
Abstract
Introduction
Apicoectomy with retrograde filling is a well-established surgical procedure to treat teeth affected by persistent periapical lesions. 3,4 The apical root end is generally removed with burs, and the adjacent periapical tissue curetted, or alternatively treated with ultrasound or laser.
In 1971, Weichman et al. 4 first demonstrated the possibility of using laser photonic energy in endodontics. Numerous other studies since have explored the use of different types and modes of laser for sterilizing root canals. These include the CO2 laser, 5 ,the neodymium-doped yttrium aluminium garnet (Nd:YAG) laser (1064 nm), 6 the excimer laser (308 nm), 7 the diode laser (810 nm), 8 the erbium:yttrium-aluminum-garnet (Er:YAG) laser (2640 nm), 9 and the neodymium:yttrium-aluminum-perovskite (Nd:YAP) laser (1340 nm), 10 all of which also possess marked bactericidal power, operating at different power settings for the different types of laser. In 1983, Eriksson and Albrektsson 11 introduced another concept that is indispensable if use of the laser is to result in a successful outcome: if it is to survive, bone subjected to laser treatment must not undergo heating to >47°C for 1 min. They also reported that excessive power may cause thermal damage to periodontal tissues. These damaging effects can be minimized by using the laser in a pulsed emission mode. The effects of such parameter manipulation may be seen with differing laser wavelengths; 12 it has been observed that the Er:YAG laser produces smooth root surfaces, free of impurities and without areas of charring, when working in pulsed mode at energy levels between 50 and 90 mJ. 13 The Er:YAG laser also not only removes the smear layer better than the argon or Nd:YAG lasers, 14 –16 but also possesses enhanced anti-inflammatory power, reducing bacterial infiltration within the resected root after apicoectomy and retrograde obturation. 17,18
The aim of this study was to evaluate the efficacy of erbium lasers (Er:YAG and Er,Cr:YSGG lasers) in retrograde endodontic treatment, in terms of clinical outcome and treatment success.
Materials and Methods
The study comprised a series of 65 otherwise healthy patients with periapical lesions at the incisors, canines premolars, or molars, previously diagnosed on the basis of clinical and radiological findings.
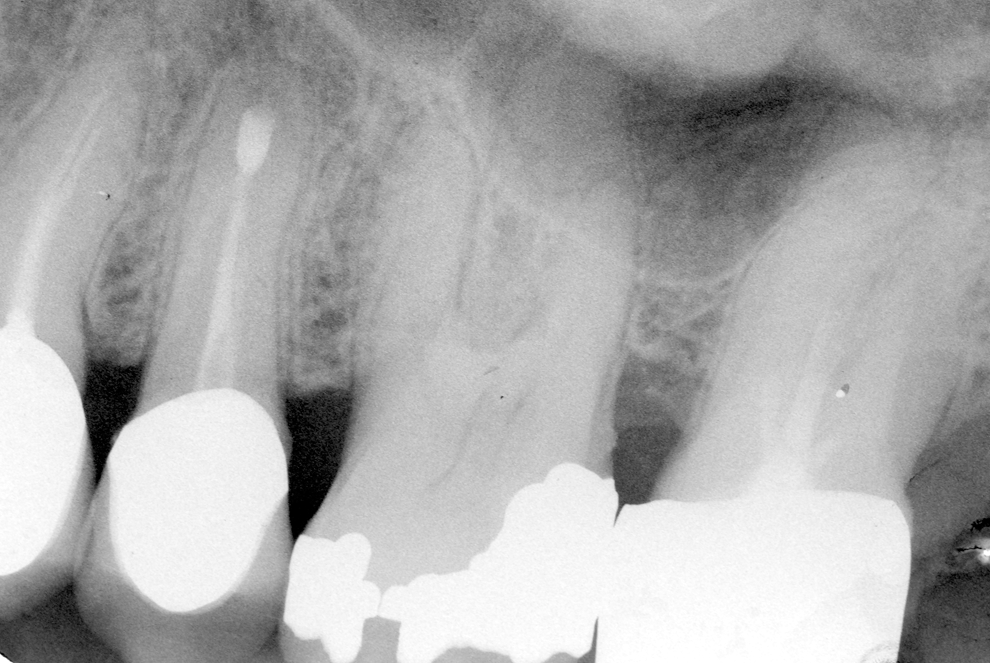
Apicoectomy was performed in 29 men and in 36 women at the Italian Stomatological Institute in Milan, and at the Department of Oral Surgery, Genoa University, during the period between 2000 and 2010. All quadrants were involved in the apical resections (I quadrant, 29 cases – 45%; II quadrant, 21 cases – 32%; III quadrant, 8 cases – 12%; IV quadrant, 7 cases – 11%). The treatment protocol was as follows: with the patient under local anesthesia (2% carbocaine and 1:100.000 adrenaline) apicoectomies were performed in necrotic teeth with apical lesions (Fig. 1), using two types of laser: Er:YAG 2940 nm (Opus 20, Lumenis LTD, Yokneam, Israel); and erbium,chromium-doped:yttrium-scandium-gallium-garnet (Er,Cr:YSGG) 2780 nm (Waterlaser Biolase Technology Inc., CA). Laser characteristics and settings were as follows.

