
Abstract
Introduction
In an attempt to search for alternatives to reduce or even prevent tissue necrosis, studies are being conducted using experimental models with the application of different kinds of drugs such as vasodilators, anticoagulants, antioxidants, prostaglandin inhibitors, calcium channel blockers, and antiadrenergic agents. 5 –7 The use of some of these drugs, however, involves undesired systemic effects, with a consequent increasing demand for nonpharmacologic sources such as acupuncture and electroacupuncture, 8 low-level laser therapy (LLLT), 9 –13 and polarized low frequency electric current. 14
The use of LLLT has become an essential tool to increase flap survival and safety because of its easy application, and suitable and encouraging results at both the macroscopic and cellular levels. 15 –19 Low level laser therapy is a therapeutic treatment able to increase blood flow and to promote angiogenesis, being widely used to accelerate wound healing. 20
As a result of these effects, the efficiency of low level laser therapy in improving skin flap survival started to be investigated. Many authors have demonstrated that the diode laser may improve flap survival by both eliciting proliferation of new blood vessels around the irradiated sites and increasing reperfusion. 9 –13 However, the literature points out several discrepancies in terms of laser parameters, especially those regarding the ideal wavelength. Therefore, we aimed to find out which wavelength was the most effective in treating ischemic flaps, as well as to investigate the effect of 830 and 670 nm diode lasers on vascular endothelium growth factor (VEGF) and epidermal cell proliferation index (KiD67) in random skin flap survival.
Materials and Methods
The study was approved by the Research Ethics Committee of the University of São Paulo (FMRP-USP) according to the current legislation.
Thirty adult male albino Wistar rats (Rattus norvegicus) weighing 260–320 g were used. After the laser therapy sessions, the animals were housed in their respective cages, with temperatures between 22 and 27°C on a 12/12 h light–dark cycle and maintained on commercial ration and water ad libitum.
Equipment
The diode laser equipment used in this study was from Ibramed® Equipamentos Médicos (Amparo - Brazil) (Table 1). The equipment was calibrated in the Physics Department, University of São Paulo (USP). Before each application, the calibrator was adjusted. Radiant power was determined by attaching the extremity of the laser diode to a Lasercheck® digital potency analyzer (Coherent®, Staunton, VA) sensor at a 90 degree angle, calibrated, and used according to the manufacturer's instructions. Three consecutive measurements were performed and the mean value was used.
Groups and experimental protocol
Laser irradiation was performed immediately after surgery and for 4 consecutive days, always at the same time of day. Irradiation was applied through a punctual contact for 72 sec per session, with the probe being positioned perpendicular to the skin flap. The site of the laser application was located at 2.5 cm distal from the cranial base of the skin flap 13 (Fig. 1).
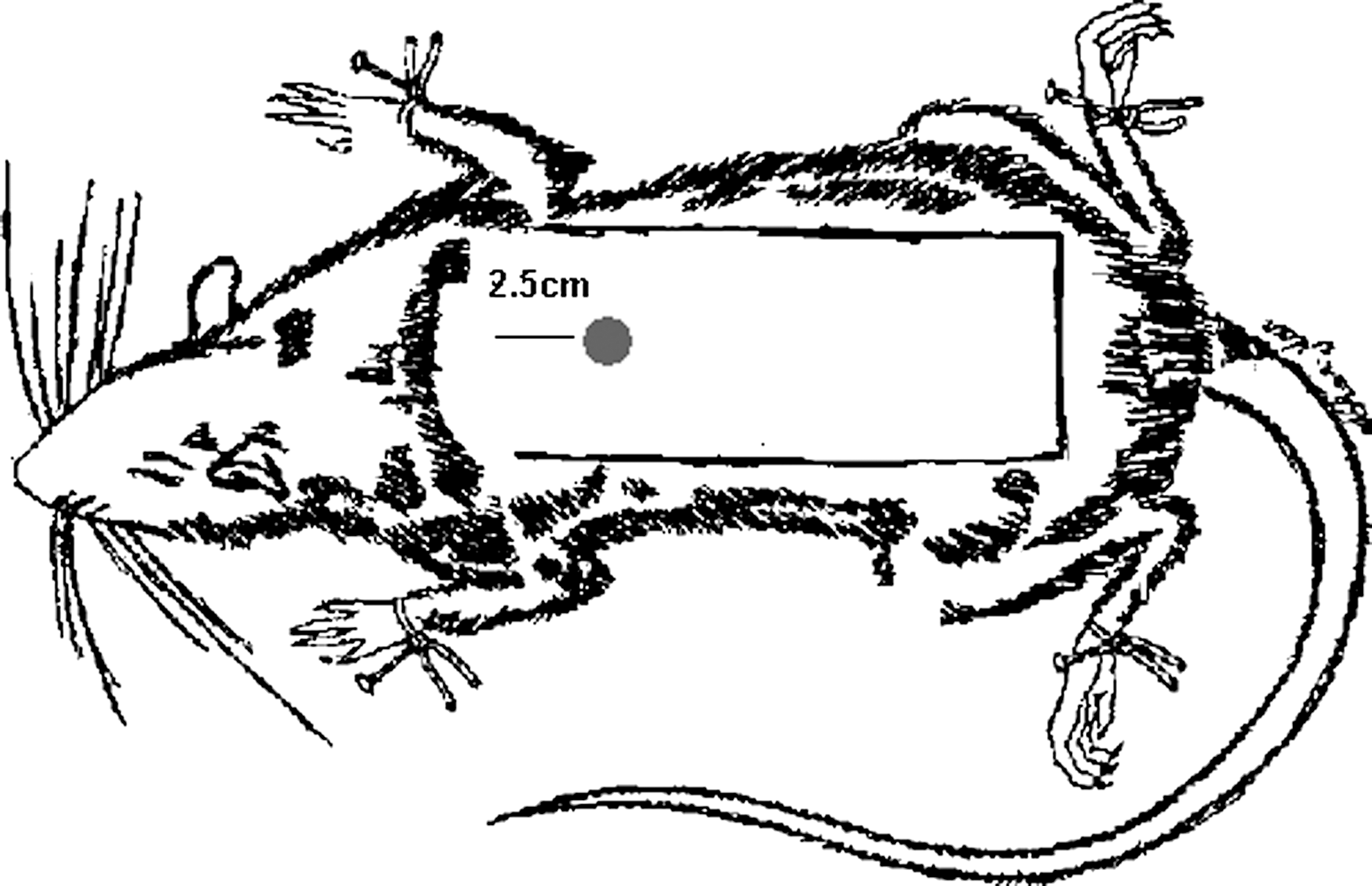
Irradiation site.
