
Abstract
Introduction
Therapeutic laser treatment, also referred to as low-level laser therapy (LLLT) offers several benefits. For >30 years, LLLT has been an interesting but not well-defined field among the medical, dental, physiotherapy, and veterinary professions. Among the reasons for this are the positive clinical experiences, scientifically verified changes in tissue equilibrium, and, above all, a better understanding of the mechanisms. 2
LLLT can positively impact biologic tissues via improved microcirculation, nerve conduction, and cell proliferation. Other positive effects may include stimulation of the host immune system, increased enzyme activity and DNA synthesis, and enhancement of cell membrane structure. 2 Low dosage levels stimulate tissues/cells whereas high doses can be inhibitory. 2 A review of current knowledge regarding the impact of LLLT on basic cellular mechanisms has been published by Huang et al., 3 whereas the clinical documentation in periodontology has been reviewed by Eduardo et al. 4
Aim
The aim of this study was to investigate whether or not the adjunct use of LLLT could improve the short-term clinical and immunological outcome of traditional scaling and root planing, as well as assessing its effect on the bone density.
Materials and Methods
Participants and study design
To evaluate the potential usefulness of LLLT in periodontal treatment, 16 patients (4 males and 12 females), consulting at the dental outpatient clinics of three public hospitals supervised by the Egyptian Ministry of Health in Cairo, were selected. The participants in this study were chosen from chronic periodontitis patients referred to these clinics. Selection of patients was in accordance with the approval of the local ethical committee. The following criteria were mandatory for including patients in the study group: patients were aged between 22 and 50 years; had chronic periodontitis with contralateral pockets with a probing depth of 4–6 mm in at least three teeth in each quadrant; were healthy, with no systemic diseases according to the Cornell Medical Index and were not taking any type of medication; and were not pregnant or planning to become pregnant in the following 6 months. All patients were nonsmokers and had not received any periodontal treatment during the last 6 months. None of the participants had ever received laser treatment before. Therefore, the patients had no particular anticipation of the effect of this treatment. The 16 selected patients included in the clinical study received complete documentation concerning the trial, and were briefly informed about the biologic effects of LLLT before its use, and a written informed consent form was signed by all participants. After inclusion, each patient was ascribed a randomization number. All included patients completed the study. The study was conducted from May 2008 to June 2009.
The study was planned as an intra-individual short-term test of 12 months' duration, using a split-mouth randomized design. At baseline, one side was randomly assigned as the control site and the other as the laser site. All teeth were treated conventionally, and minimally two, and when possible three, teeth of each side were selected for the study. The selection was done in order to locate teeth with similar pocket depths in each quadrant.
At baseline, cause-related therapy consisting of one single session of full-mouth scaling and root planning (SRP), motivation, and oral hygiene instructions were given. The patients were controlled weekly for 6 months to check on oral hygiene compliance. At these sessions only superficial debris, if present, was removed. Patients who did not follow the oral hygiene measures were excluded from the study. The main author (MM) randomly allocated the quadrants for active laser or placebo (laser shut off) and performed the clinical and laser treatment. The clinical examination and gingival crevicular fluid (GCF) sampling at the control dates were performed in the same manner as at the baseline. All clinical parameters were measured by a different experienced examiner who was blinded to the treatment techniques and to the control and laser sites, to assure an unbiased evaluation.
The clinical parameters measured at baseline, 5 weeks, and 3 and 6 months included: index 5 , gingival index (GI) 6 , probing pocket depth (PPD), and GCF levels of interleukin (IL)-1β, 7 The clinical observations were ended at 6 months but a further control of the radiological outcome was performed at 12 months.
