
Abstract
Introduction
Growth factors have an essential role in the control of collagen breakdown, formation of new fibroblasts, stimulation of osteoblast activity, formation of new matrix components, and blood vessels. Therefore, the release of growth factors from both injured cells and inflammatory cells seems to be an important part of the repair process. 16
The basic fibroblast growth factor (bFGF), an endogenous polypeptide growth factor expressed by osteoblasts, has numerous biologic activities that include stimulation of cell growth, migration, angiogenesis, wound healing, tissue repair, differentiation, and morphogenesis. 17,18 It has been demonstrated that bFGF stimulates the proliferation of various cell types including fibroblasts, 19 osteoblasts, 20 cementoblasts, 21 and endothelial cells, 22 which are crucial cells for periodontal regeneration. Insulin-like growth factor (IGF) is a multifunctional peptide that may enhance periodontal regeneration by stimulating formation of soft tissue collagen, bone, and cementum. 23 In bone cell systems, IGF stimulates proliferation of pre-osteoblasts as well as differentiation of osteoblasts, including type I collagen synthesis. 24,25 Thus, IGF increases both the number of cells synthesizing bone and the amount of extracellular matrix deposited by each cell. The IGFs bind to specific receptors and their function is regulated at one level by the presence of insulin growth factor-binding proteins (IGFBPs), which function as carrier proteins in biological fluids, mediate the transport of IGFs from the vascular area, and increase their half-lives. 26
In our previous study, it was demonstrated that low-level laser irradiation of gingival fibroblasts enhanced the secretion of growth factors. 27 LLLT may also have an effect on osteoblasts by enhancing the release of various growth factors. However, little is known about the mechanisms of biostimulation of osteoblasts. Therefore, the aim of the present study was to investigate whether LLLT stimulates release of bFGF, IGF-I, and receptor of IGF-I from osteoblasts, and whether the effect of laser on osteoblast cells depends upon dose.
Materials and Methods
Isolation of mesenchymal stem cells (MSCs) and osteogenic differentiation
Unfractionated fresh bone marrow (10 mL) was obtained by iliac crest aspiration from donors aged 25–55 years. The donors were either clinically healthy or in remission from malignancy (off protocol for chemotherapy or radiotherapy), and undergoing marrow harvest for future autologous bone marrow transplantation. Ficoll method was used to isolate human mononuclear cells from these marrow aspirates. Briefly, 10 mL of marrow was added to 20 mL of low-glucose Dulbecco's Modified Eagle's Medium (L-DMEM), which contains 10% fetal bovine serum (FBS). The mixture was centrifuged to pellet the cells and remove the fat layer. Cell pellets were then re-suspended and fractionated on a density gradient generated by centrifuging a 70% Ficoll solution at 13.000 g for 20 min. The mononuclear cells–enriched low density fraction was collected, rinsed and cultured at 1 x 105 nucleated cells per 25 cm2 culture flasks. The flasks contained DMEM medium supplemented with 10% FBS 2 mmol/L
MSCs were incubated in the control medium for 1 day to adhere the cells to the flasks, and the media were then placed in the osteogenic medium: L-DMEM containing 10% fetal bovine serum, 100 nM dexamethasone, 10 mM sodium β-glycerophosphate and 0.05 mM ascorbic acid. The media were changed every 3 days and osteogenic differentiation was assessed by von Kossa staining 2 weeks after initial osteogenic differentiation. The study protocol was approved by the Internal Review and Ethics Board at the Gulhane Military Medical Academy.
Laser irradiation
A diode laser (BTL-2000 Benešov, made in the Czech Republic) with a continuous wavelength of 685 nm was used in the study. An optical fiber was fixed to a distance of 1 cm above the cells and used to deliver the laser beam on an area of 1.75 cm2. The power on the laser device display, the duration of exposure, the power density, and the energy dose were 25 mW, 140 sec, 14.3 mW/cm2, and 2 J/cm2, respectively.