All 30 rats were weighed and randomly divided into three groups of 10 animals each. The number of animals in each group was determined by means of statistical planning. Group 1 (control) underwent sham irradiation, group 2 was subjected to diode laser irradiation at 830 nm, and group 3 was treated with diode laser irradiation at 670 nm. For the experimental groups, the energy density (dosimetry) was set at 36 J/cm2 (total energy=2.52 J).
Surgical technique
The animals were anesthetized with an intraperitoneal injection of an even mixture of tiletamine and zolazepam (50 mg/kg), remaining anesthetized during surgery and the laser sessions. Following anesthesia, the rats were positioned on a flat surface with limbs extended, and a digital trichotomy was performed on their back. The skin flap was anatomically planned on the animals' back by using a 10 cm long and 4 cm wide plastic template. The inferior angles of the scapulae and the ilium of the pelvis served as reference. The flap was elevated in a caudocranial direction and included the deep and superficial fasciae, the panniculus carnosus, and the skin. 21 A plastic sheet (10×4 cm) was placed between the flap and the donor site. 22,23 The flap was then sutured in the original position using 4-0 monofilament nylon thread with simple stitches separated 1 cm from each other. 21
Immediately after the surgical procedure, group 1 (sham) and both experimental groups were kept anesthetized for another 30 min, when they received the diode laser radiation at the same time.
On the 7th postoperative day, the animals were anesthetized and the percentages of their necrosis area were calculated through the paper template method. 24 A skin sample was collected to perform an immunohistochemical analysis of the endothelial vessels with the VEGF marker and the epidermal cell proliferation with the Ki-67 marker.
A pachymeter was used in order to standardize the sample collection, with a 1 cm2 sample being removed 2.5 cm distal from the cranial base of the skin flap and 2 cm from the lateral margins (laser irradiation site). Immediately after, euthanasia was performed by excessive inhalation of diethyl ether.
Method for estimating percent necrotic area in the distal portion of the flaps
The limit between viable tissue characterized by soft, reddish, warm, and hairy skin; and necrotic tissue by stiff, dark, cool, and hairless skin was demarcated in the animals.
24
A mold of the entire flap and the necrotic area was drawn and cut in transparent paper, being checked in a precision scale (+/− 0.001 g error). The following equation was then used:
Morphometry for the evaluation of VEGF and Ki-67
Slides were read with a light microscope (Olympus BH-2 brand) with a 10× ocular lens and a 40× objective, producing a 400× magnification. The quantitative study was performed using an ocular lens with 10× magnification and a small quadriculated grid. The grid consisted of 100 squares measuring 0.25 mm on each side and was adapted to the light microscope. Only the cells immunopositive to the Ki-67 marker and the blood vessels expressing VEGF, which were inside the quadricules and were not superposed by their lines, were counted. For the morphometric reading, a total of 10 fields were observed on each slide. The mean value of the immunopositive cells and of the vessels expressing VEGF per slide was measured. These measures were done by a blinded researcher.