Laser treatment
At baseline, the contralateral laser sites received LLLT directly after SRP, using the Petrolaser apparatus model SL-202 with 830-nm wavelength. The output was measured to range closely around 100 mW. The laser output power was tested through a digital indicator aperture on the control panel before irradiation. A continuous mode (CW) was used, with slight contact to the tissues with the K30 laser delivery tip, 0.03 cm2 in diameter (supplied with the apparatus). Because the fiber is thin, and consequently produces a high local power density (3 W/cm2), it was decided to scan the involved area to obtain a more homogeneously saturated area and to avoid bio-inhibiting dose ranges. The tip was positioned externally at the base of the pocket according to the PPD, lingually and buccally in slight contact, at a 90 degree angle to the long axis of the tooth, in a sweeping motion all over the area, starting apically and moving upward to the top of the pocket. The selected dose used was based on a previous unpublished pilot study. The irradiated area on each site was ∼1 cm2, and by delivering 3 J of energy in 30 sec, the dose (fluence or energy density) became 3 J/cm2. Three laser sessions were given the first and second weeks, followed by two sessions during the third week, and then sessions were once weekly during the fourth and fifth weeks (a total of 10 sessions for every site). LLLT simulation without starting the laser apparatus was performed for the SRP sites in order to assure patient blindedness.
Immunological assessment
Sampling
From all patients, two GCF samples were taken from the pockets of the selected teeth after removal of the supragingival plaque from the sites to be sampled. These sites were isolated with cotton rolls and gently dried by air syringe before sampling. GCF was collected with prefabricated paper strips (Periopaper, Ora-flow Inc., Plainview, NY). Two strips (2×8 mm in dimension) were inserted into the pockets until resistance was felt and kept there for 30 sec; blood contaminated samples were discarded. GCF volume was measured with a calibrated Periotron 8000 (Oraflow Inc.). The two samples from each periodontal pocket were pooled together and diluted in phosphate buffered saline (PBS) up to 1 mL. After dilution for 15 min, the strips were removed and the samples were frozen at −20°C, pending analysis. 7
Laboratory analysis
IL-1β was measured as described elsewhere. 6 Briefly, a monoclonal antibody to IL-1β (MAB 601, R&D Systems, Minneapolis, MN), diluted 125 times in carbonate buffer, was coated onto microtiter plates (Nunc Maxisorb, NUNC A/S, Roskilde, Denmark) overnight at +4 C. These were washed once with PBS 10.05% polyoxyethylene sorbitan monolaurate (Tweens 20, Sigma Chemical, St. Louis, MO), and blocked with 1% human serum albumin (HSA) for 1 h at room temperature. After four washings, a standard curve (2–200 pg/mL) and undiluted samples (100 mL) were added to the plates. They were incubated at 37°C while shaking for 45 min, and then washed four times. The detection antibody (BAF 201, R&D Systems), a biotinylated polyclonal goat antibody diluted 250 times, was incubated as described previously. After washing, the horseradish peroxidase conjugated streptavidin, diluted 200 times in PBS 10.1% HSA, was added to the plates and incubated in the same manner as the detection antibody. The plates were washed again and the undiluted substrate (TMB, Sigma Chemical) added. The reaction was stopped with 1M H2SO4 after 15 min and the absorbency read at 450 nm in a spectrophotometer (Millenia Kinetic Analyzer, Diagnostic Product Corporation, Los Angeles, CA). 6
Radiographic assessment
Direct intra-oral radiographs were taken at day 0, 6, and 12 months for bone density evaluation by specially designed software (Orion Corporation, Soredex Medical System, Helsinki, Finland).
Radiographic exposure
Standardized reproducible direct digital intra-oral radiographs were taken using a Blue-X imaging machine (Blue Imaging S.R.I., Assago, Italy) with exposure parameters of 65 kV(p)*, 10 mA and 0.02 sec exposure time. The long cone paralleling technique was applied in conjunction with special film holders (Rinn XCP film holder, Rinn Corp., Elgin, IL) and specially designed occlusal radiographic stents constructed for every patient (for standardization of geometric exposure factors). An alginate impression was taken for the investigated arch and poured to obtain a stone cast. Self-curing acrylic resin was mixed and applied at the dough stage on the cast. The Rinn XCP bite block was pressed on the acrylic resin and then the resin was pressed inside the side holes of this bite block. After polymerization of the resin, the template was removed, finished, and polished to be used during radiographic exposure to assure reproducible serial radiographs without any geometric variations.