Two study groups and a control group were formed. Cells were irradiated only one time in the first study group (single dose group) and twice with a 24-h interval in between in the second study group (double dose group). Laser irradiation was not performed in the control group. Twenty-four hours after laser irradiation, the media in culture plates were collected and used to determine the cell viability, proliferation, and the level of bFGF, IGF-I, and IGFBP3 released from osteoblasts.
Cell viability and proliferation
After laser irradiaton, proliferation and viability of osteoblasts were determined using metabolic XTT assay (Biological Industries, Beit-Haemek Ltd., Kibbutz Beit Haemek, Israel). Viable cells convert XTT to formazan, which is a colored product and is proportional to the number of vital cells. Cells were incubated with a final concentration of 200 μg/mL XTT and 5 μM reducing agent phenazine methosulphate (PMS) for 4 h at 37°C. Cell culture supernatants were placed in 96-well plates and the absorbance was read at 450 nm. Net absorbance values were calculated by subtracting the average absorbance values of blank wells from seeded wells. The proliferation rate was calculated as the percentage of absorbance values compared to control cells. Duplicates of 24 wells were used for each assay.
Assay for bFGF, IGF-I, and IGFBP3
Commercially available kits were used to determine the level of bFGF (bFGF ELISA kit; RayBiotech, GA), IGF-I (Non-Extraction IGF-I ELISA kit; Diagnostic Systems Laboratories, TX), and IGFBP-3 (IGFBP-3 ELISA; DSL-10-6600 ACTIVE®, Oxon OX25 5HD UK) using materials and techniques previously described. 27
Statistical analysis
SPSS 10.0 (SPSSFW, SPSS, Chicago, IL) statistical program was used for the statistical analysis. The differences between the groups were assessed by Mann–Whitney U test and the differences were considered to be significant when p<0.05.
Results
The comparison of bFGF between groups revealed significant increases for single dose and double dose groups compared to the control group (p<0.05 and p<0.01, respectively). bFGF levels were also significantly higher in the double dose group compared to the single dose group (p<0.01) (Fig. 1).

Effect of single dose and double dose (24-h interval) laser irradiation (140 sec, 2 J/cm2) on the release of bFGF from osteoblasts. *Significant increase compared to control group (p<0.05). †Significant increase compared to control group (p<0.01). ‡Significant increase compared to single dose group (p<0.01).
When IGF-1 was compared, significant increases were found for single dose and double dose groups compared to the control group (p<0.01). IGF-1 level was also statistically higher in double dose group compared to the single dose group (p<0.05) (Fig. 2).