Statistical analysis
Analysis of variance (ANOVA) was used to determine possible significant differences between groups regarding the percentage of necrosis, VEGF, and Ki-67,
The Pearson correlation coefficient was calculated to determine whether a statistically significant relationship existed among the percentage of necrosis, VEGF, and Ki-67 values. The level of significance was defined as 0.05, in a bilateral test for all analyses.
Results
The percentage of necrotic area was: group 1 (48.04%), group 2 (33.60%), and group 3 (30.22%). The experimental groups (groups 2 and 3) showed statistically significant differences when compared with group 1 (p<0.01) in terms of necrosis percentage, with the highest values being observed in group 1. Groups 2 and 3 did not differ significantly from one another (p>0.05) when the paper template method was used (Fig. 2).
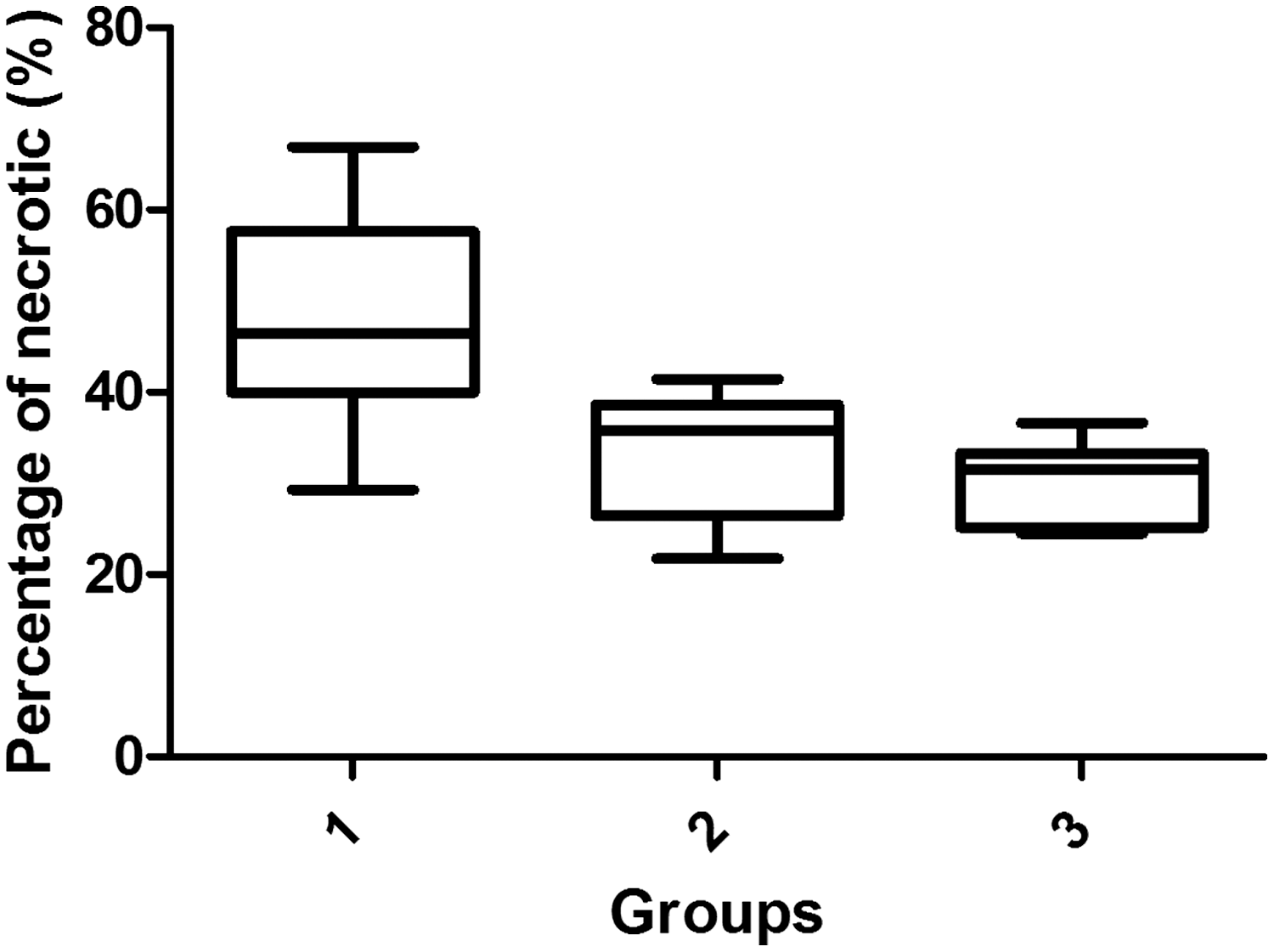
Percentage of necrotic area obtained through the paper template method.
In the present study, the mean number of vessels expressing VEGF for each group was: group 1 (1.87), group 2 (4.34), and group 3 (6.62). The experimental groups (2 and 3) showed a statistically significant increase in VEGF when compared with the control group (Fig. 3). There was also a statistically significant difference between groups 2 and 3, with group 3 presenting higher values of vessels expressing VEGF (Fig. 4).