Image analysis
Digitized images were manipulated using the Digora software system to perform densitometric measurements. As an attempt to assess the bone density changes around each of the studied teeth before and after therapy, three lines were drawn parallel to each other and 1 mm apart, with the first line was drawn just tangential to the lamina dura. The mean of the three lines was calculated and included in the statistical analysis. To determine intra-observer variation, all measurements were performed by one examiner twice at two different sessions with a 2-week interval and calculated as κ index and overall agreement. The examiner was blinded to the performed treatment (Fig. 1).
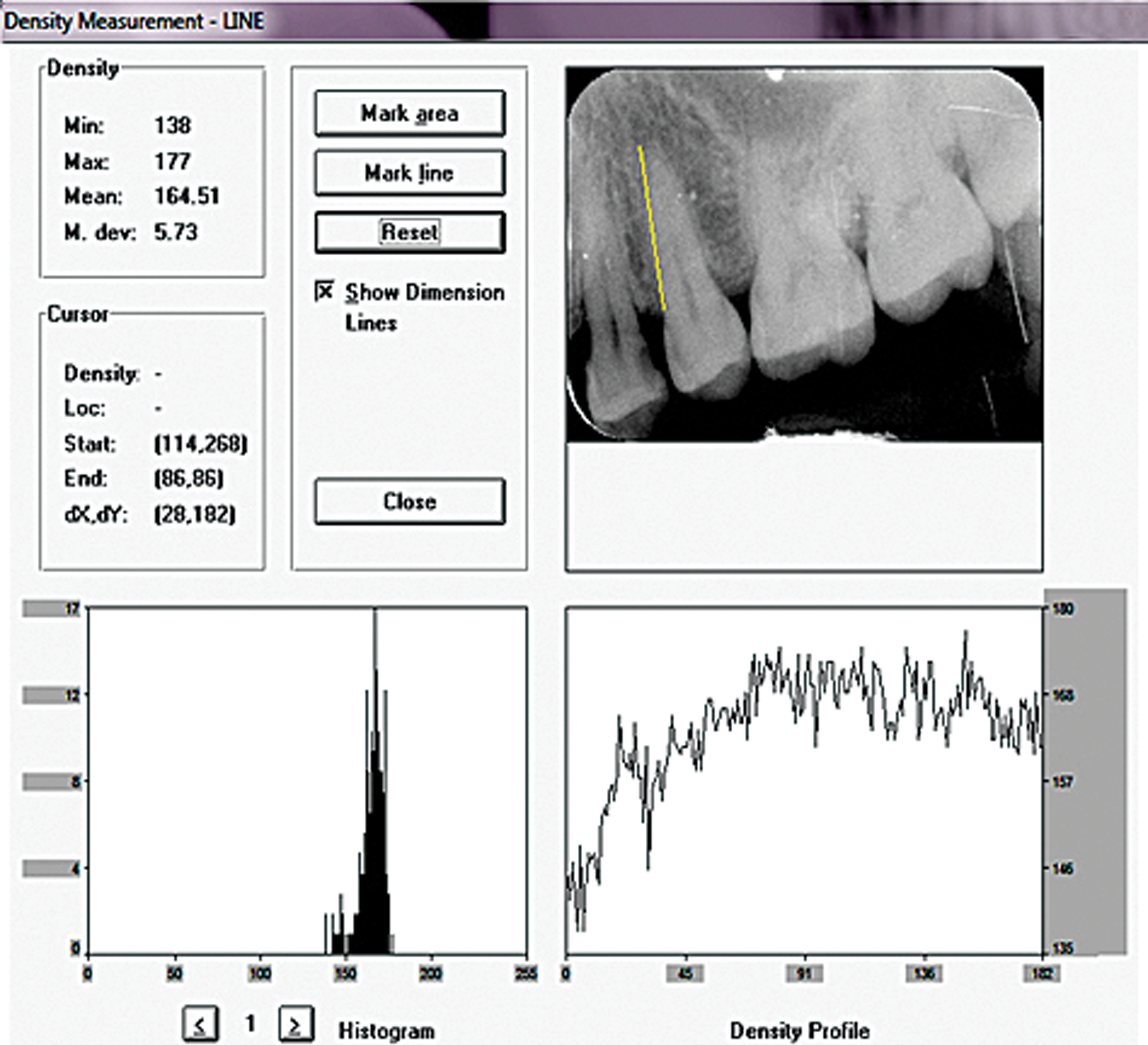
The Digora system.
