
Abstract
Introduction
Materials and Methods
LED device
The transcranial LED treatments were performed beginning at 228 days post-severe head trauma, caused by a fall when fighting. This is an off-label use for the L-light (Fig. 1), which has a 78 mm wide and 72 mm long (23 diodes; peak wavelength,850 nm [830–870 nm, the full width half-maximum range]; 13 mW per diode; total power 299 mW; the spot size of each LED 0.95 cm2; SUN-MECHATRONICS, Tokyo, Japan) (Table 1). The half-value angle of LED is 6 degrees according to the manufacturer's specification. The device was applied at a distance of 5 mm away from the skin. The estimated beam area per diode on the skin was 1.14 cm2; the power density 11.4 mW/cm2; the energy density 20.5 J/cm2 at the skin. The patient received transcranial LED treatments with placement of the L-light on the left and right forehead areas superior to the eyebrows for 30 min, 2 times daily, for 73 days. The dosage/treatment duration of 30 min twice a day was based on the results obtained in animal studies. 2

A photograph of a model being treated, L-light (SUN-MECHATRONICS, Tokyo, Japan).
CBF measurement
Single-photon emission computed tomography with N-isopropyl-[123I]p-iodoamphetamine (IMP-SPECT) was performed twice. Prior to LED therapy, the IMP-SPECT scan was performed at 227 days post-head trauma. Post-LED therapy, the IMP-SPECT scan was performed at 300 days post-head trauma, and following 73 days of LED therapy, and 146 LED therapy treatments. It was performed within 30 min of the last LED treatment. At 10 min after the beginning of the IMP infusion, 3 mL of arterial blood was obtained from the radial artery. The whole-blood radioactivity of 1 mL of each blood sample obtained was measured by using a well counter that was cross-calibrated to the SPECT scanner. All reconstructed SPECT images were corrected for the radioactive decay of 123I back to the IMP injection start time, normalized by the data collection time, and cross-calibrated to the well counter system. The whole-blood radioactivity count of the single blood sample was referred to the standard input function. The absolute value of regional CBF (rCBF) was thus obtained.
Results
Case presentation
A 40-year-old man underwent craniotomy over the left frontal areas and evacuation for traumatic acute subdural hematoma, secondary to a fall from fighting. Initial neurological examination showed a score of 5 on the Glasgow Coma Scale. He survived but was in a persistent vegetative state for 8 months after the trauma. He showed no spontaneous movement of limbs. A CT scan of the head 8 months after accident showed a focal low-density area in the right frontal lobe (Fig. 2A). He showed no symptoms and signs of increased intracranial pressure at 8 months. After approval by the institutional review board of National Defense Medical College, the appropriate informed consent was obtained, and the transcranial LED treatments were initiated. This is an off-label use for the L-light (SUN-MECHATRONICS, Tokyo, Japan) (Fig. 1 and Table 1). He received transcranial LED treatments with continuous-wave L-light on the left and right forehead areas superior to the eyebrows for 30 min twice daily for 73 days. The interval between the two treatments on the same day was 6 h. Five days after beginning the LED treatments (after 10 treatments), the patient began to move his left arm and hand to reach the site of tracheostomy when suctioning was performed. He had never shown any spontaneous movement prior to the LED treatments. After LED treatment for 2 months, which ended 300 days post-head trauma, he always showed spontaneous movement, but did not obey commands. We observed no further improvement in his neurological condition after LED treatments.