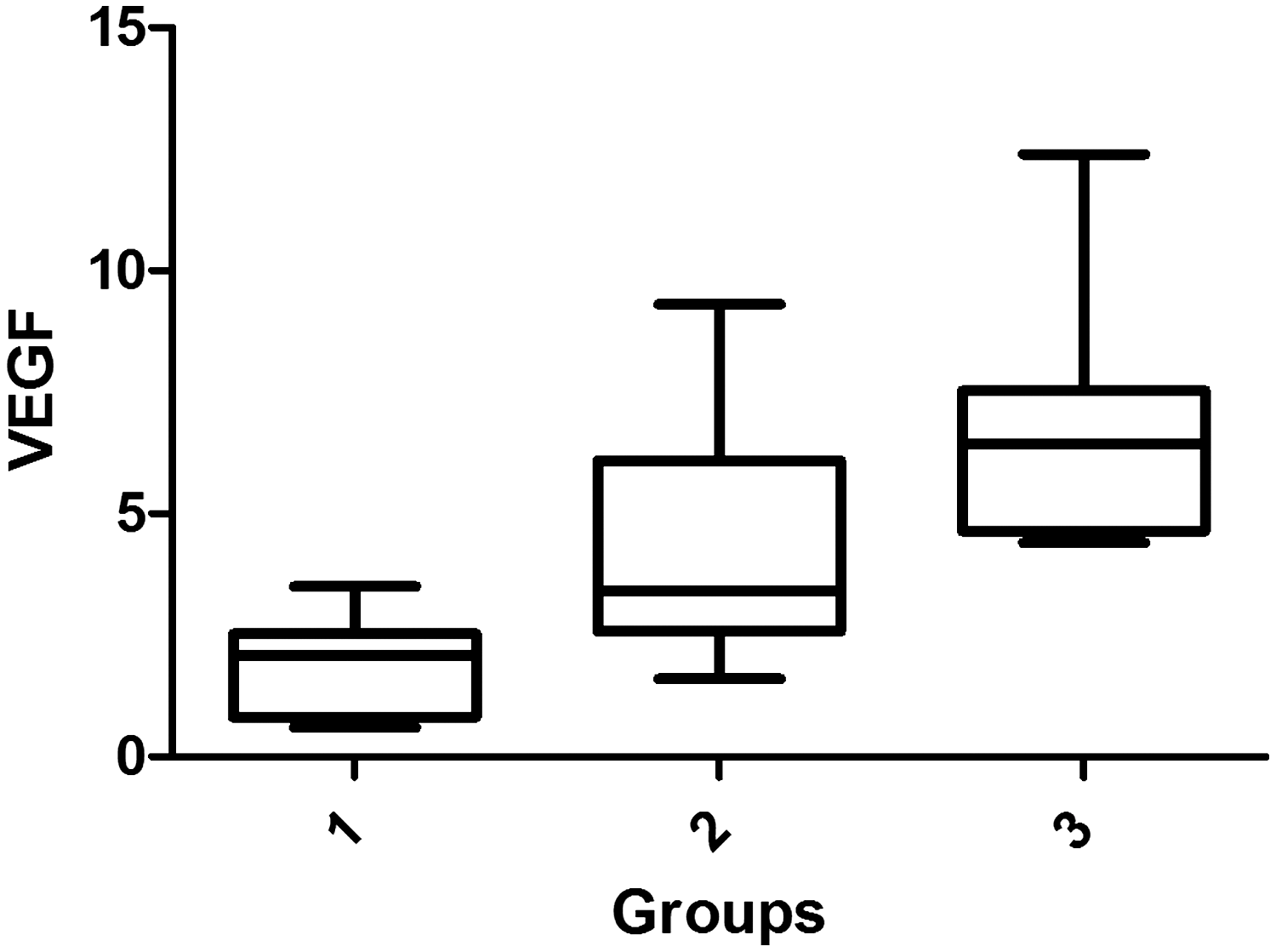
Blood vessels expressing vascular endothelial growth factor (VEGF).
