
Abstract
Introduction
Studies have shown that tea polyphenols can protect the skin against UV damage. 3 Proanthocyanidins, a group of polyphenolic bioflavonoids, widely available in fruits, vegetables, nuts, seeds, flowers, and barks of some plants, have been reported to exhibit strong biological properties. 4 Some experiments have demonstrated that GSPE is highly bioavailable and can provide significantly greater protection against such diseases as skin whitening, TPA-induced hepatitis, and brain lipid peroxidation than ca vitamin C and vitamin E. 4, 5 GSPE is used experimentally in many fields such as ischemia-reperfusion injury, 6 chronic pancreatitis, 7 and even cancer. 8,9 Here, the cutaneous photoprotection properties of GSPE were studied.
One of the major consequences of exposing skin to ultraviolet radiation is the generation of sunburn cells (SBCs). 10 The morphological feature of SBCs is typical of apoptosis, which starts with cell shrinkage and blebbing of the cytoplasmic membrane, followed by condensation of the chromosome and genomic DNA damage. 11 In the present study, we investigated the protective effects of topical GSPE against acute UV injury in vivo in humans. We especially focused on the role of GSPE in SBC formation, p53 expression, and change of Langerhans cells–epidermal immune cells.
Materials and Methods
Subjects
Men and women aged from 18 to 50 years were eligible for the studies. All subjects were in excellent health, not on medication, and had no history of skin diseases or abnormal reactions to sun exposure. Written consents were obtained from all participants in the study. All volunteers were all financially compensated after finishing the experiments. The protocol was approved by the Institution Ethics Board of the Air Force General Hospital. Ten volunteers, six women and four men with Fitzpatrick skin phototype III and phototype IV participated in this study (mean age 34.3 years, aged from 22 to 42). Personal information is shown in Table 1.
SPF, sun protecting factor; GSPE, grape seed proanthocyanidin extract.
Antibodies and reagents
Purified GSPE (95% of purity) was gifted by M.D. Liu (An-xin Co. Ltd., Shenzhen, China) with the chemical composition shown in Table 2. Mouse anti-human CD1a monoclonal antibody and monoclonal antibody p53 that recognizes mutant p53 protein were purchased from NeoMarkers (NeoMarkers, Frement, CA). GSPE solution (0.08 mg/mL) was prepared by weighing 0.8 mg of GSPE and dissolving it in 10 mL of 1:1 ethanol/water vehicle.
GSPE, grape seed proanthocyanidin extract.
UV irradiations and dosimetry
Evaluation of the minimal erythema dose (MED) was performed with Multiport Solar Simulators GS-2000 (Aohua Co., Beijing, China). 12 This sun simulator includes a 450 W xenon lamp and a dichroic mirror. Radiation was filtered with a WG 320, 1-mm thick short cutoff filter, plus a UG 11, 1-mm thick long cutoff filter (Schott, Clichy, France) to deliver a continuous UV spectrum from 290 to 400 nm for the measurement of MED and solar simulated radiation (Fig. 1). The irradiances at skin level were monitored with a calibrated digital spectroradiometer (National Institute of Measurement, Beijing, China). The percent of UVB and UVA radiation emitted are 5% and 95%, respectively. The lowest doses resulting in uniform erythema over the radiation sites after 24 h were considered as the MED.
