
Abstract
Introduction
Although some researches have reported clinical data, primary and secondary caries progression has mainly been assessed in vitro, using decalcifying solutions or bacterial culture. 3 Therefore, the artificial caries models, both in laboratory and in situ, 4 have been widely used for the purpose of verifying the efficacy of therapeutic and preventive procedures. In the laboratory, the process of lesion formation is faster than it is in the mouth: therefore, an advantage of these models is that much can be learned in a short period of time. 3 Many laboratory studies have used the pH variation model. 1,5 These models can produce a continuous process of caries formation that ranges from an imperceptible white spot to cavity formation, which enables one to investigate the etiology and prevention of caries lesions.
In turn, the use of lasers offers a new possibility for improving caries treatment and prevention techniques. Specifically, the Nd:YAG laser seems to modify the crystalline structure of enamel, making it more acid resistant, and thus, making it difficult for demineralization lesions to develop. 6,7 Nevertheless, argon laser irradiation can also be used to modify hydroxyapatite and make it more resistant to dissolution by acid. 8,9 In spite of the preventive effect of the two lasers with respect to isolated results, alterations to the enamel surface are different for each type of laser. Whereas the Nd:YAG laser causes the prisms to melt and fuse, 10 the argon laser produces a granular surface with innumerable microporosities, which appear to function as mineral deposits that serve to defend the structure against acid challenges. 11 However, the real isolated effect of the laser on the dental structure for caries prevention is not yet clear, as various studies use fluoride associated with the laser and vary the irradiation parameter.
In view of the importance of discovering methods for preventing caries disease, the aim of this study was to investigate the effect of Nd:YAG and argon laser irradiations on enamel demineralization after two different models of inducing artificial caries lesions.
This study started from the null hypothesis that there is no significant difference among the studied groups with regard to the area of enamel demineralization.
Materials and Methods
Sample preparation
This research protocol was approved by the local Research Ethics Committee
For the pulsed Nd:YAG laser (λ=1064 nm), the enamel surface of the sample was covered with graphite, 10 and irradiated with the parameters of 60 mJ, 15 Hz repetition rate, 47.77 J/cm2, 100 μs pulse duration, without contact for 30 sec per sample on all exposed area of enamel. For the continuous argon laser (λ=488 nm), the surface was covered with a carbopol-based gel and red coloring (Whiteness HP, FGM, Curitiba, PR, Brazil). Previously, the absorption spectrum in the infrared field had been measured by Fourier transform infrared spectroscopy (FTIR), which verified a wavelength of 575 nm. The parameters for the argon laser were: 250 mW, 12 J/cm2, for 48 sec. After the surface treatment procedures, the hemifaces were washed with jets of air/water and stored in individual Eppendorf tubes containing de-ionized water, in an oven at 37°C, for 24 h.
Induction of artificial caries
To standardize the area of exposure to the in vitro demineralization models, all the hemifaces were covered with varnish (Colorama, São Paulo, SP, Brazil), leaving only a pre-established area (3 mm in the cervical-occlusal direction and 3 mm in the mesio-distal direction). A digital caliper (Mitutoyo, Suzano, SP, Brazil) was used to check the measurements.
Each of the enamel surface treatment groups was subdivided into two groups, with different ph cycling models. In Model 1, the hemifaces of each group (14 hemifaces per group) were subjected to the dynamic demineralization and remineralization cycling model, 12 which consisted of daily immersion in a demineralization solution (2.0 mmol/L of calcium, 2.0 mmol/L of phosphate, and 75 mmol/L of acetate in pH 4.5) for 6 h, after washing in de-ionized water, drying with jets of air, and immersion in remineralization solution (1.5 mmol/L of calcium, 0.9 mmol/L of phosphate, 150 mmol/L of potassium chloride, and 20 mmol/L of tris buffer at pH 7.0), for 18 h at 37°C, during 14 days. The two solutions, demineralization and remineralization, were changed daily, the quantity being standardized at 30 mL per group.