Statistical analysis
Data are presented as mean and standard deviation (SD) values. Data were explored for normality using the Kolmogorov–Smirnov test. Exploration of data revealed that bone density measurements, as well as the clinical data; PD, GI, PI, and IL-1β data were normally distributed (parametric data). Percentage change data were not normally distributed (nonparametric). For normally distributed data (parametric data), a paired t test was used to compare between the groups and to study the changes within each group of patients. For nonparametric data, a Wilcoxon signed rank test was used to compare between the groups. Statistical analysis was performed with SPSS 16.0® (Statistical Package for Scientific Studies) for Windows (SPSS, Inc., Chicago, IL).
Results
Bone density
The bone density was higher in the laser group at 6 months and further improved at 12 months (Table 1 and Fig. 2).
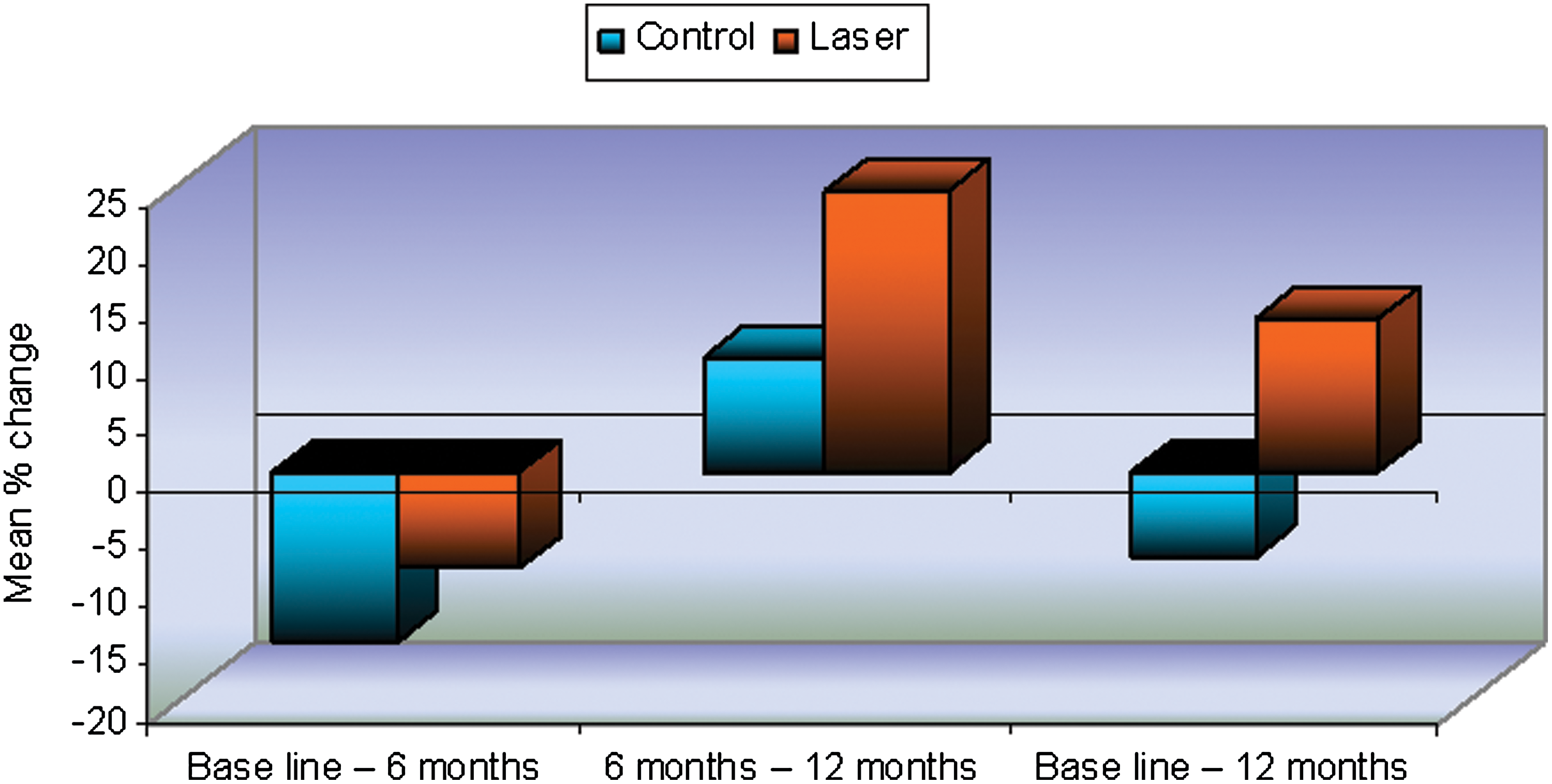