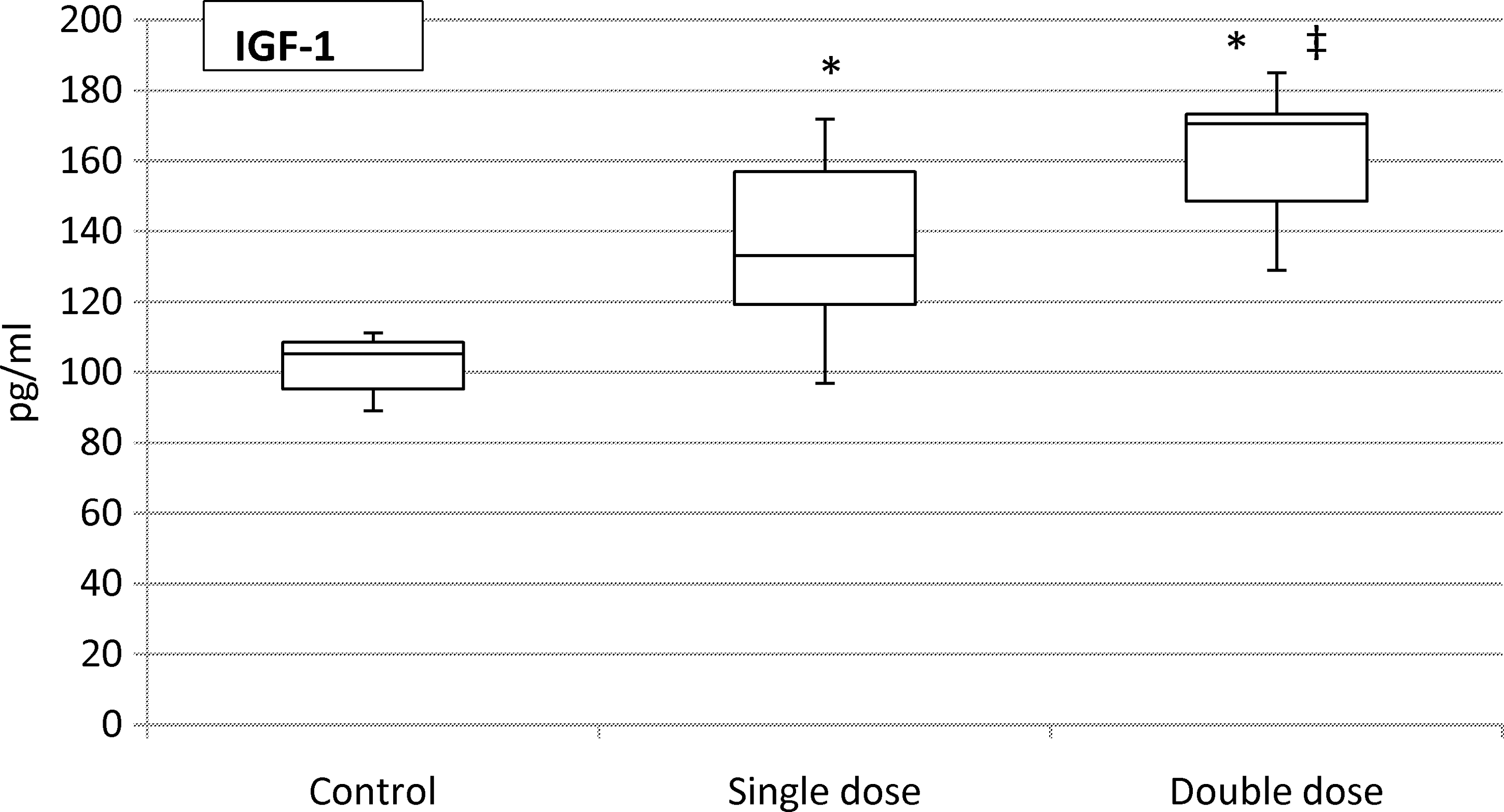
Effect of single dose and double dose (24-h interval) laser irradiation (140 sec, 2J/cm2) on the release of IGF-1 from osteoblasts. *Significant increase compared to control group (p<0.01). ‡Significant increase compared to single dose group (p<0.05).
The comparison of IGFBP3 levels between groups showed significant increases both for single and double dose groups compared to the control group (p<0.01). When the laser- treated groups were compared to each other, significant decrease was detected for IGFBP3 in the double dose group (p<0.01) (Fig. 3).
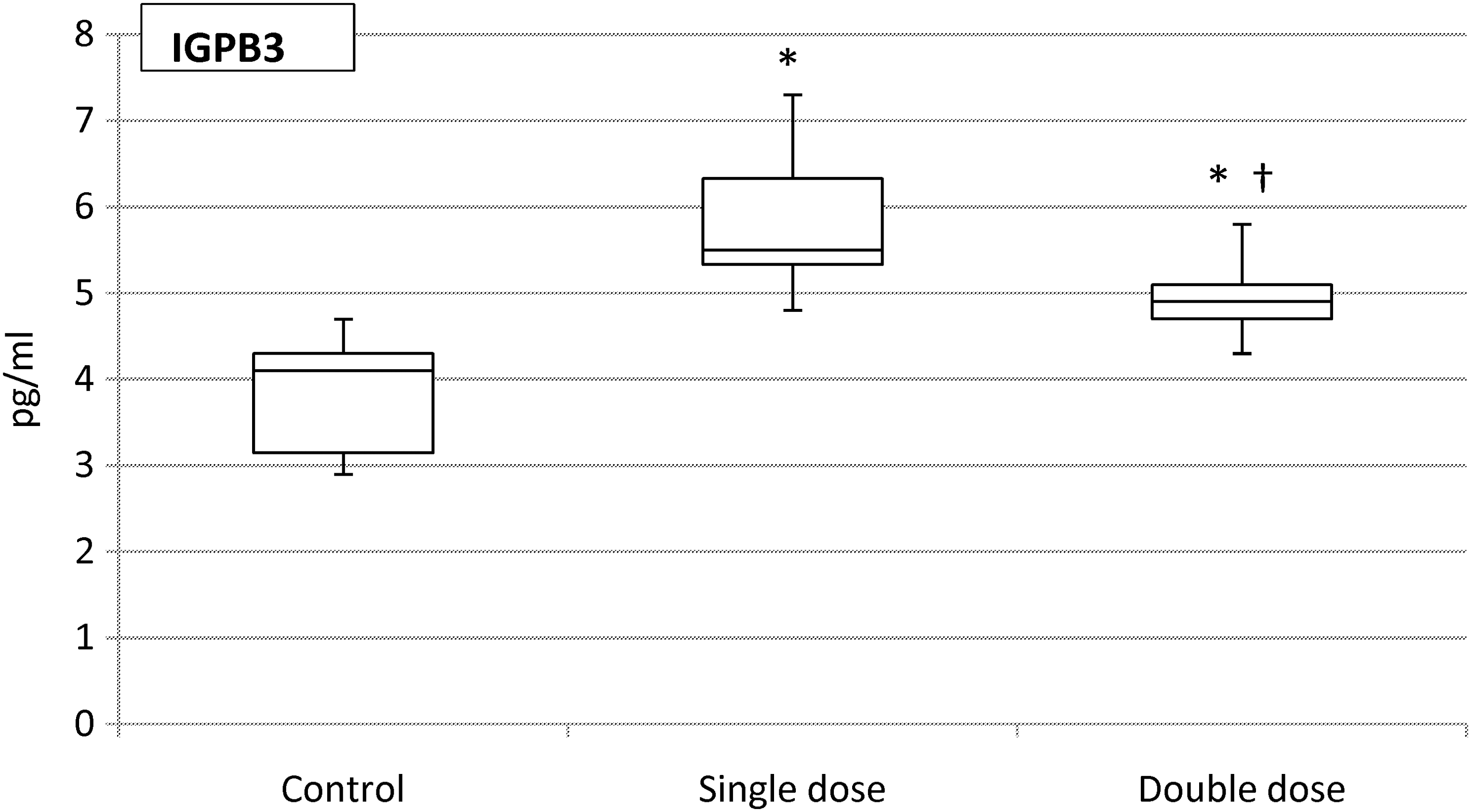
Effect of single dose and double dose (24-h interval) laser irradiation (140 sec, 2 J/cm2) on the release of IGPB3 from osteoblasts. *Significant increase compared to control group (p<0.01). †Significant decrease compared to single dose group (p<0.01).
Proliferation of osteoblasts increased in all the study groups. The rate of proliferation was determined to be significantly higher in the laser-treated groups than in the control group (p<0.05). Cell viability was 118.2% for the single dose group and 110.8% for the double dose group. This difference was not significant between the single and double dose groups (Fig. 4).
