
Abstract
Introduction
Combining with exogenous photosensitizer aminolevulinic acid (5-ALA), topical photodynamic therapy (PDT) can achieve targeted therapy by selectively treating abnormal skin tissues within a lesion area with the light at a specific wavelength. 2 For the thick wart tissues with extensive proliferation, the penetration of the light may not be enough; 3 therefore, a single local photodynamic therapy often shows poor efficacy. Therefore, to improve the treatment, from March 2008 to December 2010, for 40 cases of perianal CA, we tested the use of curettage to remove, first, thick proliferative wart tissues, and then used a subsequent local PDT for cure. Our study demonstrated a significant efficacy of this combined treatment.
Patients and Methods
In this study, 40 patients with perianal warts were recruited from the dermatology clinic in our hospital. There were 24 males and 16 females with an average age of (31.24±8.59) years. Each case had 5 to 25 lesions, and a total of 522 lesions were treated, at an average of (14.21±5.52) lesions per patient. Warts varied in size, but all had wide pedicle, smooth and moist surface, and clear boundary. Some were fused lesions. Most lesions were gray-brown in color, and a small number of warts appeared dark red. Twelve cases had diameter >4 cm. Fourteen patients had never received any prior treatment, whereas others had received repeated freezing, laser therapy, electrocautery, or/and other treatments for periods ranging from 2 months to 2 years. Four cases showed obvious scar formation. Patients with history of a photosensitivity; serious systemic diseases; severe immune deficiency or suppression; concurrent rectal, urethral and vaginal warts; infection of HIV; histologically proven intraepithelial neoplasia or cancer; and women who were pregnant or breast-feeding, were all excluded from the study.
The study protocol was reviewed and approved by Institutional Review Board of the hospital. All subjects signed informed consent forms for photodynamic therapy and allowed themselves to be photographed. They also agreed to the use of the photographs showing their body part with the lesions. All the eligible patients were informed of the principles, efficacy, potential complications, and side effects of PDT. In addition, they were informed of the potential benefit of curettage to the warts with marked hyperplasia, and the significance of the overall treatment plan.
For warts with obvious hyperplasia, local anesthesia was achieved by application of 2% lidocaine, and a curette scrape was used to remove the abnormal tissue of perianal CA. To avoid excessive damage to the perianal skin, curettage was limited to the size of the wart, and did not go beyond the base of the warts. After the procedure, the area was then treated with chlortetracycline eye ointment and iodophors gauze with appropriate pressure. Biopsies of the lesions were compatible with CA. Twelve hours later, the patients demibained in a bath of potassium permanganate solution. Topical photodynamic therapy was performed 2 days after curettage procedure. Fresh wounds were covered by cotton sheets soaked with 10% 5-ALA (Fudan Zhang Jiang Biomedical Corp., Shanghai, China) in an oil-in-water emulsion (containing 5% azone) for a 3-h incubation period under a light-shielding dressing. The laser beams of a 635-nm wavelength emitted by a diode laser type XD-635AB (manufactured by Xingda Photoelectricity Medical Equipment Corp., Guilin, China) were directed onto the therapy area at the same energy density (120 J/cm2) within an irradiated field of 3 cm2; power output was set to 177mW/cm2. The light direction was adjusted to keep a constant distance from lesions. Each therapy area was irradiated for 10 min. After the PDT, the perianal area was bathed in 1:5000 potassium permanganate solution for 30 min once a day, for a total of 3 days. During the recovery process, patients were advised to avoid scratching and intense activities. Later, the patients experienced another two periods of treatment at 1 week and 3 weeks. Before treatment and at each return visit, the lesions were photographed. At 1 and 3 months after three sessions, all patients were followed up for clinical evaluation, including lesion recurrence, encrustation, scab off, scar formation, skin pigmentation change, and tolerance to pain. At each visit, patients were surveyed for their satisfaction with the treatment results. Each patient was asked to select one of the three answers "very satisfactory”, “fairly satisfactory”, or “unsatisfactory".