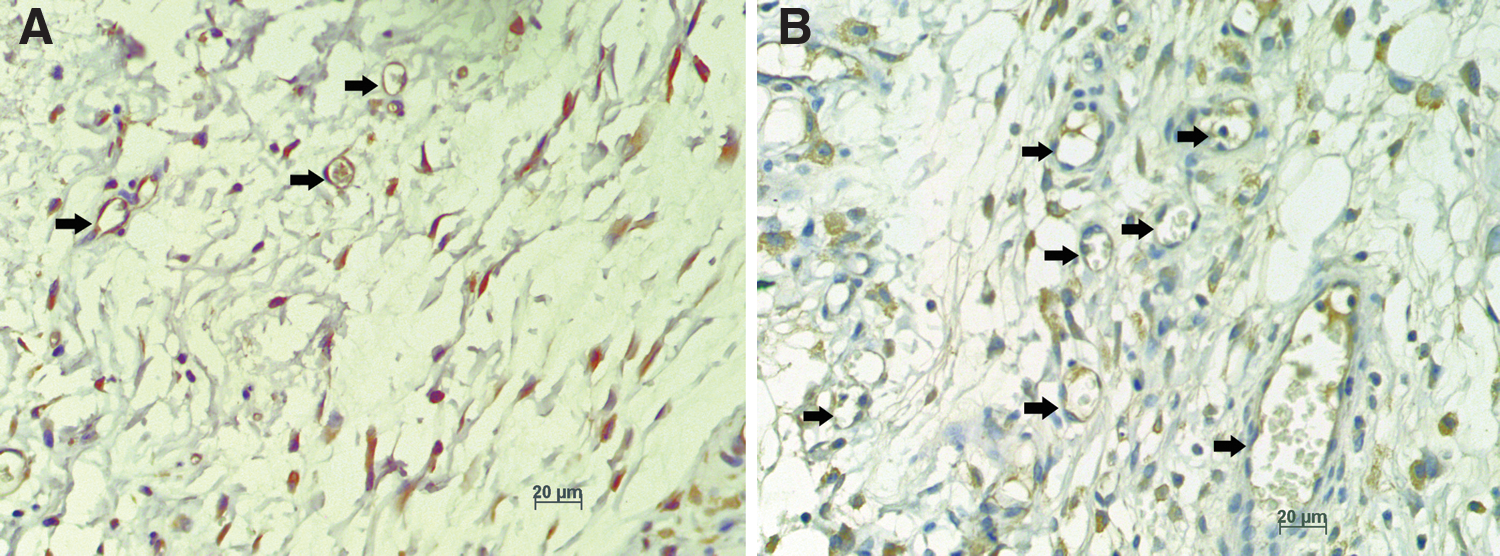
Immunohistochemical analysis (IHQ) – vascular endothelial growth factor (VEGF) with 400× magnification.
Pearson's linear correlation test between necrosis percentage and number of blood vessels expressing VEGF showed a correlation coefficient of −08.82 (p<0.01). Therefore, the variables expressed were negatively and strongly correlated, that is, the higher the percentage of the necrosis area, the lower the amount of blood vessels expressing VEGF found in the flap, and vice versa.
In the present study, the mean number of cell proliferative activity in the epidermis basal layer for each group was: group 1 (0.34), group 2 (3.53), and group 3 (4.58). The