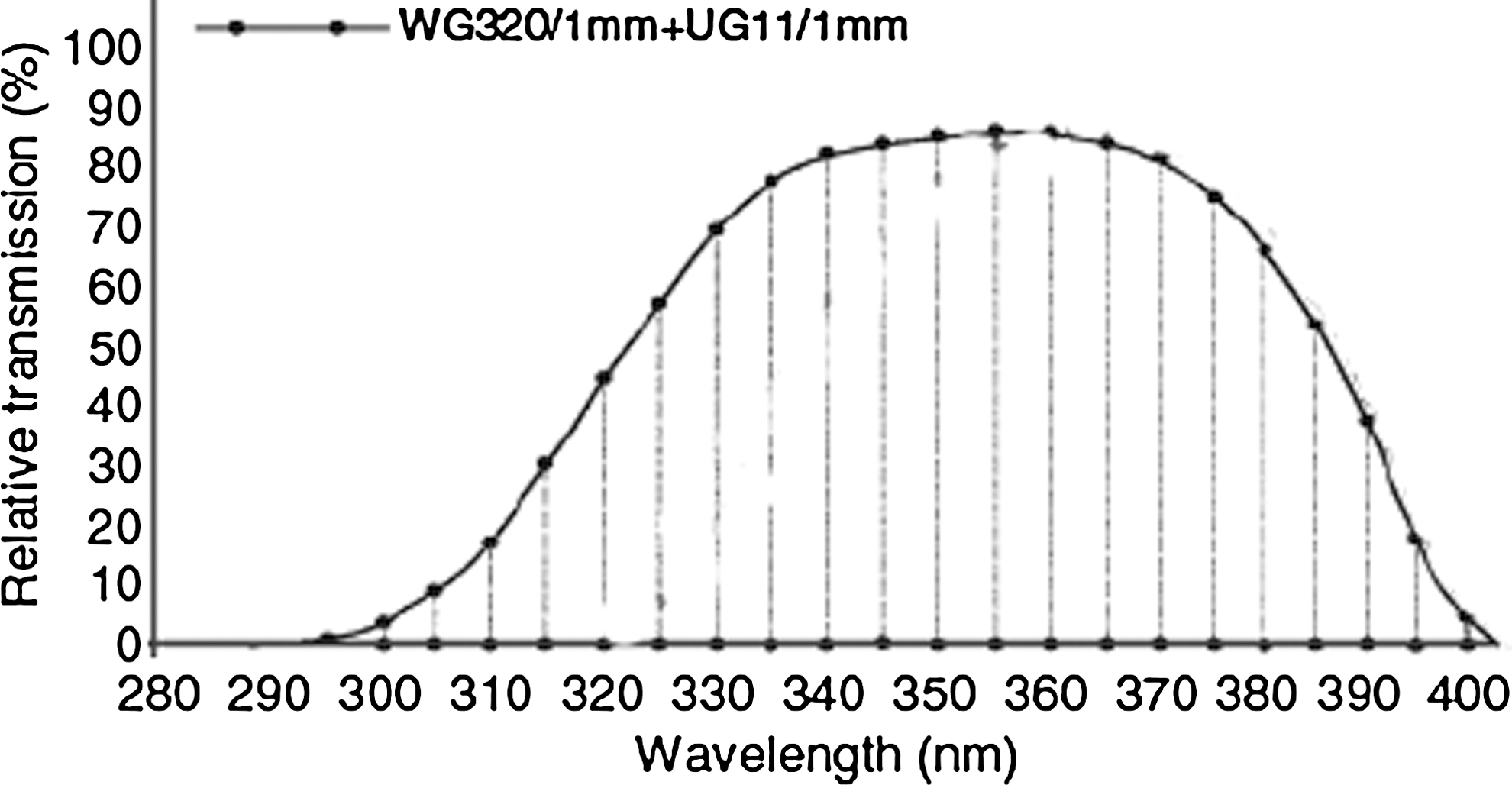
Relative transmission of the filters in the solar simulator is shown. Schott WG 320/1 mm plus UG 11/1 mm are used for the measurement of minimal erythema dose (MED) and simulated solar radiation (SSR).
Experiment design
Five visits per person were required. During the first two visits, each individual MED was determined by exposing the skin to graded doses of UV radiation from Multiport Solar Simulators GS-2000. The lowest doses resulting in uniform erythema over the radiation sites after 24 h were considered as the MED. At the same time the sun protecting factor values (SPF) of GSPE were detected on these volunteers.
The experiments were designed in four groups, with cutanous areas on the back of each volunteer being marked with four 7×3 cm sites, which meant that 10 persons were involved in each group. The first sites of all volunteers, Group 1 (Normal skin group), were given no treatment; the second sites, Group 2 (UV group), were exposed to 2 MED solar-simulated radiation (SSR) for 3 consecutive days; the third sites, Group 3 (Vehicle+UV group), were treated with the vehicle 30 min before a 2 MED dose SSR for 3 consecutive days; and the fourth sites of each volunteer, Group 4 (GSPE+UV group), were pretreated with GSPE solution 30 min before exposure to 2 MED SSR for 3 consecutive days.