Periapical radiographic image of tooth 15 devitalized with apical lesion.
• Opus 20, Lumenis LTD, Yokneam, Israel Er:YAG 2940nm, pulse width 200–400 μsec, conduction in hollow fiber, curved hand piece, truncated cone HPX tip, 400 μm with the following parameters: to open the mucoperiosteal flap, power 250 mJ, frequency 12 Hz, air/water spray 80mL/min; osteotomy and removal of apex, HPX 600 μm tip, power 400 mJ, frequency 15 Hz, air/water spray 100mL/min.
• Waterlase Biolase MD, (Biolase Technology Inc. CA) Er,Cr:YSGG 2780 nm, conduction in optical fiber, curved hand piece, 400 μm truncated cone MT4 tip, length 6 mm, with the following parameters: to open the mucoperiosteal flap, power 2.5 W, frequency 15 Hz, 60% air/40% water spray, S (Soft tissue) mode, pulse width 700 μsec; osteotomy and removal of apex with 600 μm MG6 tip, length 6 mm, power 3.5 W, frequency 20 Hz, 55% air/45% water spray, H (Hard Tissue) mode, pulse width 140 μsec; decontamination of canal, with MZ3 320 μm tip, length 9 mm, power 2.0 W, 70% air/30% water spray.
Surgical procedure
All the phases of endodontic surgery (mucosa incision, osteotomy, apical resection, cavity preparation) were performed by delivering laser photonic energy. The mucosal incision design was marginal, paramarginal, or semilunar, depending upon anatomical specifics and surgical requirements (Fig. 2). The full-thickness mucoperiosteal flap was elevated, after which laser osteotomy was performed. The osteotomy area and the periapical zone were decontaminated with laser photonic energy where possible; undercut areas and others impossible to reach were decontaminated with curved ultrasound tips, and with surgical curettes with curved tips. In particular, some erbium lasers are fitted with flexible terminals of varying lengths, with which canals may be cleansed for some millimeters. Canals were decontaminated with the same tip, the curved tip (provided that the canal anatomy allowed it), for a minimum length of 3 mm after resection (measured with a millimeter probe) or, if access was unfavorable or complex, with an ultrasound hand piece. The infected area was finally washed with 20 mL of physiological solution (50%) and hydrogen peroxide (50%) to aid removal of any debris deriving from the surgical maneuvers. The cleansed canal was then closed with cement. The flap was sutured with interrupted sutures of 3/0 braided silk thread, needle V-5 Ethicon, and with 3/0

The semilunar-design mucosal incision is made with the Biolase Waterlase MD, Er,Cr:YSGG 2780-nm laser, conduction in optical fiber, curved hand piece, 400-μm truncated cone MT4 tip, length 6 mm, with the following parameters: to open the mucoperiosteal flap, power 2.5 W, frequency 15 Hz, 60% air/40% water spray, S (soft tissue) mode. The osteotomy was prepared with tip MG6, length 6 mm, 600 μm, power 3.54.0 W, frequency 20 Hz, spray air 55%, water 45% mode H (hard tissue).