Results
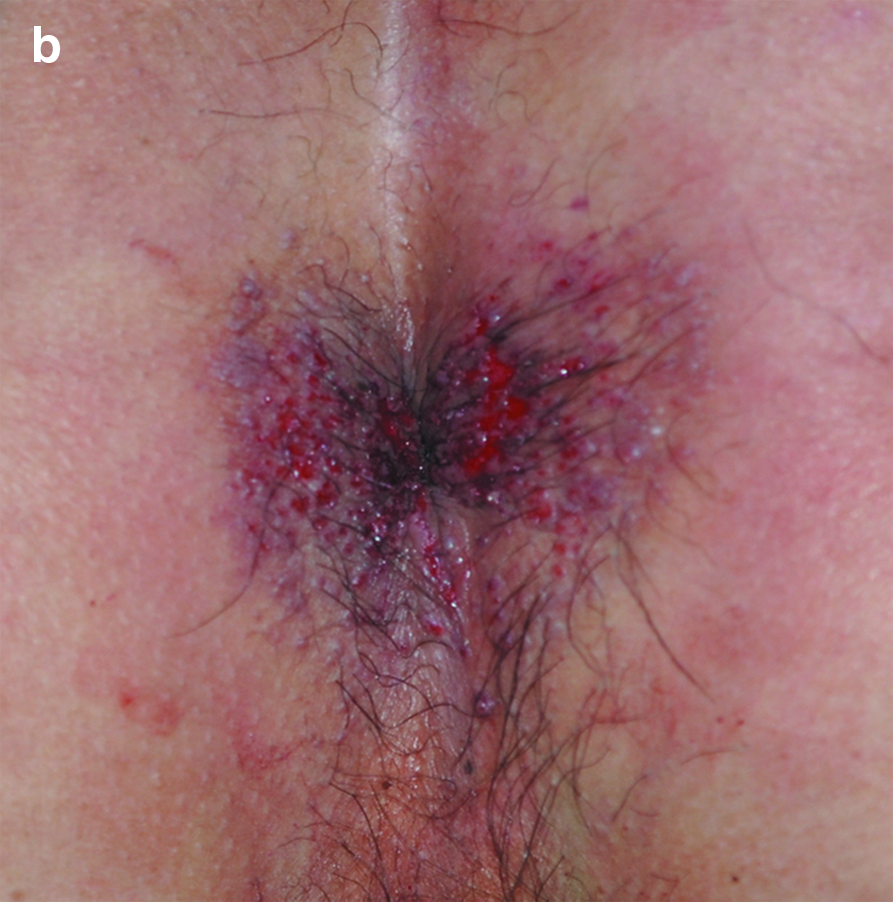
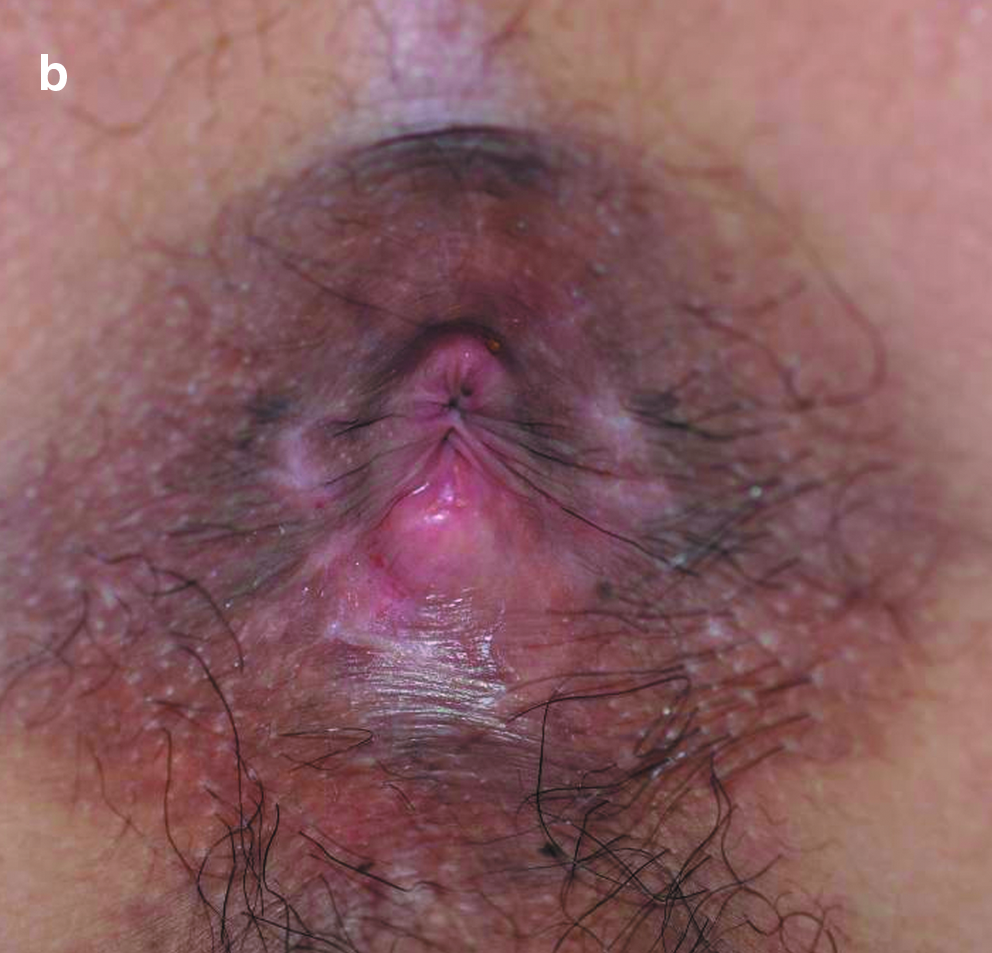
Two days after wart curettage followed by treatment with 5-ALA emulsion, the skin lesions were generally healed, and all patients presented with no discomfort except for mild-to-moderate pain. They all completed three PDT sessions. The perianal area had no visible warts after two topical PDT treatments. At the 1-month follow-up visit, no recurrence was identified (Figs. 1 –3); at 3 months, six cases of recurrence were identified, and the recurrence rate was 15%. This rate was still much lower than the rate of recurrence following other conventional treatment methods. These results were summarized in Table 1. In the course of treatment, all patients were able to follow the treatment protocol, and responded to the survey with 100% satisfaction at 1 month and 95% satisfaction at 3 months after completion of treatment.






After local wart curettage, obvious bleeding might occur but can be stopped easily after application of local pressure. Different degrees of edema and erythema occurred around the treatment area in some patients during laser irradiation, which was also accompanied by mild-to- moderate burning pain. All these symptoms were well tolerated, and all patients were able to successfully complete the laser treatment. Rupture of blisters in the treated area occurred in two patients. The lesion healed in 3 days after the recommended bathing treatment. These events did not affect the next PDT, and there was no depigmentation and scar formation.
Discussion