The bone density was higher in the laser group at 6 months and further improved at 12 months.
Significant at p≤0.05.
Pocket depth (PD)
The PD in the laser group improved at 5 weeks and at 3 months, but at 6 month is was the same in both groups (Table 2 and Fig. 3).
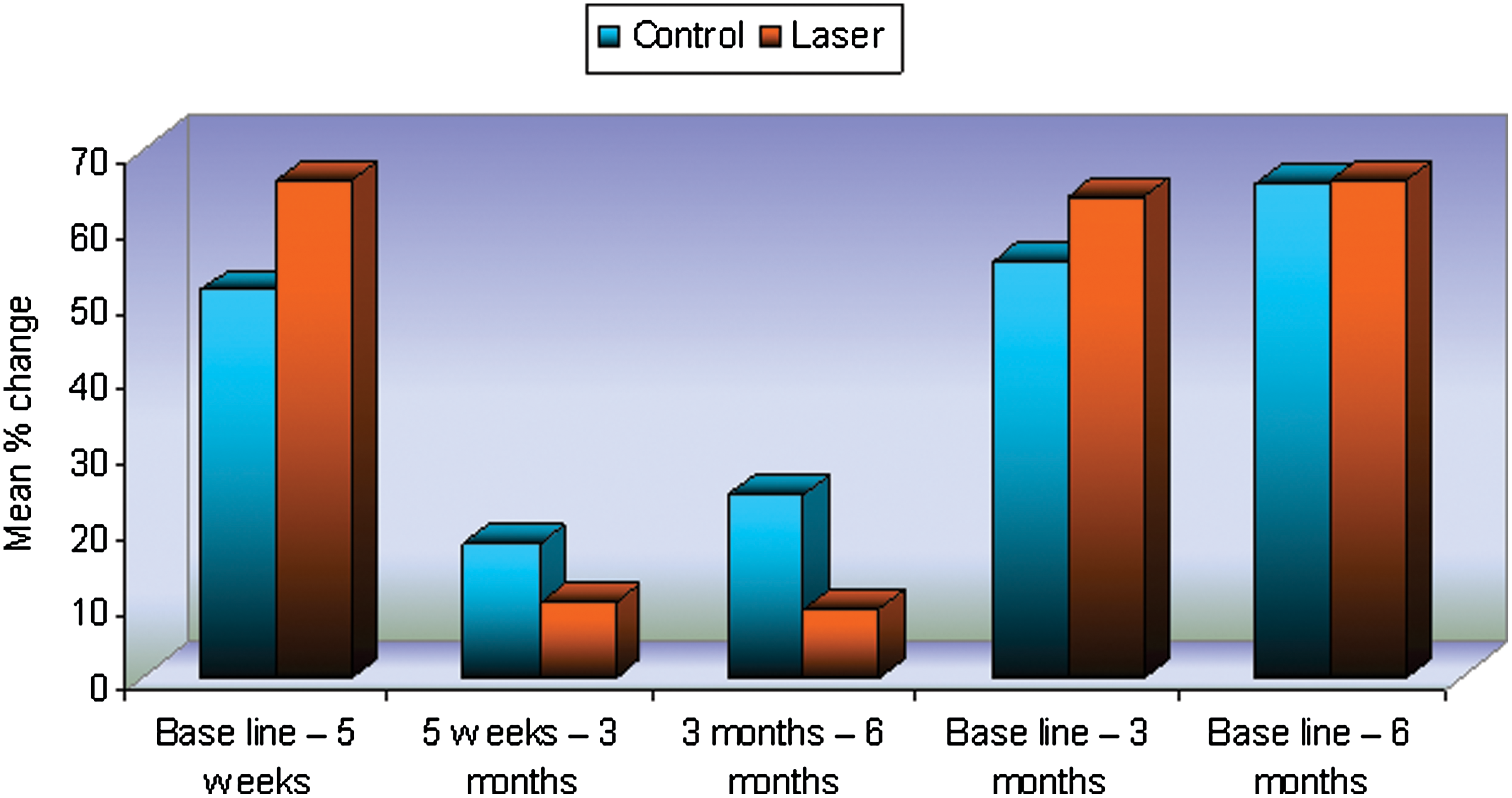
The pocket depth in the laser group improved at 5 weeks and at 3 months, but at 6 months it was the same in both groups.
Significant at p≤0.05.
IL-1β
There was no statistical difference between the control and laser group throughout the experimental period (Table 3 and Fig. 4).
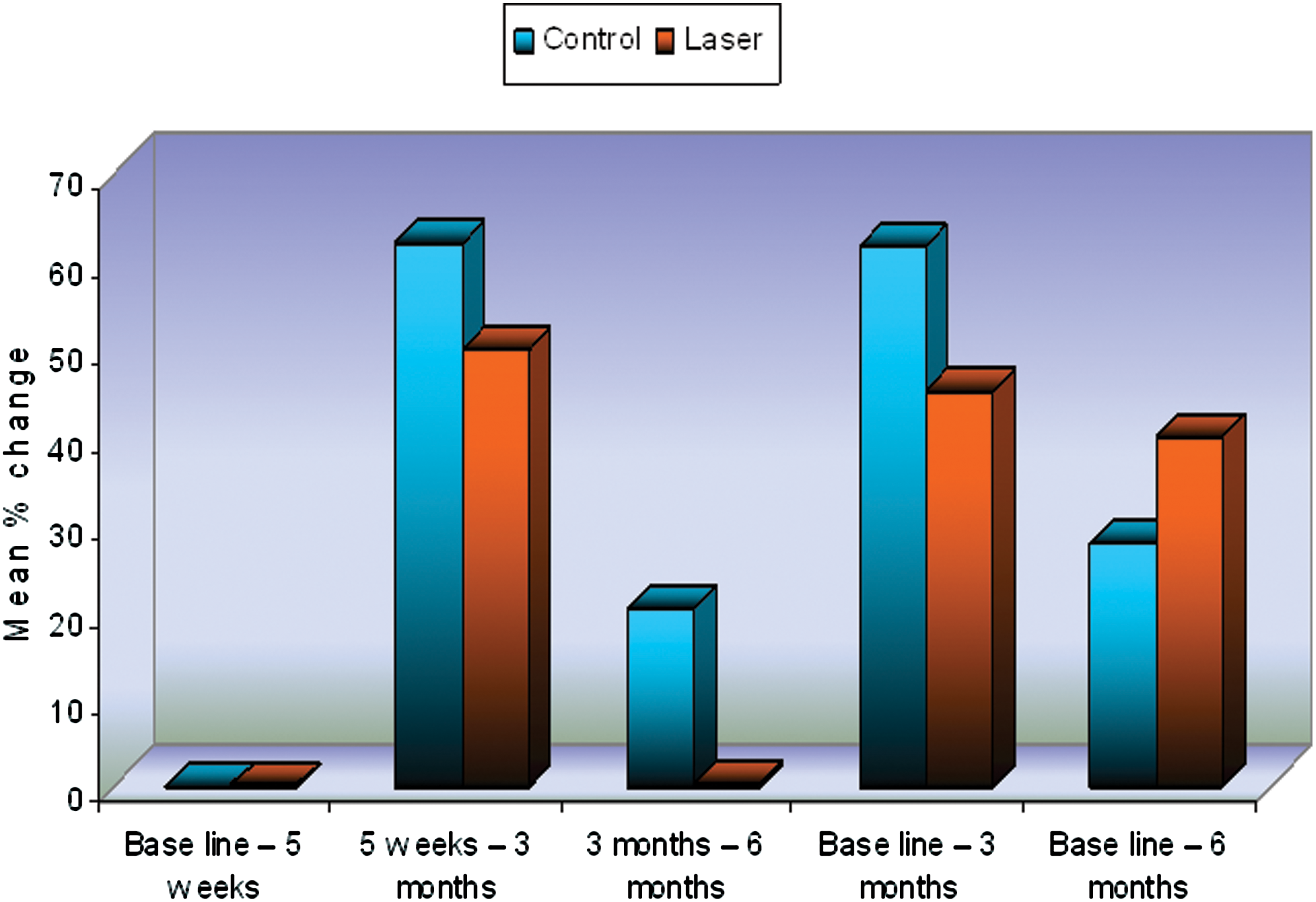
There was no statistical difference between the control and laser groups throughout the experimental period.
GI
The GI did not improve significantly over the control group at any time (Table 4).
Plaque index (PI)
The PI did not reach a significant difference (Table 5).
Discussion