A 0.8-mL. solution of GSPE or vehicle was applied to the marked areas on corresponding sites before 2 MED SSR. Volunteers returned 24 h after the final exposure, in which 3-mm punch biopsies were taken from the center of each marked area. The specimens were fixed in formalin and embedded in paraffin.
Measurements of SBCs
Skin biopsy specimens were fixed in 10% neutral buffered formalin and processed for routine histology. SBCs were identified by round shape, with loss of connection with surrounding keratinocytes, suprabasal localization, and typically eosinophilic cytoplasm surrounding dense and contracted nuclei, or by severely swollen nuclei plus vacuolated cytoplasm. 13 The entire 3-mm central section of the histological ribbon was analyzed and the results expressed as SBCs per 10 high-power fields. All the histological specimens were read in a blinded fashion.
Immunohistochemical detection of CD1a+ Langerhans cells and mutant p53-positive cells
Immunohistochemical detection of CD1a+ Langerhans cells and mutant p53-positive cells was performed as described. 14 In brief, formalin-fixed, paraffin-embedded tissue sections were deparaffinized, dehydrated, equilibrated in phosphate-buffered solution (PBS), and blocked with 10% goat serum in 2% bovine serum albumen/tris buffered saline (BSA/TBS) for 30 min at room temperature. Some tissues sections were incubated with rabbit mutant anti-p53 antibody or with mouse anti-human CD1a monoclonal antibody overnight at 4°C in 2% BS/TBS. With each primary antibody that was used, a rigorous staining optimization protocol was applied. Antigen retrieval by either microwave treatment or enzymatic digestion was performed. Sections were washed and incubated with horseradish peroxidase-conjugated streptavidin (NeoMarkers, Frement, CA) and the immunoreactivity was developed by adding 3-amino-9-ethyl-carbazole (Maxin Company, Fujian, China) from 8 to 20 min until satisfactory staining was obtained (the whole procedure was monitored under the microscope). The number of Langerhans cells and p53- positive epidermal cells were counted as with the SBC described previously.
Statistical analysis
Mean and standard error were calculated for all data. The student t test was used for comparison between groups with a p value<0.05 considered significant.
Results
No undesirable effects caused by the treatment were reported, and compliance was excellent. All subjects completed the trial, and none failed to observe the protocol. SPF of GSPE of each volunteer varied between 1.5 and 3.75. The results are shown in Table 2.
The different skin sites of volunteers were unexposed or exposed to 2 MED of UV radiation daily for 3 consecutive days. Histological analysis of untreated and treated skin was taken 24 h after exposure to 2 MED of solar simulated radiation. Damaged keratinocytes compressed in the superficial epidermis, as well as vacuolation of keratinocytes and intercellular edema could be seen in skin areas of the UV group and the Vehicle+UV group. The number of SBCs was found to be highest in the UV Group and the Vehicle+UV group (Fig. 2). There was a significant decrease of SBCs in the GSPE+UV group compared with the UV group and the Vehicle+UV group. The results demonstrated that treatment with topical GSPE provided protection against SBC formation induced by SSR. The results are shown in Fig. 2A and B.