Genital warts are a highly recurrent sexually transmitted disease caused by HPV infection of keratinocytes. The anal area is humid, and at a high risk of relapse after treatment. This disease and its high relapse rate seriously affect the quality of life and treatment confidence of patients, as well as their family stability and welfare. 4 Traditional treatment such as freezing is often significantly associated with blisters and blood blisters. Superficial ulcers or erosion can occur as the result of friction, therefore affecting wound healing while promoting the virus inoculation and opportunities for wart recurrence. On the other hand, CO2 laser treatment can also result in ulcers if the depth of the radiation site is not well controlled, and scarring after healing can also provide shelters for the virus to grow and cause relapse. 5 In recent years, topical application of imiquimod has brought new hope to the treatment of genital warts, but its efficacy is not good for larger warts. 6
The histological feature of typical condyloma lesions is intra-epidermal abnormality, such as parakeratosis, hyperkeratosis, epidermal acanthosis, papilloma hyperplasia, and marked hyperplasia of basal cells. Vacuole-like cells appear in the granular layer and above the stratum spinosum. However, a majority of subclinical HPV infections only show focal epithelial hyperplasia by histology. 7 The latency of HPV infection is also an important factor contributing to the relapse of genital warts after treatment. To reduce the recurrence of perianal warts, we used local PDT, a new technology developed in recent years, which uses light excited at specific wavelengths to stimulate the photosensitive material of biological tissues; trigger a series of physical, chemical, and biological reactions of the body; and, ultimately, achieve selective treatment. 8 It can largely reduce the inevitable damage to the surrounding normal tissue that is the side effect of most traditional treatments.