Low level lasers have been used for experimental and clinical studies on bone repair. The 830-nm wavelength is known to be a fair tissue penetration laser, because hemoglobin and water have a low level of absorption for this wavelength. 8 Consequently, 830 nm was chosen as the wavelength for this study. The application of this unit was advantageous as it is a small, easy to use, and fairly inexpensive device.
Upon calculating the total mean bone density changes by pooling the mesial and distal values together, a statistically significant increase was detected in the total mean bone density for the laser group from the periods “6 months to 12 months” and from “baseline to 12 months” than the control group. At 6 months there was a statistically significant decrease in mean bone density for the two groups. This percentage decrease was similar for both groups. The remodeling of bone is more or less complete after 6 months, with or without laser. Early comparisons would, therefore, be more appropriate in order to determine the possible effect of LLLT during the early bone healing process. However, a striking finding was the extended and continued improvement on the laser-treated side up until 12 months.
The literature contains several studies on the influence of LLLT on the stimulation of bone formation, although most studies have focused on bone healing after fractures. Pinheiro and Gerbi 9 have summarized the findings in the dental area. Matsumoto et al. 10 have analyzed the role of cyclooxygenase-2 following bone repair in rats subjected to LLLT. The results suggest that LLLT is able to improve bone repair in the tibia of rats 14 days after surgery as a result of an upregulation for cyclooxygenase-2 expression in bone cells. Xu et al. 11 have investigated the effect of 650 nm, 2 mW, irradiation on mRNA expression of receptor activator of NF-κB ligand (RANKL) and osteoprotegerin in rat calvarial cells.