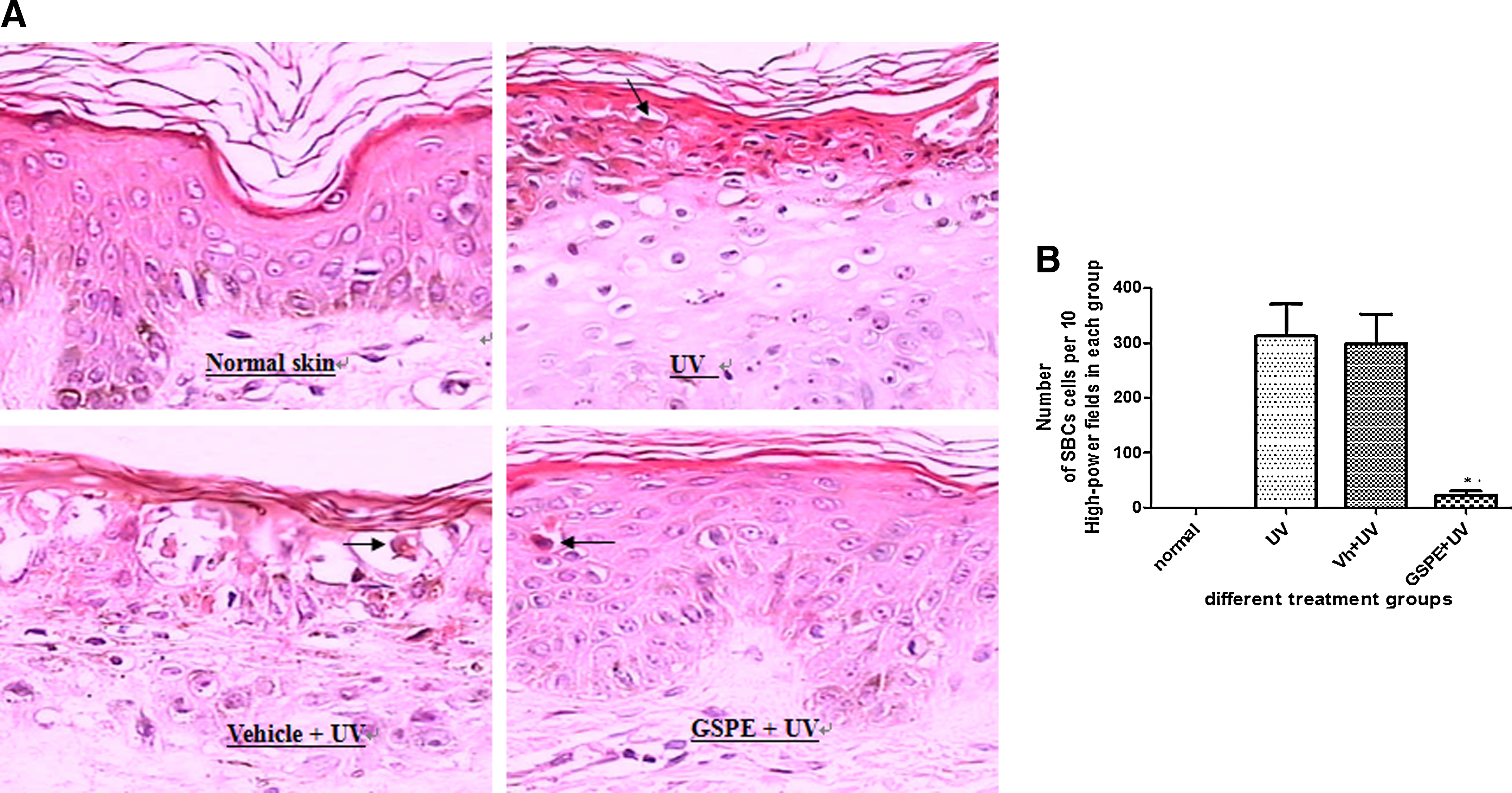
Histologic appearance and sunburn cell (SBC) count of different treatment groups.
In normal skin, the number of cells expressing the p53 marker was 10±2/10 high-power fields. The increase in the number of mutant p53-positive cells of the UV Group and the Vehicle+UV group compared with the normal skin group was statistically significant. The group with GSPE treatment (GSPE+UV group) had reduced mutant p53-positive cells compared with the UV group (p<0.001). The results are shown in Fig. 3A and B.