As a biosynthetic precursor of heme, a hemoglobin prosthetic group, 5-ALA itself is not a photosensitizer. When penetrated into the skin, it can be absorbed by HPV-infected proliferating keratinocytes, and then converted to protoporphyrin IX (PpIX) via biological synthesis. 9,10 Because the activity of ferrous chelating enzyme in the actively proliferating cells is inhibited, the synthesis of PpIX into heme is reduced, and ultimately PpIX accumulates in a typical wart tissue, or HPV-infected subclinical and latent tissues at a higher specificity. 7,10,11 As a potent photosensitizer, PpIX generates a large number of singlet oxygen and some reactive oxygen species under light irradiation at a certain wavelength by the photosensitizing effect, 8,12 and then causes the desired damages to overly proliferative cells, and eventually achieve a targeted therapeutic effect.
The light source used in this study emitted at a wavelength of 635 nm, which penetrates to an effective depth of ∼ 6 mm. 13 Although the safety of the treatment is ensured, the depth of PDT treatment is limited by the depth of penetration and the restriction of photosensitive reaction, which is not sufficient for CA with significant proliferation. Therefore, removal of perianal warts by curettage significantly improved the treatment effect, particularly to the giant condyloma. The curettage procedure did not result in the occurrence of ulcers or scars, and can significantly clear the obstacles for the follow-up treatment.
HPV infection has an epidermal tropism, and generally condyloma tissues are limited to the epidermis. Therefore, well-operated curettage surgery can be limited to the epidermis and not damage dermal tissues; therefore, the wound at the wart site can be healed 2 days after curettage to allow the subsequent PDT. This greatly shortens the treatment time and is beneficial for recovery. The removal of proliferation warts provides a pathway for the laser to penetrate deeper into the skin layer and enhance the treatment efficacy. This practice is consistent with the required depth of 2–3 mm to eliminate superficial skin lesions, cited in the literature. 3,14 Therefore, among the cases we observed, all warts disappeared after three treatments, and there was no recurrence at 1 month. During the course of treatment, the intact skin area after treatment often shows more obvious erythema, swelling, or even blisters. However, the skin lesions after curettage show less significant swelling. This observation may be explained by the fact that fresh wound skin contains only a thin stratum corneum, so the resistance to exogenous photosensitizer permeation is reduced and the drug is more concentrated. This allows for specific distribution of the drug and improvement of photodynamic therapy, and also for a correspondingly lower incidence of side effects.
Because of the selective treatment to the typical CA by HPV infection, and the clearance of subclinical lesions and latent infection, local PDT shows an effectiveness and relapse rate superior to many traditional treatments. 1,5,15 The recurrence rate was only 15% in the 3 month follow-up period. In this study, the curettage surgery to the highly proliferative warts greatly compensated for the limitations of local PDT treatment, and improved the treatment of perianal CA by extending the depth of treatment. Among six cases of recurrence, four patients had scar tissues from prior treatment, one patient was an alcoholic, and one had long-term depression.
Because of the selectivity of PDT and the prevention of dermal tissue damage, no ulcers or scars occurred in any of the 40 cases, further confirming the safety of this combination therapy. 16 With the excellent outcome and safety, 95% patient satisfaction rate was achieved at 3 months after treatment.
Conclusions
Through the operation, obvious hyperplasia was cut off, and time to cure was markedly decreased. After curettage, the clean lesion afforded an ideal circumstance for PDT. Topical PDT could eliminate the subclinical infection of HPV and decrease the rate of recurrence. Therefore, the combined treatment was proven to be a safe and effective procedure in perianal CA, especially in large warts. It was demonstrated that topical ALA-PDT combined with curettage could offer a wide clinical application for the treatment of perianal CA.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.