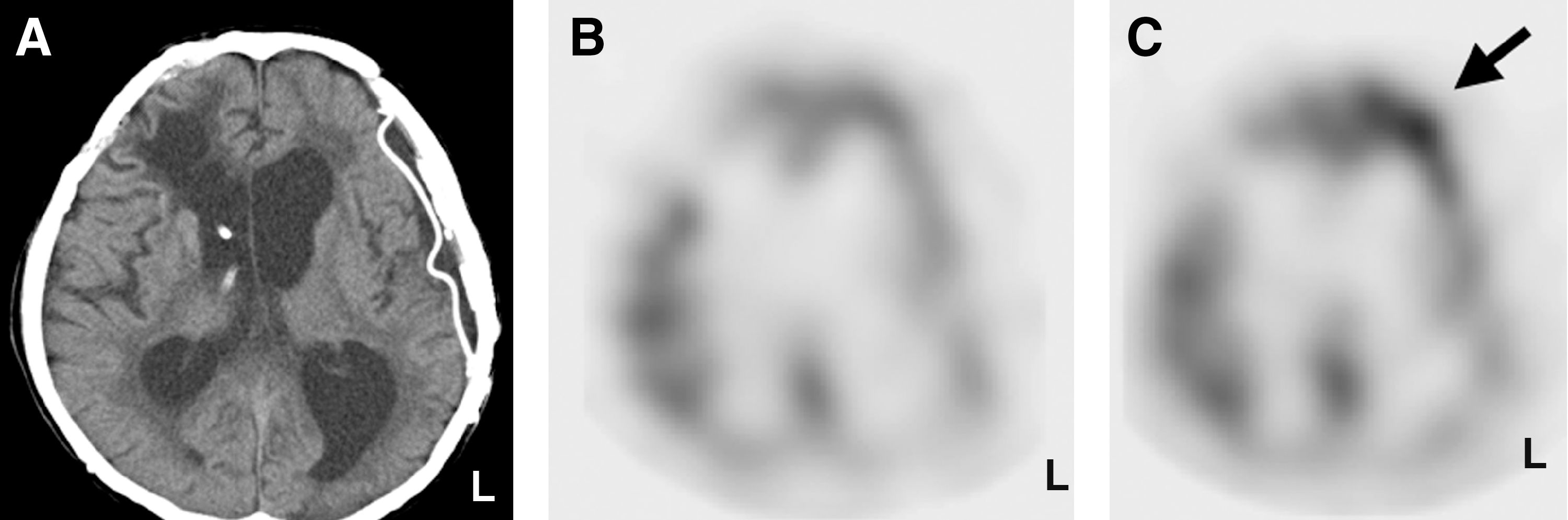
IMP-SPECT showed focal increase (20% higher) of CBF in the viable left anterior frontal lobe 30 min after the 146th LED treatment, which was performed on the 73 days of the LED treatment series, and 300 days post-trauma (Fig. 2B and C).
Discussion
Positive behavioral improvement has been observed following transcranial near-infrared light therapy in humans with chronic traumatic brain injury; 1 acute stroke; 3 –5 and chronic severe depression. 6 These studies suggest that, at least in part, near-infrared light can penetrate the scalp and skull, and reach the cerebral cortex in humans. The Schiffer et al. study 6 observed increased CBF in the frontal pole areas following a single, near-infrared LED treatment to F3 and F4 (10/20 EEG system) in the lateral-superior forehead region.
We have previously demonstrated a targeted increase of CBF by applying transcranial near-infrared light irradiation in rats. 2 This is the first quantitative measurement demonstrating focal increase of CBF by near-infrared light irradiation in humans using IMP-SPECT, which can be used for the quantitative estimation of rCBF in normal and pathological states, with high reproducibility. 7 It has been reported that variation of rCBF in the same patient can range from 0.3% to 15% (mean 6.2%). 7 In the present case, increased rCBF (20% increase) in the left anterior frontal area is not likely to be caused by spontaneous change, because no other areas showed increased rCBF. With the exception of the right anterior frontal area, none of these other cortical brain areas received LED therapy. IMP-SPECT showed continued low rCBF in all other areas following the LED therapy series to the left and right forehead areas. It is unknown why there was no increase in the right anterior frontal area, despite LED therapy at this location. The low-density area in the right anterior subcortical white matter area, anterolateral to the right frontal horn, may have played a role. The laterality of the increased rCBF (left anterior frontal cortex) was not related to the side of spontaneous upper extremity movement (left arm/hand). Stimulation of left dorsolateral prefrontal cortex may be responsible for improved akinesia in this patient. Further studies, including more scalp placement areas and perhaps an LED device with a higher power density, are required to determine greater potential for long-term improvement in cases of persistent vegetative state, or coma.
Conclusions
Transcranial LED might increase rCBF, with some improvement of neurological condition in severely head-injured patients. Further study is warranted.
Footnotes
Acknowledgments
We thank Mr. Hayakawa at SUN-MECHATRONICS, Tokyo for providing specifications of L-light.
Author Disclosure Statement
No conflicting financial interests exist.