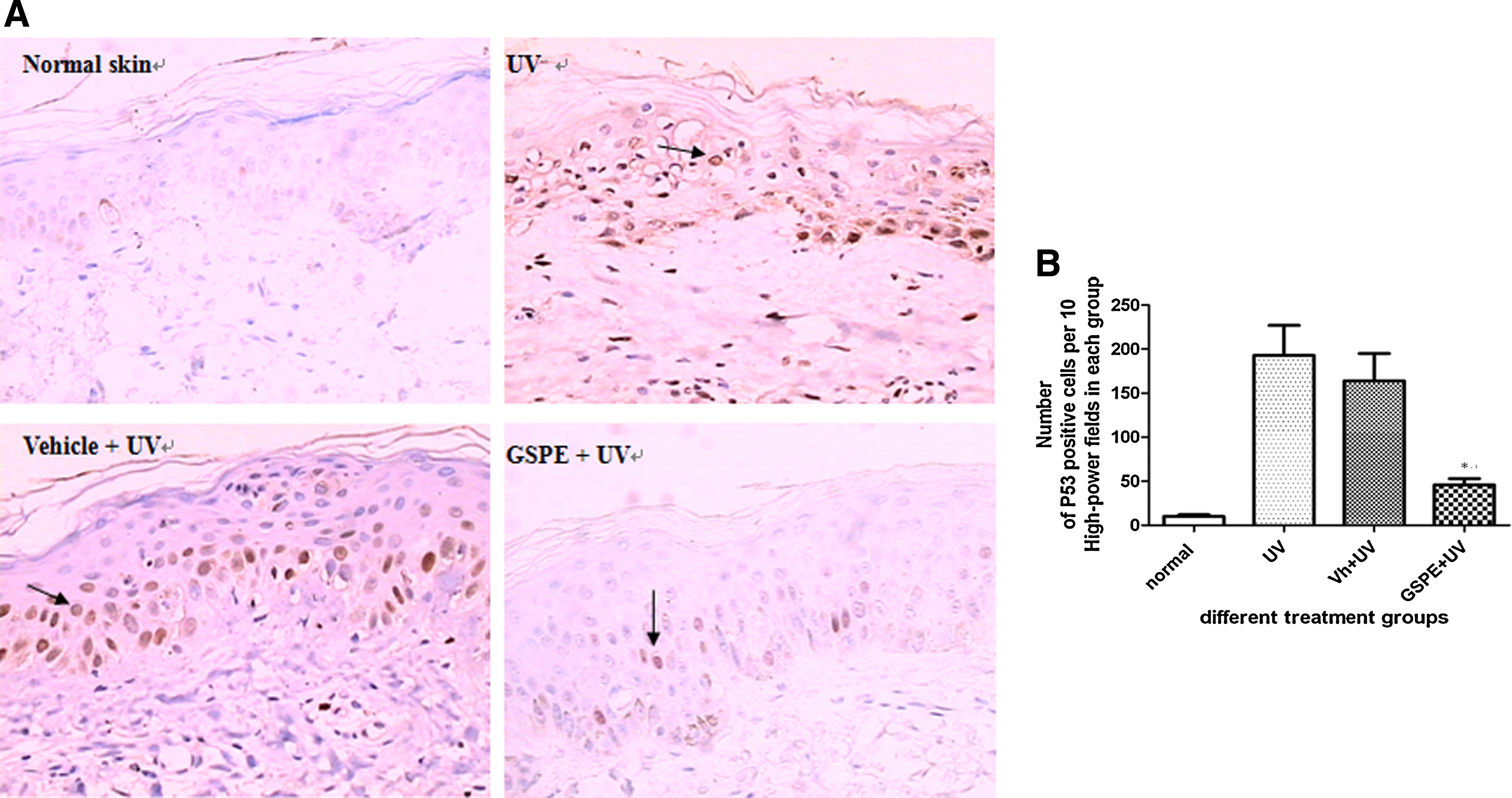
Immunohistochemical detection of mutant p53-positive cells in tissues and mutant p53-positive epidermal cell count of different treatment groups.
Langerhans cells in the epidermis are bone marrow derived antigen-presenting cells (APC) and represent the first line of defense against environmental stimuli encountered by the epidermis. Studies have shown that the number of epidermal Langerhans cells will be decreased or depleted by UV radiation, leading to immune suppression.
