderate repigmentation in 5/20 (25%) patients, good repigmentation in 8/20 (40%) patients, excellent repigmentation (Fig. 1) in 6/20 (30%) patients, and poor repigmentation in 1/20 (5%) patients; (3) Group III (vitamin E) showed a moderate repigmentation in 2/13 (16%) patients, 10/13 (76%) patients did not show signs of repigmentation and 1 patient 1/13 (8%) discontinued the treatment because of lack of efficacy.

Percentage of repigmentation was significant higher in Groups I and II than in Group III (p<0.001). Clinical response between Group I and Group II did not show statistical significance (p=0.36) (Fig. 2).
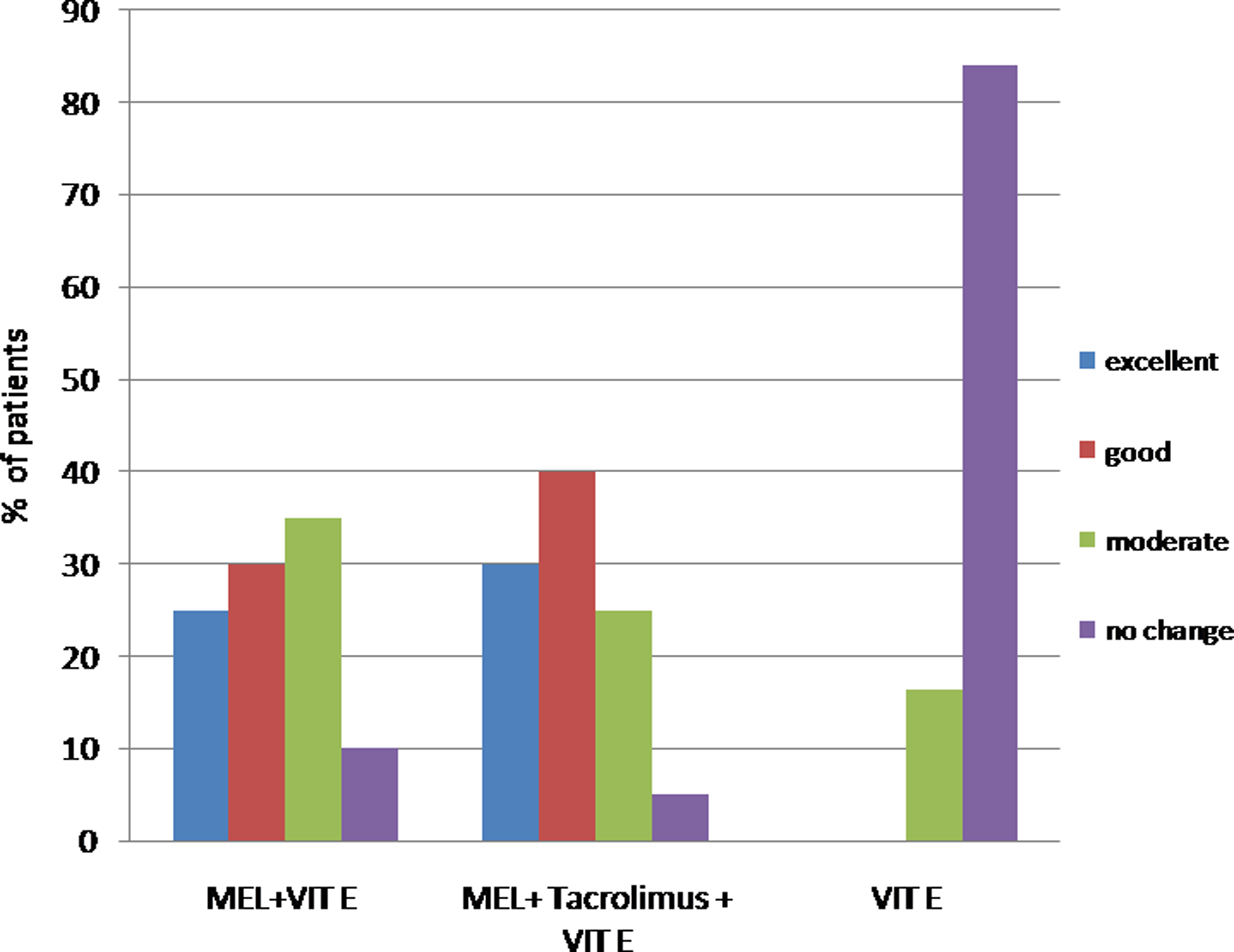
The chart shows the percentage of patients achieving an excellent, good, moderate, or no/poor repigmentation in the three treatment groups (Group I: MEL + vitamin E, Group II: MEL + 0.1% tacrolimus + vitamin E, Group III: vitamin E). The percentage of excellent–good repigmentation rate was higher in Group II than in Group I. Both clinical responses were significant compared to the control group (p<0.001).
The mean total dose at the end of treatment was 19.3 and 21.7 J/cm2 in Groups I and II, respectively.
No side effects, such as burning and blistering, were observed in any of the patients treated, although mild side effects were observed such as symptomatic erythema, burning/pain, stinging, and peri-lesional hyperpigmentation in 30% of patients and 25% of patients in Groups I and II, respectively.
Treatments were well tolerated, and at the 120-day follow-up visit adverse events related to therapies were not reported.