proliferative activity measured by the Ki-67 marker was significant, showing higher cell proliferative activity in the epidermis basal layer in the group irradiated with low level laser (groups 2 and 3) compared with control (p<0.01) (Fig. 5). In addition, proliferative activity was significantly higher in group 3 (p=0.04) compared with group 2 (Fig. 6).
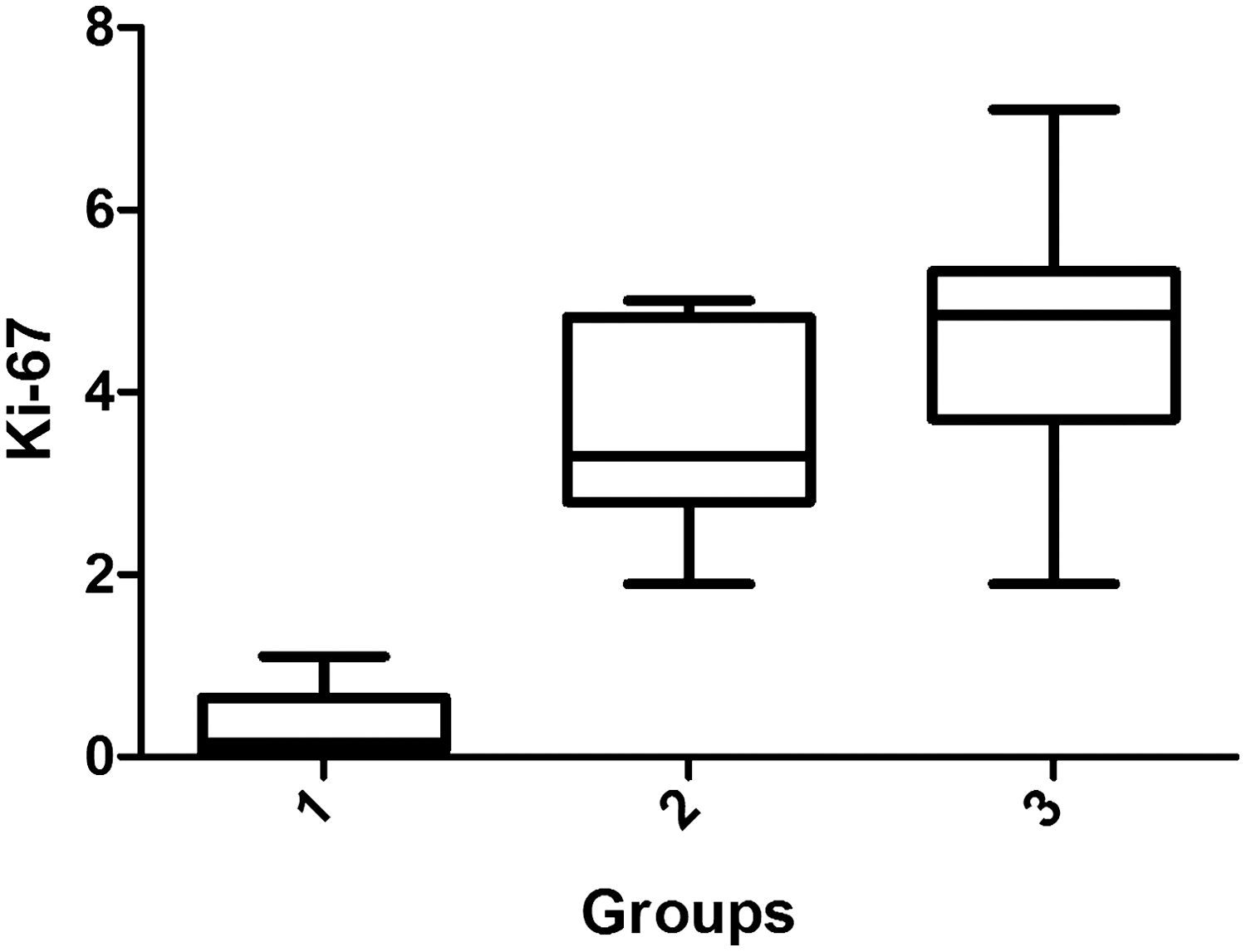
Epidermal cell proliferation index (KiD67).
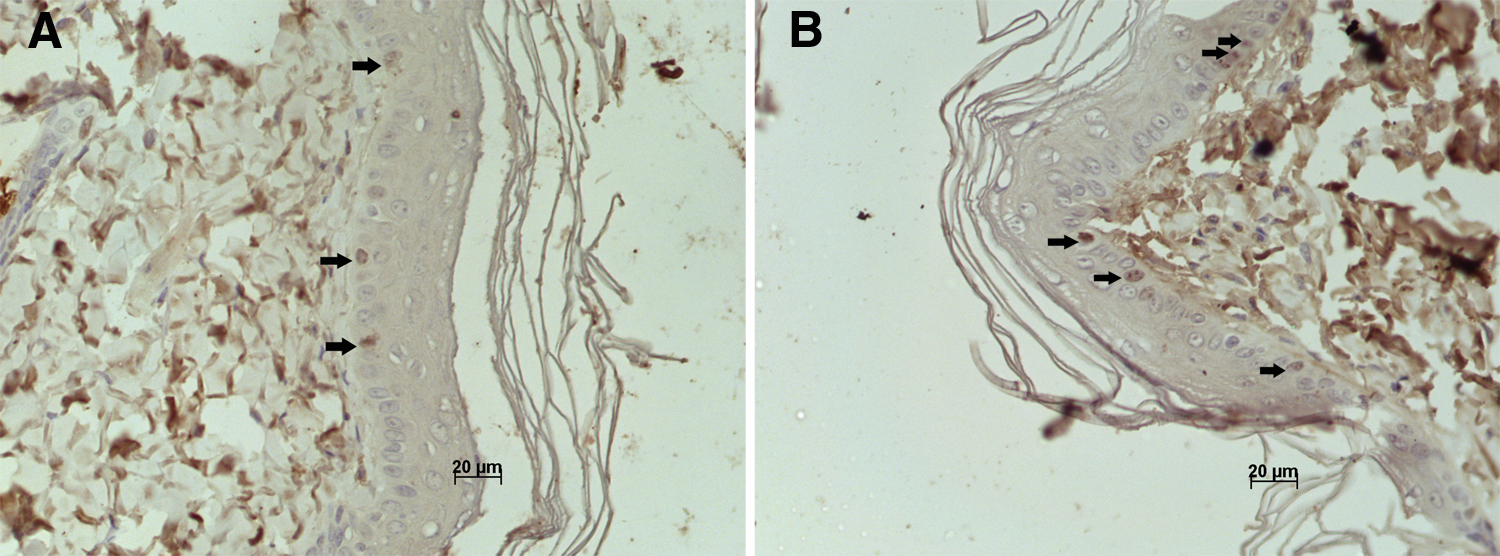
Lamina IHQ – Ki-67 with 400× magnification.
Pearson's correlation test showed that the higher the percentage of the necrosis area, the lower the amount of cells in the proliferative phase found in the flap, and vice versa.