Disappearance of Langerhans cells could be seen in some skin sections of the UV group and the Vehicle+UV group in our experiment. Application of GSPE before UV exposure resulted in almost total reconstitution of this epidermal immune cell population. In most of sections in the GSPE+UV group, we also found more dendrites and longer dendrites in most of the Langerhans cells, which may be signs of immune activation. The results are shown in Fig. 4A and B.
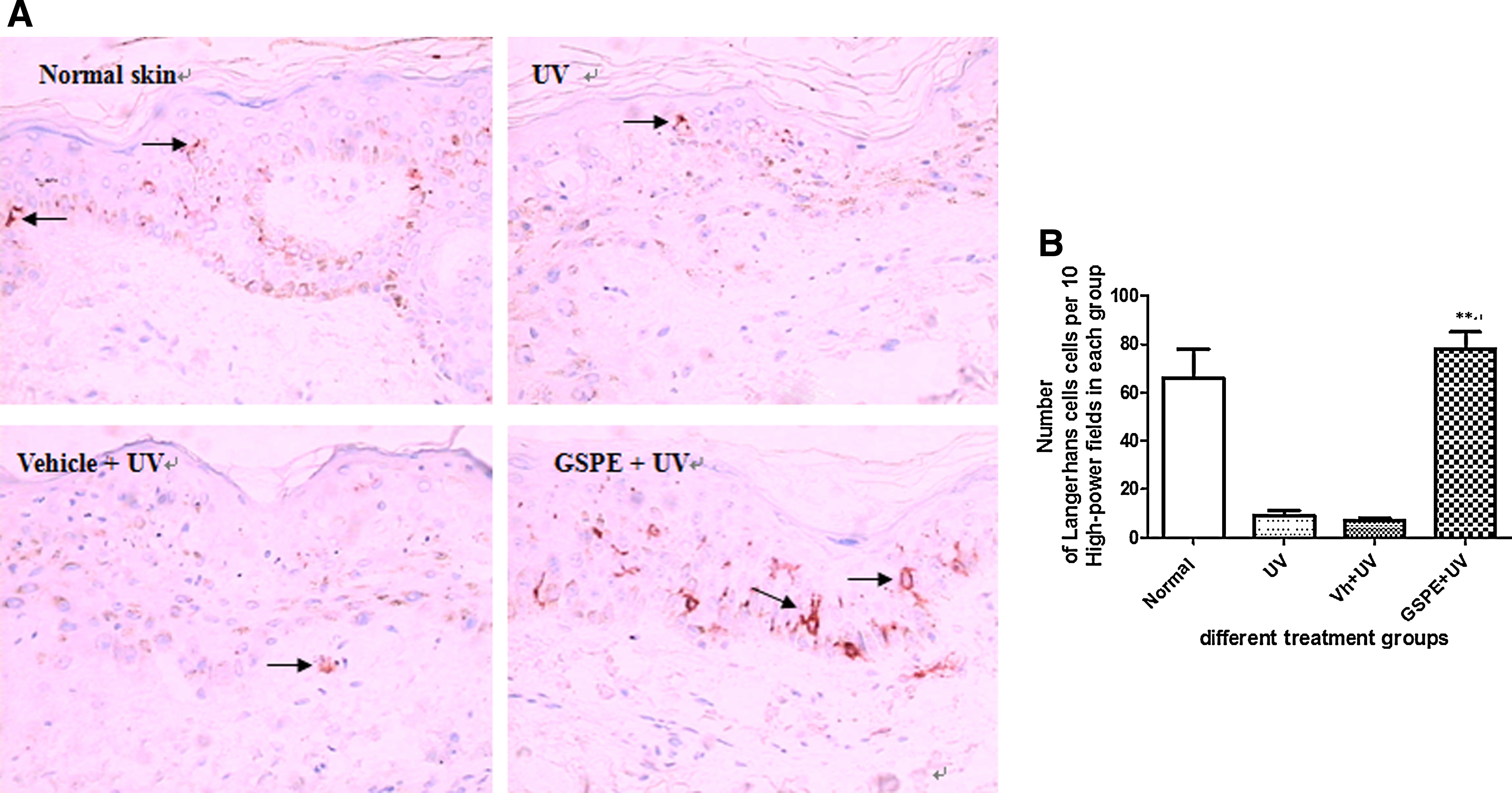
Immunohistochemical detection of CD1a+ Langerhans cells in tissues and Langerhans cell count of different treatment groups.