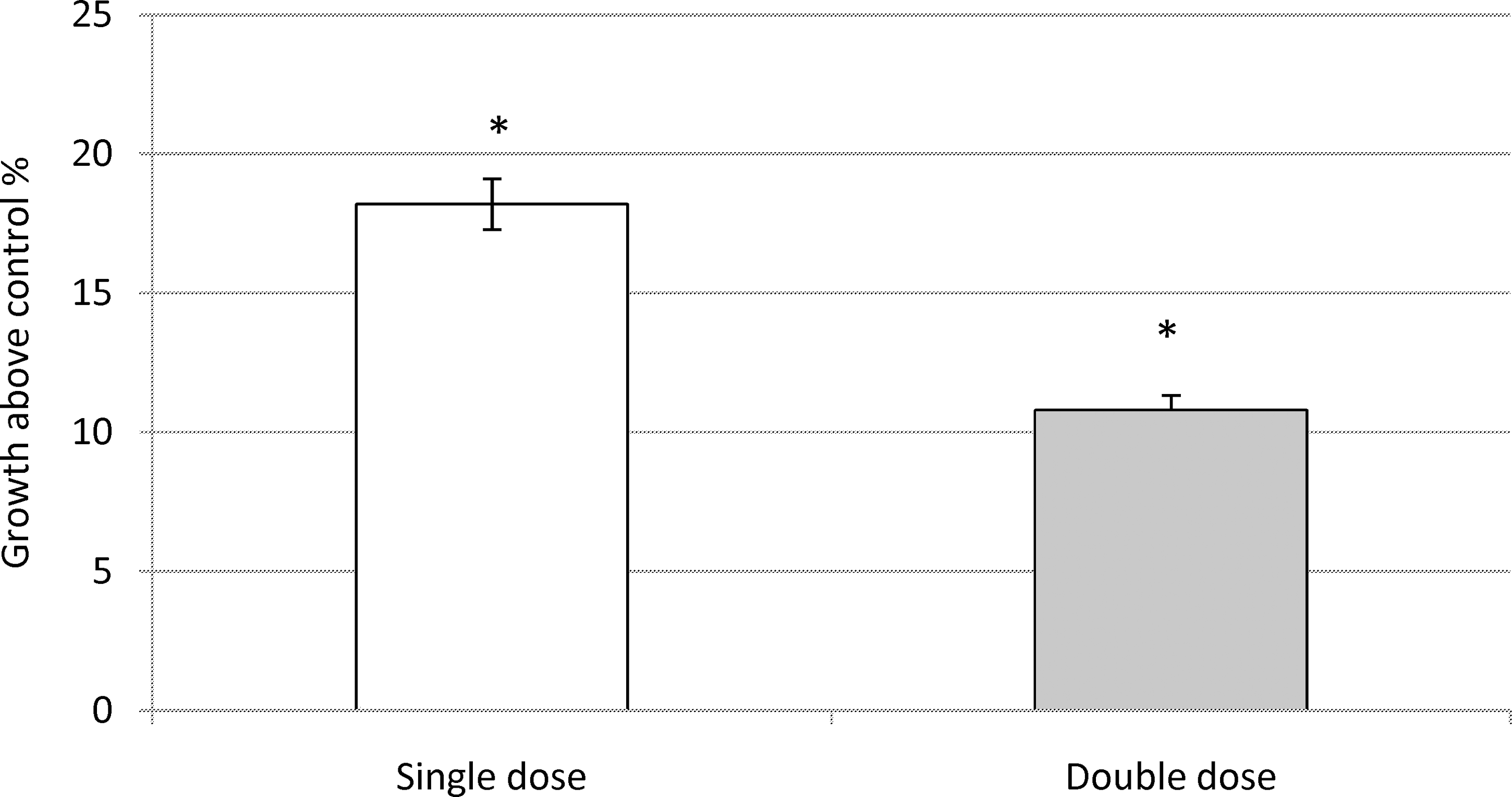
Effect of single dose and double dose (24-h interval) laser irradiation (140 sec, 2 J/cm2) on the osteoblast viability. *Significant increase compared to control group (p<0.05).
Discussion
Growth factors are essential for many biological events associated with the turnover, repair, and regeneration of periodontal tissues. 19,21,23 bFGF and IGFs may be presumed to act as autocrine or paracrine stimulators on bone cells. 28 In some studies, bFGF and IGF-1 have been suggested to promote periodontal regeneration by stimulating the formation of mesenchymal tissues including collagen, bone, and cementum. 23,29 It is also known that IGF stimulate not only the proliferation of pre-osteoblasts but also the differentiation of osteoblasts. 24,25 Similarly, the mitogenic and angiogenic features of bFGF suggest that it may play an important role in wound healing. 17,18 In the present study, we investigated the possible effects of LLLT on bFGF, IGF-1, and IGFBP3 expressions by osteoblasts.