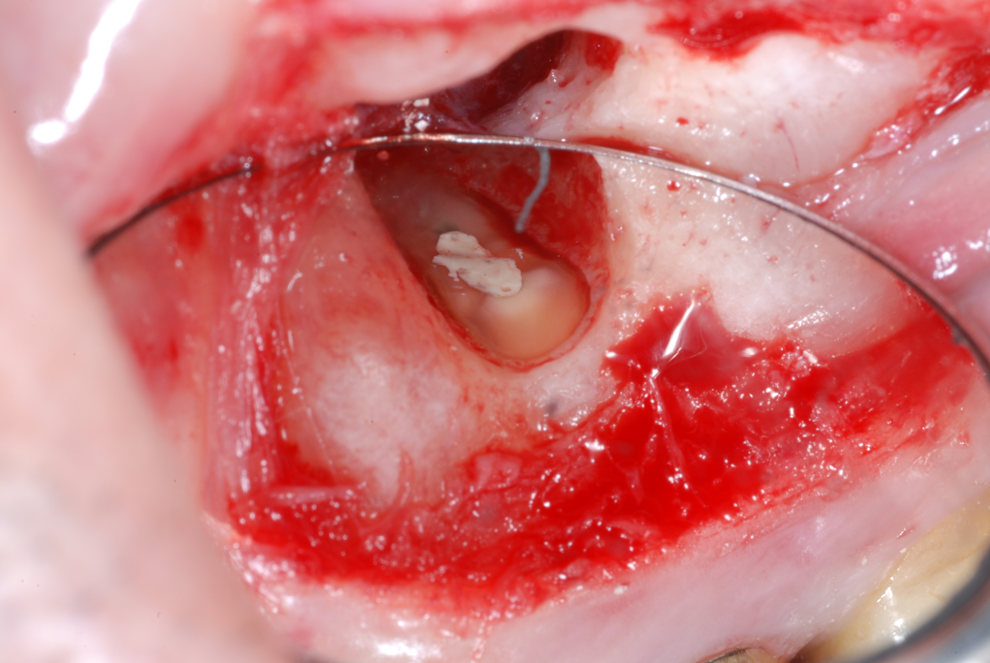
The resected root surfaces showing the SuperEBA Bosworth cement; the filling material is perfectly adapted to the site.
Postoperative course
Pharmacological treatment comprised administration of amoxicillin 1 g capsules, 2 capsules per day for 5 days or, in the case of intolerance of penicillin, spiramycin 3,000,000 U capsules, 2 capsules per day for 5 days, or azithromycin 500 mg capsules, 1 cap per day for 3 days. In all cases, patients were instructed to use gel-bearing trays to apply 0.2% chlorhexidine-based gel to the treated zone, for 5 min twice daily for as long as the sutures remained in place. The patients were followed up for 1 year, for 3 years, or for >5 years.
Patients were monitored through orthopantomography, preoperative and postoperative intra-oral radiograph (Fig. 4), intra-oral radiograph at 3 months, at 6 months, and every year after surgery (Fig. 5).

Intra-oral radiograph post-surgery.
Intra-oral radiograph after 36 months.
Results
Of the 65 cases in the study, failure only occurred in nine treatment sites and it occurred at different times. At the immediate follow-up there was one case (tooth 14, QI) of formation of a fistula at the median third of the root; this was successfully treated (decontamination with 980 nm diode laser (Dental Medical Technologies, Lissone (MB) Italy), 320 μm fiber, power 2.0 W in pulsed mode (50 ms on, 50 ms off ) in a single session, accompanied by irrigation of the fistula with 1% polyvinylpyrrolidone iodine, 50% 12-volume hydrogen peroxide/50% physiological solution) and one case of root fracture (tooth 25, QII). At follow-up 3 years after apicoectomy, there were two cases of relapse, resolved by surgical retreatment (tooth 36, QIII and tooth 17, QI), and one fracture of tooth 46, QIV, subjected to double apicoectomy on both its roots; 9 months later it was replaced with two titanium implants. There were also two cases of endoperiodontal recontamination with subsequent tooth loss (tooth 13, QI and tooth 24. QII). At 5-year follow-up, two root fractures were detected (tooth 13, QI and tooth 25, QII) with subsequent tooth loss. In all other cases healing was excellent.