In Model 2, the hemifaces of each group (14 hemifaces per group) were subjected to the model of chemical induction of demineralization for 48 h 13,14 (2.2 mmol/L calcium chloride, 2.2 mmol/L sodium phosphate, and 50 mmol/L of acetic acid, in pH 4.5, adjusted with sodium hydroxide) which consisted of immersion in demineralization solution at 37°C, changed after 24 h.
After both models, a white stain could be clinically observed on the enamel.
After the end of pH cycling models in vitro, the fragments were prepared for evaluation under polarized light microscopy.
Obtaining of histologic slices
The hemifaces were fixed with wax (Kota, São Paulo, SP, Brazil) in an acrylic matrix measuring 4 cm high×4 cm wide×0. 8 cm thick, and afterwards cut into slices with a diamond disk coupled to a cutting machine, in the enamel-dentin direction, under cooling with de-ionized water, at a speed of 150 rpm. The slices were manually worn with 600 and 1200 grit water abrasive papers to a final thickness of 60–100 μm, which was gauged with a digital caliper.
Analysis under polarized light microscopy with interferential contrast
The slides were mounted with de-ionized water and observed under an optic microscope (DMRHC, Leica, Wetzlar, Germany), at 5× magnification and equipped with an interferential contrast system in which the areas of demineralization in enamel were analyzed. The images were recorded with the aid of a digital camera (model 990, Nikon, Tokyo, Japan) coupled to a microscope, and afterwards analyzed by means of the Software VIM-I (Engineering Faculty, PUCRS, RS, Brazil) (Fig. 1), in which the area of the caries lesion was measured in mm2. To verify the intra-examiner reproducibility, from each group an image was selected, which was measured five times, once per week, during 3 weeks. The measurements were subjected to analysis of variance (ANOVA) to determine whether there was difference between the days evaluated, or equality between the days being determined by p>0.05. The examiner did not know to which groups the specimens belonged.
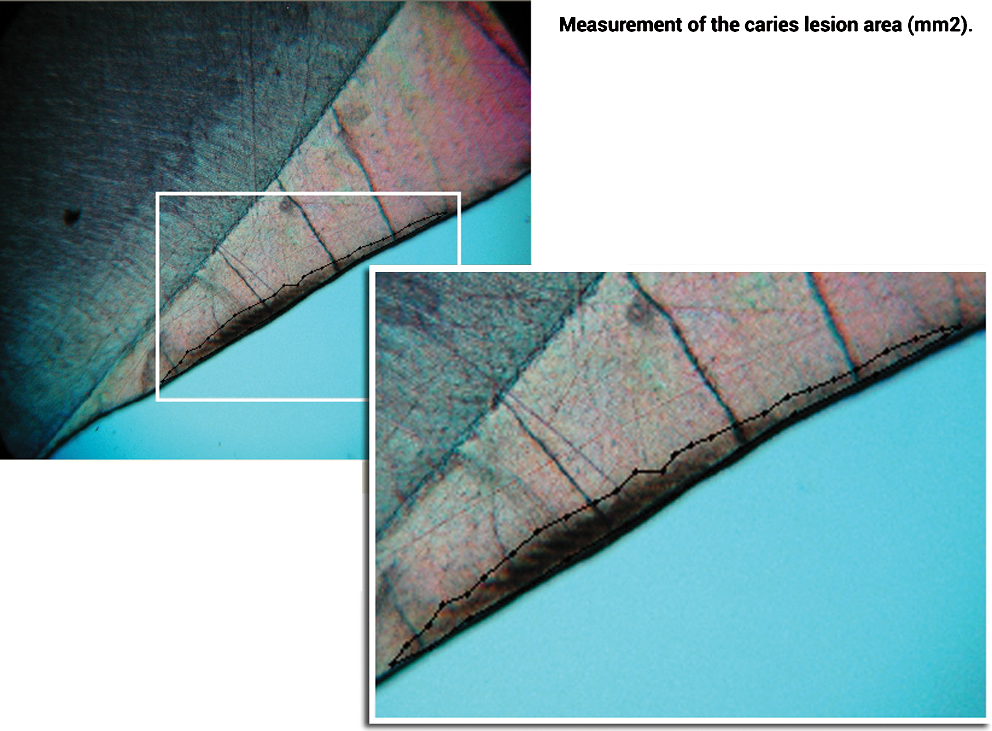
Measurement of the caries lesion area (mm2) by means of VIM-I software. The demarcated area corresponds to the area of enamel demineralization.