Discussion
SBCs can be seen in skin areas of acute sun injury and are often signs of apoptosis. 8, 15 Our study showed that areas of skin that were pretreated with GSPE before exposure to 2 MED SSR reduced the SBC formation, in other words, reduced DNA damage induced by UV radiation.
The p53 gene is the most commonly mutated gene in human cancers. 16 Patches of morphologically normal keratinocytes that stain positively with an antibody recognizing an altered conformation of the mutant form of p53 protein may represent such an early step. After consecutive days' exposure to 2 MED SSR, we observed many more mutant p53- positive cells; therefore, we can infer that UV-induced mutant p53-positive epidermal cell formation has been long present before the formation of tumors. Topical GSPE obviously reduced mutant p53-positive epidermal cell formation. This result showed that applying GSPE before exposure to UV radiation reduced mutant p53 expression, a tumor initiator and tumor promoter.
Langerhans cells are subpopulations of epidermal antigen-presenting cells. It is well known that they play a key role in the development of cutaneous cell-mediated immune responses. Similarly, depletion of the number of Langerhans cells in the epidermis after UV irradiation has been well documented, and this results in immunosuppression and even photocarcinogenesis. 17 In our study, the reduction or disappearance of Langerhans cells happened after exposure to 2 MED SSR; however, topical application of GSPE before UV exposure resulted in almost equally total reconstitution of this epidermal immune cell population. We also found an interesting phenomenon: more dendrites and longer dendrites in most Langerhans cells could be seen in the skin areas that were pretreated with topical GSPE. These results have never been mentioned by other similar experiments on protection against sun injury by antioxidants, such as green tea polyphenols. 13
One consequence of UV exposure is a shift in the activation of T cells from a Th1 to a Th2-type immune response. 18 Araneo et al. isolated T cells from mice that were exposed to UV radiation and immunized with Antigen (Ag). These cells were then stimulated with Ag in vitro, and IL-2, IL-4, and IFN-γ production was measured. Compared with normal controls, the T cells from the UV-irradiated mice were found to secrete less IL-2 and IFN-γ, but more IL-4, indicative of a shift toward a Th2-like reaction. 19 Wang et al. reported that UV irradiation after immunization induces type 1 regulatory T cells that suppress Th2-type immune responses via secretion of IL-10. 20 Grape seed extract has also been found to activate Th1 cells in vitro. 21 As the studies of Sharma et al. have found, oral GSPE could increase induction of IL-12 (Th2 cytokines) and decrease induction of IL-10 (Th1 cytokines) by UV radiation. 22 All of the abovementioned information may indicate that GSPE can affect the T cells by UV radiation, which is associated with photocarcinogenesis.
To exclude the possibility that GSPE was merely acting as a sunscreen, spectrophotometric analysis was also performed on GSPE in vitro and its SPF value was detected on volunteers. The results showed the UV absorption maximum of GSPE was at 275 nm and that the SPF value of GSPE was < 4. However, the continuous UV spectrum of UV radiation used in our experiment was from 290 to 400 nm (as shown in Fig. 1) and the percent of UVB radiation emitted was only 5%. We also applied GSPE after exposure to UV radiation and obtained similar results (data not shown). These results together indicate that GSPE is not acting simply as a sunscreen as green polyphenol 13 and magnolol. 23
Conclusions
To our knowledge, the data obtained from this study for the first time suggest that topical GSPE can provide photoprotection against UV-induced damage by reducing sunburn cells and mutant p53 epidermal cell formation, and by reconstituting Langerhans cells. Our study fundamentally suggests that GSPE may be a promising chemopreventive agent for photoprotection.
Footnotes
Acknowledgments
The authors thank Professor Wen-Hui Wang for language editing and Jian-You Guo for the preparation of graphic material. We also thank Shiseido China Research Center Co. Ltd for financial support.
Author Disclosure Statement
No competing financial interests exist.