Discussion
LLLT was first used to speed the healing process of ulcers of several etiologies. In this respect, several studies demonstrated many mechanisms of action for LLLT such as angiogenesis induction, blood flow increase, collagen synthesis, fibroblast proliferation, and activation of superoxide-dismutase (SOD) delivery. 25 –28 Based on this knowledge, we decided to investigate the effects of this blood flow increase promoted by laser irradiation, on the viability of ischemic random skin flaps.
Some literature reports have shown the efficacy of LLLT regarding skin flap viability, as is also shown by the results obtained in the present study. 9 –13,17,19 However, there is wide a discrepancy in terms of parameter standardization for the application of LLLT, making it difficult to compare results and interpret some of its mechanisms of action.
It has been reported that the efficacy of LLLT depends upon some variables such as wavelength, power, energy density, power density, transverse section of the transmitter beam area, total energy issued, application technique, and treatment frequency. 16,26,27
Only two trials have evaluated the action of 670 nm laser on the viability of random skin flaps in rats. Assis et al. 17 compared lasers with wavelengths of 670 nm (power 30 mW) and 904 nm (power 15 mW) in terms of random skin flap viability in rats. However, the same energy density was used (16 J/cm2) for the two types of lasers. A significant decrease occurred in the necrosis area of irradiated groups when compared with the control group; however, the laser with a wavelength of 670 nm operating with 30 mW power was more effective than the laser with a wavelength of 904 nm, with 15 mW power. Bossini et al. 29 studied the 670 nm laser using energy densities of 3, 6, 12, and 24 J/cm2, and concluded that all experimental groups had statistically significant values compared with control, and that the one treated with the energy density of 24J/cm2 had the smallest area of necrosis.
These studies are contradictory regarding some variables, such as the number of irradiated points, the amount of application of laser radiation, and the flows used. Assis et al. 17 applied radiation to just one point located at 2.5 cm away from the flap base for 5 consecutive days. In the study by Bossini et al., 29 the application of laser radiation was spread over 24 points distributed on and around the flap, based on the study by Pinfildi et al. 18 who had obtained a smaller necrosis area when the laser was applied on and around the random cutaneous flap in rats.
Regarding laser with a wavelength of 830 nm, only four publications have evaluated the action of laser on viability of random flap in rats, 9,11,30,31 but these also showed contradictions with regard to some variables. Kami et al. 9 used equipment with power of 15 mW, beam area of 0.02 cm2 and energy density of 16 J/cm2. Kubota and Ohshiro 11 used a laser with power of 60 mW, wavelength of 830 nm, and energy density of 36J/cm2, but the beam area was not mentioned.
Kubota 30 used laser with power of 100 mW, beam area of 0.0054 cm2 and energy density of 185 J/cm2 and, despite this very high dose, they observed a statistically significant outcome. Prado et al. 31 used equipment with power of 30 mW, flow of 36 J/cm2 and irradiation beam area of 0.06 cm2, with a continuous beam. Despite the differences in equipment, all authors were able to obtain significant results.
Based on this, the purpose of the present study was to compare lasers with wavelengths of 670 and 830 nm using the same number of irradiated points, the same power, energy density, area of the transverse section of the beam, total energy issued, application technique, and treatment frequency. The results showed that there was no statistically significant difference in percentage decrease of the necrosis area between the two wavelengths, although both lasers induced a significant reduction when compared with control.
To study necrosis and its prevention, a random dorsal cutaneous flap from the cranial base was used as the experimental model, as proposed by McFarlane et al. 21 In this model, a flap measuring 10 cm long×4 cm wide generally presents a necrosis percentage between 25 and 50% from its distal portion. To assure and standardize the degree of flap ischemia, a plastic film was placed between the flap and the donor bed to avoid flap revascularization from the bed vessels, as proposed by Ugland 22 and reviewed by Kaufman et al. 23 The percentage of flap necrosis area was evaluated on the 7th postsurgical day using the paper template method, as first described by Sasaki and Pang. 24 This method was used because it is quick and easy to perform, with an error of <5% and only a piece of translucent paper and a precision scale are necessary.
Based a study by Prado et al., 31 the experimental groups were irradiated for 5 consecutive days at the same time of day. To choose energy density, we reviewed studies investigating the effects of LLLT on cutaneous flaps and decided to use 36 J/cm2 based on the investigations by Kubota and Ohshiro 11 and Prado et al., 31 who reported that this dose was sufficient to reduce the area of flap necrosis. The application technique used was the punctual contact one, based on the studies by Kami et al., 9 Amir et al., 12 and Pinfildi et al. 18 According to some authors, the application allowing the contact of the laser source with the skin surface during irradiation increases the depth of penetration, because of the reduction of both reflection and energy dispersion. 9,11 –13
Following an experimental model for LLLT on random ischemic skin flap in rats proposed by Prado et al., 13 we applied laser radiation to a point located at 2.5 cm from the flap base in order to stimulate all its vessels, instead of stimulating angiogenesis in regions cut to lift the flap.