Eleven samples were analyzed per group. Some samples were lost because of the difficulty of the methodology. For the analysis under polarized light microscopy, the slices need to be manually worn with 600 and 1200 grit water abrasive papers to a final thickness of 60–100 μm. Some samples were broken during this process. After this, the measurements obtained were analyzed with the Shapiro–Wilk normality test, followed by the statistical tests of ANOVA with two fixed factors (surface treatment and cycling method) and Tukey (p<0.05) (Statistix for Windows 8.0, FL).
Results
The intra-examiner calibration indicated an acceptable reproducibility (p=0.98).
The values obtained in the measurement of enamel demineralization are shown in Table 1. One observes that the argon laser obtained the smallest mean demineralization area in the cycle of 14 days. In turn, in 14 days, the Nd:YAG laser presented no statistical difference in comparison with the control group without treatment.
Means followed by different letters differ among them by ANOVA and Tukey (p<0.05).
Table 2 shows the comparison of the general performance of the studied groups when subjected to the different pH cycles. It is possible to observe that the argon laser presented a smaller demineralization area, but did not differ statistically from the Nd:YAG laser, considering all the studied groups.
Means followed by different letters differ among them by ANOVA and Tukey (p<0.05).
There was no statistical difference in the demineralization area between the pH cycling of 48 h and that of 14 days (Table 3).
Means followed by the same letter do differ among them at the level of significance of 5%.
Discussion
According to the results obtained, the initial hypothesis of this study, in which there would be no differences among the groups for the enamel demineralization area, was rejected.
Because of the ease of clinical application of the technique presented in this research, it could be suggested that the immediate clinical implications are the preventive irradiation of recently erupted permanent teeth and treatment of the enamel surface at restoration margins.
Frequent change of restorations has been a problem in dental practice. This restorative cycle ends up enlarging preparations, weakening the dental structure, and increasing the need for more complex treatments. Studies on the frequency of changing restorations in dental offices show that the occurrence of secondary caries is the main reason for replacing them. 15 The defects in restorations present a relationship with the presence of secondary caries, probably because of being a place of bacterial accumulation; however, it has been proven that the lesion starts externally at the tooth–restoration interface, a place capable of being diagnosed, controlled, and inactivated. 16,17
Susceptibility to caries is greater soon after eruption of the tooth and diminishes with age. 18 The enamel surface of unerupted teeth presents more porosity and less mineral content than that of teeth that have already erupted. 19 Kotsanos and Darling 18 evaluated, in vitro, the susceptibility to caries of unerupted teeth and others that had already erupted, with different times of exposure to the oral medium. The results indicated a reduction in the occurrence of caries lesions proportional to the increase in exposure time of the tooth to the oral medium, particularly in the first 3 years post-eruption. Because of this great variability, it was decided to use included third molars indicated for extraction in the research, and conduct an in vitro study.
In this study, the laser used was not associated with fluoride, as the focus of this experiment was to observe if laser light only would be capable of preventing the development of the lesions. In the same way as fluoride, the laser cannot be considered an absolute antidote to the establishment of caries disease, but rather a new preventive possibility. In the present study, there was lesion formation in all the groups subjected to the artificial caries induction models in vitro, as was the case in studies with fluoride, which in isolation did not prevent the disease, but efficiently reduced the speed of its progression. 20,21 In this research, only irradiation of the surface with the proposed lasers was performed. It is also known that fluoride needs to be constantly available in order to avoid or retard the development of carious lesions. Nevertheless, although there are no populational follow-up studies of individuals with enamel surfaces irradiated by Nd:YAG or argon lasers without fluoride, it is pointed out that the treatment here proposed can be considered coadjuvant to the strategies of access to fluoride, such as dentifrices and professional topical application, which present effective results in reducing the prevalence of dental caries. 22 –24
As regards the artificial process of caries formation, this can be performed using two methods: one involving the use of the oral microbiota, 25 and the other using a chemical model. 12,26
Both have been widely used for inducing 27,28 the formation of initial lesions, particularly white stains, secondary caries around restorations, root caries, caries in pits and fissures, and caries in dentin.