In several studies, LLL energy was demonstrated to enhance osteoblast proliferation. 9 –12 Conflicting data have been reported about the number of laser applications adequate for proliferation of osteoblasts. In the present study, the effects of single and double dose laser irradiation (140 sec, 2 J/cm2) were compared. Higher rates of osteoblast proliferation were detected for both groups in comparison to the control group. Consecutive laser application caused numerically less proliferation, but this difference was not significant when compared with the single dose group. The results of one dose group are parallel to the findings of Ozawa et al. 9 and Arisu et al. 13 who demonstrated higher proliferation rates of osteoblasts after LLLT using diode and Nd:YAG lasers respectively. However, Stein et al. 28 found no significant differences between the control group and the sample exposed to a single dose of 2 J/cm2 for 1 min using diode laser. The same conflicting situation exists for the double dose group. Dörtbudak et al. 11 demonstrated that repeated irradiation of osteoblasts (60 sec, 1.6 J/cm2) resulted in increased proliferation compared to control group as it did in our study. Whereas Kim et al. 29 demonstrated that cell proliferation was significantly suppressed by 13.6%, 11.2%, and 7.5% in the irradiated groups of 1.5, 3, and 5 J/cm2 energy intensities, respectively, compared to that of the control cells. These inconsistent reports may be attributed to the wide variety of laser setups and types, irradiation time, and distance of the fiber from the specimen used in different studies.
Stein et al. 28 reported that osteoblasts irradiated with laser energy at 1 J/cm2 demonstrated increased cell proliferation, whereas laser energy at 2 J/cm2 suppressed cell proliferation after 24 h. Significant differences were reported between the laser groups but the laser groups were not significantly different from the control group. These findings suggest that both stimulation and inhibition of the osteoblast proliferation is likely to be caused with the same laser in the same cells. On the other hand, according to the present findings, laser energy at 2 J/cm2 may be suggested to have a positive biostimulation effect on osteoblasts and not to cause cell damage. The discrepancy between our present data and the findings of Stein et al. 30 may be explained by the differences in cell lines in terms of sensitivity to various wavelengths and energy densities as demonstrated by Renno et al. 31 Studies characterizing cellular proliferation and differentiation stimulated by laser irradiation address cytokine or growth factor release as regulators. Saracino et al. 32 reported that superpulsed laser irradiation on osteoblastic-like cells resulted in increased expression of transforming growth factor-beta 2(TGF-β2), bone morphogenetic protein (BMP)-4 and BMP-7 which are members of the TGF-β superfamily. The present study demonstrated that low-level laser irradiation (2 J/cm2) also increased the production of other growth factors such as IGF-1 and bFGF from osteoblasts. Similarly, increase in IGF-1 protein and gene expression was reported by Shimizu et al. 33 using low intensity Ga–Al–As laser irradiation (3.82 J/cm2).
IGFBPs have important functions as carrying proteins in biological fluids and mediating the transport of IGFs from the vascular space. 26 In a previous study, it was demonstrated that LLLT of fibroblasts increased IGFBP3 production. 27 A new finding of the present study was that laser irradiation at a wavelength of 685 nm, with 140 sec exposure time, and 2 J/cm2, also increased the production of IGFBP3 from osteoblasts.
To our knowledge, this is the first study to evaluate whether LLLT could stimulate the release of bFGF and IGFBP3 from osteoblasts. Our findings are in line with the results of other researchers, and suggest that LLLT may accelerate wound healing because of the stimulatory effects on osteoblast proliferation. The biostimulatory effect of LLLT may be associated with the enhanced production of growth factors such as IGF-1, bFGF, and IGFBP3 from osteoblasts. LLLT may play an important role in wound healing and regeneration by enhancing the production of the growth factors. As the regeneration of bone tissue is an important aspect in regenerative therapy, the biostimulatory effects of LLLT could prove an adjunctive treatment in the repair of osteogenic defects. Further in vivo and in vitro investigations are needed to understand the mechanisms leading to stimulation of osteoblasts and to evaluate whether LLLT might be beneficial in regenerative periodontal therapy.
Footnotes
Acknowledgments
The study was supported by a grant from Gulhane Military Medical Academy Research Center, Ankara (Research No: AR-2004/16).
Author Disclosure Statement
No conflicting financial interests exist