Discussion
Since 1988, many studies have attempted apical resection with the CO2 laser, but without achieving the hoped-for success. 6 Later studies that evaluated the characteristics of different types of laser, showed the Er:YAG laser to be the best for root resection and apicoectomies, because it improved healing and increased postoperative patient compliance. 19 –21 Although with the Er:YAG laser (350 mJ and 6 Hz) the cutting speed is slightly slower than with traditional surgical methods, in clinical practice its use reduces the risk of contaminating the surgical site and of causing trauma to adjacent tissues. 19,22,23 Furthermore, it has also been reported that with this type of laser, preparation of the retrograde cavity is significantly quicker and cleaner than with ultrasound, whereas there is no significant difference in the quality of seal of the prepared retrograde cavities. 22,23 A study that used the scanning electron microscope (SEM) and the traditional optical microscope to analyze apicoectomies, performed with either Er:YAG laser or with Nd:YAG laser, found that the best apical seal was achieved with the Er:YAG laser for apicoectomy, but that the Nd:YAG laser was better for preparation of the retro-cavity, because it reduced the permeability of dentin. 24 The more recent introduction of the Er:YAG laser presents the possibility for laser surgery to include bactericidal and sterilizing action in periapical surgery; the absence of secondary heat damage defines the laser as an instrument of choice for these treatments. 25
Its reported that the Er:YAG and the Er,Cr:YSGG laser, set at 5.0 W and 20 Hz, have good cutting capacity without causing carbonization of the root end surface. 26 However, in a pilot study, charring was observed on the apical surface when the above parameters were used to make root end resections. 27 In the present study, the laser power was reduced to 3.5 W. A correlation has been found between the presence of cracks and thin layers of remaining dentin. 18 In the present study, no cracks were visible at radiographic examination, even with a remaining dentin thickness of <1 mm The Er,Cr:YSGG laser is outstanding in that it offers good cutting capacity for the root end surface. It does not cause carbonization or thermal damage 7 when used with adequate parameters. It also has antimicrobial activity 8,9 and can be used in endodontic surgery for sterilization of the root end apex and surrounding tissue, root end resection, root end cavity preparation. 10
In the present study, root end cavities were prepared with the laser, finally washing the infected surfaces with 20 mL of physiological solution (50%) and hydrogen peroxide (50%) to aid removal of any debris deriving from the surgical maneuvers. The cleansed canal was then sealed with a SuperEBA Bosworth cement.
The results at clinical checkup were good. Failure occurred in nine cases, occurring at different times. No patient reported pain or presented swelling, immediately after surgery. At the immediate follow-up, one case presented a fistula at the median third of the root, which was successfully treated; one case had root fracture. At follow-up 3 years after apicoectomy, there were two symptomatic cases of relapse, requiring repeat intervention, and one fracture, subjected to double apicoectomy on both its roots. There were also two cases of endoperiodontal recontamination with subsequent tooth loss. At 5-year follow-up, two root fractures were detected, with subsequent tooth loss. The remaining patients, 86.15%, had a positive course.
From these data, it emerges that this form of treatment is not without risk of failure. A moderate number of failures are reported, which, it has been suggested, should be resolved through repeat surgical treatment, rather than through proceeding to extract the tooth. 3 In order to further reduce the risk of failure, it is therefore important to use equipment and methods that ensure conditions of greatest sterility, as well as offering the advantages inherent in surgical and endodontic treatment.
Treatment prognosis depends upon a number of factors, including the type of laser used. The Er:YAG laser removes the smear layer and also has an enhanced anti-inflammatory power, reducing bacterial infiltration within the resected root after apicoectomy and retrograde obturation. 16 –18 The Er:YAG and Er,Cr:YSGG lasers appear to be especially appropriate for this type of operation: they are equipped with a very fine transport optical fiber; they possess bactericidal and sterilizing action; and they do not produce secondary heat damage. All these characteristics mean that these lasers can provide valid help for retrograde endodontic treatment, and are therefore recommended for that type of therapy.
Conclusions
All phases of endodontic surgery may be performed with the Er:YAG and the Er,Cr:YSGG laser.The results of this study show that the erbium laser, used for apicoectomy, results in a high success rate, and that therefore, its use for apicoectomy is recommended. It can be concluded that the use of erbium lasers offers a significant success rate in terms of clinical outcome and success of therapeutic treatment.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.