Among the chemical models most used in vitro, there are variations with respect to the duration of each stage of the acid challenge, the number of days, and the formulation of the solutions used. Because of this diversity of demineralization, induction models in vitro and the difficulties of performing in vivo studies, such as cost, time, and availability of patients, it was decided to compare the chemical methods, one of 14 days and the other, more simplified, of only 48 h. The absence of statistical difference between the models studied in this research (Table 3) allows one to affirm that the 48 h model appears to be more suitable, as there is a significant gain in time, and a lower rate of error in the procedure of changing the demineralization and remineralization solutions.
The results of this study demonstrated that when the two cycling models were analyzed (Table 2), the samples of the control group (0.21 mm2) presented a larger mean area of demineralization than did the samples of the groups treated with the argon and Nd:YAG laser (0.1 and 0.13 mm2, respectively), proving that the in vitro application of Nd:YAG 7,29 –31 and argon 8,9 is efficient in preventing the increase in the area of demineralization lesions in enamel. When analyzed in separate models (Table 1), the samples subjected to the 48 h cycle continued to demonstrate that both the Nd:YAG laser and the argon laser increased the enamel resistance to acid, as they presented a mean area of demineralization of 0.14 mm2 (argon laser) and 0.1 mm2 (Nd:YAG laser), whereas the control group presented a mean of 0.25 mm2 (Fig. 2). For 14 days of cycling, there was no statistically significant difference between the control group (0.18 mm2) and the Nd:YAG laser group (0.17 mm2), whereas for the argon laser group (Fig. 3) the mean enamel demineralization was statistically lower (0.07 mm2). Observing these data, it is possible to speculate that the alterations in surface enamel caused by the neodymium laser might not protect it against acid attachment in the long term, and that the application of the argon laser on enamel would be more effective. Moreover, it is supposed that perhaps the difference between the results of the Nd:YAG and argon lasers has shown the inferiority of the Nd:YAG laser by the increase in temperature during resolidification of the enamel surface, which could produce a chemical alteration, inducing the formation of less acid-resistant composites, and therefore, more soluble to the acid challenges that were used in vitro.
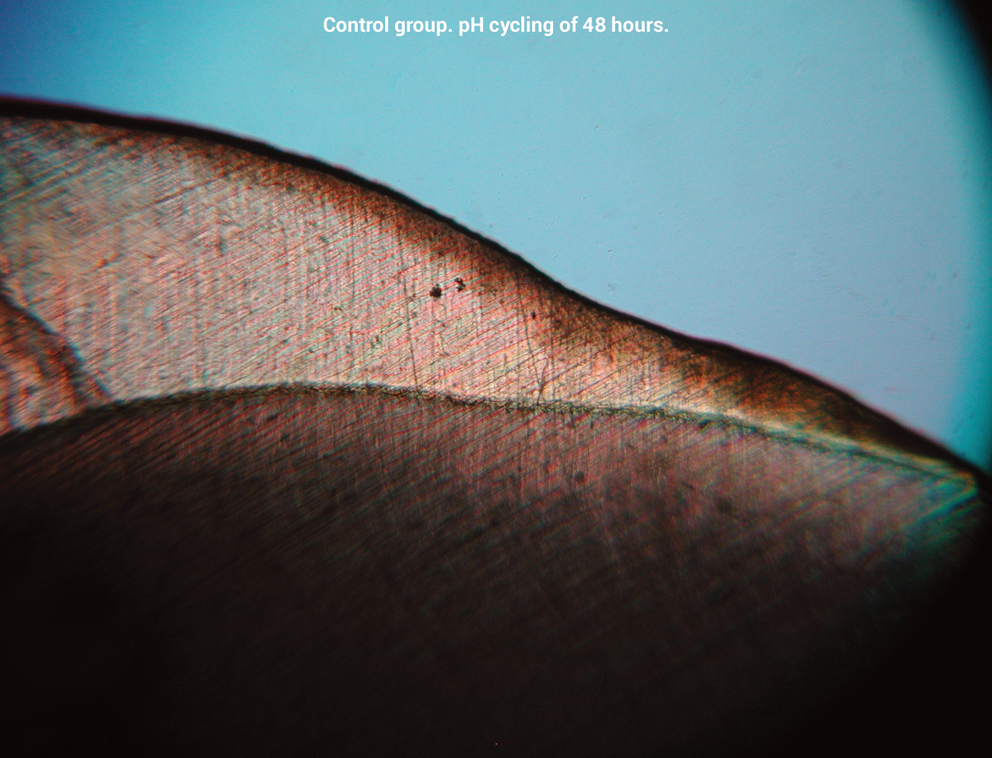
Enamel surface without treatment and submitted to pH cycling of 48 h (5× magnification).