When the results of changes in PD were compared for the two groups in the present study, the effect of laser was statistically significantly higher in reducing PD values after 5 weeks and 3 months. Moreover, the percentage improvement of PD by time of the laser group was significantly higher at the periods from baseline to 5 weeks, and baseline to 3 months than that of the control group. These results are in accordance with those of Qadri et al. 7
No statistically significant difference between the two groups regarding the GI degree was detected; although there was a trend toward a positive value in the laser group. This finding is different from that of Qadri et al. 7
The two groups in our work were initially not statistically different regarding the mean values of the PI, but when the changes by time were compared between the two groups, the percentage decrease of PI of the laser group was higher than that of the control group after 5 weeks, 3 months, and 6 months. Again, this finding was also in agreement with that of Qadri et al. 7
There was no statistically significant difference between the initial IL-1β values of the two groups to assure that any changes would be attributed to the effects of the therapy and not to variations in the initial start values. It was noticed that in both groups, there was reduction of IL-1β levels but the difference was not statistically significant. This finding was in agreement with that of Nomura et al. 12 and Qadri et al. 7
The selection of the optimal laser and treatment parameters for LLLT was another major target of this study because of the lack of adequate studies concerning these parameters. The parameters used in this study seem to have been within the “therapeutic window” of dosage but not necessarily optimal. Recent investigators being successful in finding this window are Aykol et al. 13 and Pejciç et al, 14 . Aykol 13 included smokers as well as nonsmokers in the trial and results in both groups were equally positive. Three sessions of LLLT were performed during the first week after SRP, 808 nm, 4 J/cm2. At all times of measuring, the two laser groups had better scores than the conventionally treated patients. Pejcic used 670 nm and 10 daily sessions of LLLT after SRP (18 J/cm2 for 5 days, 12 J/cm2 for the consecutive days) and had a significant effect on PI, bleeding on probing, and GI. An effect on GI was not obtained in the present study. Obradoviç et al. 15 investigated the efficiency of LLLT as an adjunctive tool in reduction of periodontal inflammation and destruction in diabetic patients. Two hundred participants were divided into four groups (50 participants in each group): groups 1 and 2 [participants with diabetes mellitus (DM) type 1 and periodontal disease], groups 3 and 4 (participants with DM type 2 and periodontal disease). During 5 consecutive days, soft and hard deposits were removed and periodontal pockets cleaned in each group, and 808 nm, 5 mW; 14 min/day applied in the laser groups 1 and 3. Results showed a significant decrease of PD index after therapy in each investigated group compared to the values before therapy.
Few clinical studies have targeted the immunological response to LLLT of patients with periodontal disease. GCF is one of the markers of gingival inflammation. 16 Qadri et al. 7 used a similar approach as ours and found that all clinical parameters were improved by the adjuvant use of LLLT. However, there was no significant difference in elastase or IL-1β between the laser and the control group. The total amount of matrix metalloproteinase (MMP)-8 increased on the placebo side but was slightly lower on the laser side, although not reaching significant values. As the immunological results did not improve significantly, whereas clinical parameters did, as in the present study, the actual mechanisms behind the positive clinical observations remain to be elucidated. Aykol et al. 13 measured TGF-ß1 levels and the ratio of MMP-1 to tissue inhibitor of metalloproteinase (TIMP)-1 decreased significantly in both of the laser groups at 1, 3, and 6 months after periodontal therapy. Basic fibroblast growth factor (b-FGF) levels significantly decreased in both groups at the first month after the treatment, then increased at the third and sixth months. It is obvious that the effects are dose and wavelength sensitive.
The minimum number of sessions to obtain a positive effect of LLLT is still not known. The present study used 10 sessions, equal to that of Pejciç et al., 14 although the latter study treated every day. Qadri et al. 7 used one session per week during 6 weeks and Aykol et al. 13 used only three sessions, concentrated to the first week after SRP. According to Pinheiro and Gerbi 2006, 9 LLLT is most effective if the treatment is administered at early stages when high cellular proliferation occurs.
Conclusions
Compared with SRP alone, LLLT in combination with SRP further improved bone density at 6 and 12 months and reduced PD at 6 months. The use of LLLT did not, however, significantly change the gingival and plaque indexes or the IL-1β levels. Further investigations are warranted to confirm the usefulness of LLLT in periodontal therapy and to identify the optimal parameters.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.