Literature reports have stated that LLLT can increase blood flow in the microcirculation, because it increases the release of nitric oxide, a powerful vasodilator, in the irradiated site. 28,32 Moreover, it may promote both delivery and secretion of angiogenesis-related growth factors, 20 thus allowing the supply of oxygen and suitable nutrients to meet the needs of the proliferative stage of the tissue repair process. 33 –36
In the present study, the experimental groups (2 and 3) showed a statistically significant increase of VEGF when compared with control, in agreement with the findings by Tuby et al., 33 who stimulated the hearts of animals submitted to a heart attack with LLLT and found a significant increase of VEGF that induced an important angiogenesis process. A statistically significant difference was also observed between groups 2 and 3. The group irradiated with 670 nm laser (group 3) presented the lowest mean percentage of tissue necrosis area and the highest mean number of blood vessels expressing VEGF compared with groups 1 and 2.
The diode laser as well as the LLLT can increase blood flow without a perceptible temperature increase. This fact allows the application of LLLT during any stage of disease progression, mainly during the immediate postsurgical period. 26 However, its exact mechanism remains unknown.
Some hypotheses have been raised in the literature in an attempt to explain this finding, such as an increase of fibroblast synthesis occurring after the increase of mitotic activity of the cells, and proliferation and delivery of fibroblast basic growth factor strongly helping neovascularization, which increases vascular perfusion, 12,37 and a possible mechanism of autonomic nervous system modulation promoted by the LLLT. 11 According to Schindl et al., 28 the capacity of the low-level laser to promote angiogenesis and to increase blood flow could provide the supply of oxygen and more adequate nutrients to meet the needs of the proliferative phase of the tissue repair process.
The immunohistochemical markers most extensively used for the study of cell proliferation are the proliferating cell nuclear antigen (PCNA) and the Ki-67 antigen. The monoclonal antibody Ki-67 was obtained by Gerdes et al. 38 It is a nuclear and nucleolar protein found in proliferative cells, but not in cells at rest. And no studies on skin flaps were found in the researched literature. In the present study, the proliferative activity measured by the Ki-67 marker was significantly higher in the basal layer of the epidermis of the groups irradiated with low-level laser.The group irradiated with the 670 nm laser presented a higher number of cells in the proliferative phase, with a consequent lower percentage of tissue necrotic area.
According to the literature, the wavelength is considered to be the determinant of the physiological effects, because it determines which biomolecules will absorb radiation. Stadler et al. 39 reported that hemoglobin, present in red blood cells, can act as a chromophore, participating in the absorption of radiation with wavelengths in the range between 600 and 700 nm. This was confirmed to have intensified the effects of irradiation of lymphocyte cultures with 5 J/cm2, with an increase of SOD, which acts as an antioxidant by removing excess superoxide. And Prado et al. 40 showed that LLLT was efficient in increasing random skin flap viability in rats, with no significant difference between 830 and 670 nm lasers, although the 670 nm laser was efficient in reducing tissue malonylaldehyde levels.
Experimental studies are being performed to evaluate tissue necrosis in skin flaps. However, the results are first based on the percentage of the necrosis area. In order to obtain more detailed information about the causes of necrosis several, some studies have analyzed the microcirculation of these flaps. To do so, many techniques have been used to improve blood intake, such as polarographic electrodes, 41 measurement of blood flow by laser Doppler fluxometry, 30 and microspheres. 1
Nevertheless, all these techniques measure indirect indicators of vascular perfusion and none of them allows the evaluation of the hemodynamic and cellular mechanisms, which could minimize and prevent tissue necrosis.
The present study aims to contribute to the scientific literature in the attempt to reduce tissue necrosis and to show the effect of LLLT based on VEGF tissue concentration and cellular proliferation index (Ki-67), which are considered to be very important aspects related to the mechanism of increased vascular perfusion. Therefore, we concluded that low-level laser stimulated the release and secretion of the growth factor related to angiogenesis, which is essential for the development of the vascular growth system and one of the earliest events in organogenesis. Therefore, the laser treatment used here becomes essential for the tissue repair process and to re-establish the blood flow of the tissue lesions, as shown by the increased amount of epithelial cells in the proliferative phase, consequently, causing a reduction of tissue necrosis, especially at the wavelength of 670 nm.
Conclusions
LLLT was efficient in increasing random skin flap viability in rats, with the 670 nm laser being more effective.
Footnotes
Acknowledgments
The authors gratefully acknowledge funding from The National Council for Scientific and Technological Development (CNPq) and Fundação de Apoio ao Ensino, Pesquisa e Assistência (FAEPA).
Author Disclosure Statement
No conflicting financial interests exist.