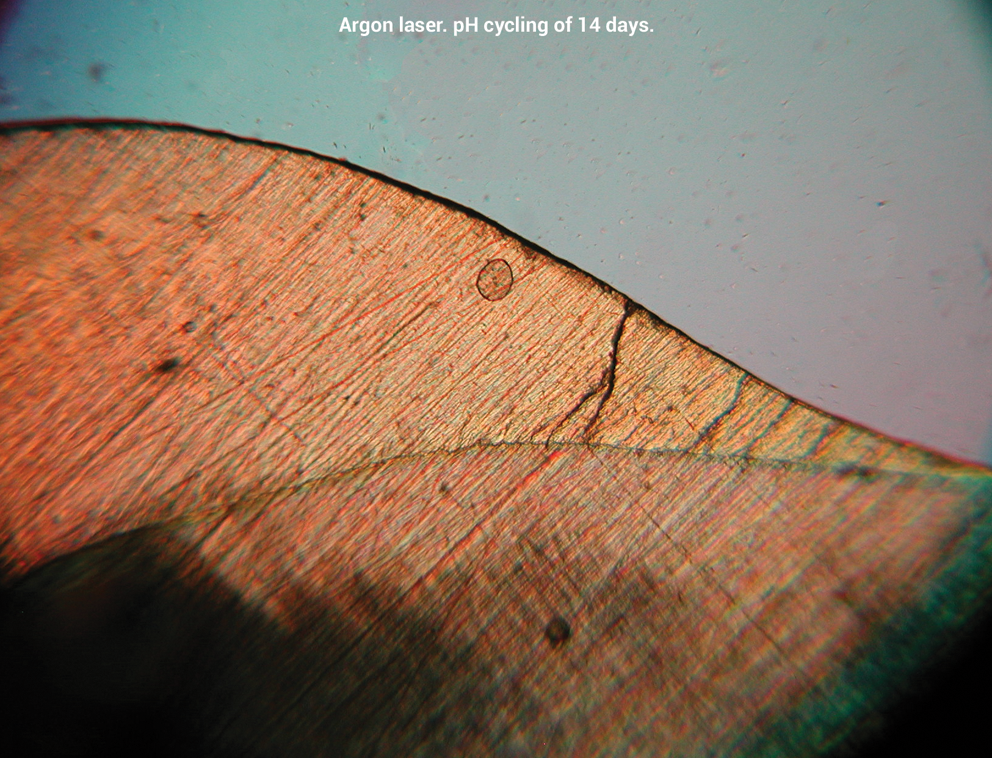
Enamel surface with argon laser treatment and subjected to pH cycling of 14 days (5× magnification).
On the other hand, there was no statistically significant difference when the cycles were compared with each other (Table 3). The samples submitted to cycling for 48 h presented a 0.16 mm2 mean demineralization area, whereas the samples of the 14 days of cycling presented 0.14 mm2. Therefore, 48 h of cycling can be recommended as being the most indicated, as it requires less time to be concluded.
It would be interesting to conduct future in vivo studies, or epidemiologic studies, using laser technologies to prevent caries, in order to have an approach with a wider scope for the benefit of the population.
Conclusions
The argon laser was more effective for caries preventive treatment than the Nd:YAG laser, showing the smallest demineralization area in enamel.
Footnotes
Acknowledgments
Part of this work was supported by coordenação de Aperfeiçoamento de Pessoal de Nivel Superior (CAPES).
Author Disclosure Statement
No competing financial interests exist.