Discussion
Our results demonstrate that the combined treatment of 308-nm excimer light and 0.1% tacrolimus ointment (MEL+tacrolimus 0.1% + vitamin E) proved more effective than either MEL+vitamin E or vitamin E alone. It is noteworthy that good–excellent repigmentation was observed in 70% of patients treated with the combination of tacrolimus and MEL and in 55% of the MEL monotherapy group.
Among therapeutic options suggested for the treatment of vitiligo, phototherapy is considered safe and effective. 4 Furthermore, both excimer lasers and light sources showed a more rapid onset of repigmentation, less frequent applications, and possibility of a selective irradiation of vitiligo patches without a perilesional skin involvement. 16,17
However, our clinical experience in the treatment of vitiligo suggests that no treatment provides satisfactory results in all patients. For this reason, we believe that combined therapies could be a novel option in the treatment of vitiligo, as the synergistic action of different treatments could induce better results, minimizing adverse events.
We have previously showed, in an open pilot study, that the efficacy of excimer light can be enhanced by combination with the photosensitizer khellin. We found that this combination improved the percentage of repigmentation and rate of clinical response in resistant anatomical sites. 18
Similarly, we hypothesize that in a cutaneous immunomediated disorder such as vitiligo, the use of TIMs could enhance the effect of phototherapy, inducing faster repigmentation with long-term results. Evidence of this possible mechanism of action comes from the study of Castanedo-Cazares et al., 13 showing that after 6 months of traditional NB UVB phototherapy, an additional 3 months' application of tacrolimus 0.1% induced a further 25% improvement in repigmentation.
The association of phototherapies with TIMs in the treatment of vitiligo has been reported by other authors. 14,19,20 Passeron et al. 19 reported, in a controlled study performed in 14 patients, that the combination treatment of 0.1% tacrolimus ointment plus 308-nm excimer laser was more effective than 308-nm excimer laser as a monotherapy and controls, for achieving a repigmentation rate of at least 75%.
In another pilot study, 12 it was reported that of the 24 vitiliginous patches treated with excimer laser 308 nm, in combination with tacrolimus 0.1% ointment, 50% achieved a successful response (75% repigmentation) at a significantly faster rate than that of other vitiliginous patches treated with excimer laser and placebo, which achieved only 20% success.
Similar to the aforementioned studies, we reported a good–excellent repigmentation in 70% of patients treated with the combination of MEL and tacrolimus, whereas in the MEL monotherapy treated group, we observed a good–excellent repigmentation only in 55% of patients. Moreover, we found that the onset of repigmentation occurred after a mean of 11 and 9 sessions, respectively, in Groups I and II. This was in accordance with the mean total dose: the mean cumulative dose of MEL was higher in Group II than in Group I, suggesting that tacrolimus increased the tolerability to phototherapy through an immunomodulator mechanism. As a consequence, the higher percentage of clinical response observed in Group II compared to Group I could be caused by both the higher cumulative dose and the immunodulatory effect of tacrolimus.
The rapid efficacy and the total number of applications confirmed previous observations reported by Passeron et al. 19 In contrast to the latter, we reported the efficacy and the rapid mechanism of action of the combined therapy in a larger group of patients. Furthermore, the safety was assessed through a long-term follow-up of 120 days.
The association of excimer light phototherapy and tacrolimus ointment offered encouraging results in terms of patient compliance with the given therapeutic protocol, as it was well tolerated, not time consuming, and easy to administer. Furthermore, even if it was not reported in this study, patients noted a significant improvement of their quality of life, less embarrassment during relationships, improvement of their body image, and a more optimistic attitude towards life and their disease when treatment was effective (data not shown). These findings were not reported in patients affected with localized vitiligo, who showed a poor response to medical treatment in all groups.
The use of a TIM in association with phototherapy gives rise to concerns about the possible increased risk of skin carcinogenesis. 20 On the other hand, results of a recent study suggest that topical calcineurin inhibitors do not affect the clearance of DNA photoproducts preventing DNA photodamage, because of a filter effect of both vehicle and active components. 21 Moreover, as previously discussed, the use of tacrolimus may be useful to prevent UVB-induced erythema by inhibiting early-phase events of the inflammatory process. 12 –14
Finally, addition of tacrolimus to excimer phototherapy could be another option for vitiligo patients, considering the lower cancerogenesis profile compared with systemic administration, and the quicker repigmentation effect.
In conclusion, our results confirm the efficacy of excimer light therapy in vitiligo as reported by other authors, 8,17 and suggest that an association with TIMs such as tacrolimus, which address the immunologic nature of the disease, could enhance the clinical response, especially in more resistant anatomical sites, without an increase in side effects.
Therefore, combination of UV light and TIMs may represent an advance in the treatment of the disease.
Conclusions
Our results confirm the efficacy of excimer light therapy in vitiligo, suggesting that an association with TIMs may represent an advance in the treatment of the disease. Furthermore, this study suggests that an association with TIMs could enhance the clinical response in vitiligo, especially in more resistant anatomical sites, without an increase in side effects. Indeed, this combination could enhance the clinical response interfering with immunological pathways involved in the pathogenesis of the disease. However, further studies are mandatory in order to identify therapeutic protocols and a long-term safety profile according to phototype and vitiligo phenotype.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist