
Abstract
Introduction
Topical photodynamic therapy (PDT) with 5-aminolevulinic acid (ALA) was first described by Kennedy et al. in 1990, and is a potentially advantageous treatment modality similar to PDT with methyl-ester-5-aminolevulinic acid (MAL, Metvix, Galderma). 5 MAL was approved for the treatment of superficial basal cell carcinoma (sBCC) and actinic keratosis (AK) in 2004, and for the treatment of Bowen's disease (BD) in 2006 in most European countries. Since then, high complete response (CR) rates combined with excellent cosmetic outcomes have been obtained in many studies. 6 PDT is an accepted treatment for non-melanoma skin cancer, especially superficial growing lesions, and is included in several clinical guidelines. 7 –9 Nevertheless, topical PDT is only effective against tumors up to a depth of 2 mm, 9 and therefore the application of PDT is limited to superficially spreading tumors only. Some clinicians advocate using ALA-PDT for thicker tumors, thereby sacrificing therapeutic effectiveness for aesthetic outcome and patient acceptance. 10
The need for proper noninvasive case selection prior to PDT for deeper tumors is obvious. Without a proper depth measurement, the treatment is not fully effective and results are not optimal. Skin ultrasound can be potentially used for measuring tumor depth noninvasively, and proper measurements allow for the selection of appropriate treatment strategies. We have previously investigated the use of noninvasive methods for the precise measurement of tumor depth and found that depth measurement by ultrasound and diameter control by fluorescence diagnostics (FD) were more precise than those conducted by conventional methods (dermatoscopy, palpation). 11 We have also explored surgical laser ablation immediately prior to PDT to decrease the size of the original tumor mass and obtained improved therapeutic efficacy. 12 Properly selected laser ablation also has the benefits of providing deep curettage without wound bleeding, which would lower the MAL concentration in the lesion. The use of a CO2 laser provides thermocoagulation of the surrounding tissue, and minimizes or eliminates bleeding. The Er:YAG laser, on the other hand, gently ablates a precise layer. 13
In this study, we analyzed a subgroup of patients with BCC of different depths, treated in our clinical center, and found high response rates to ultrasound-guided ablative laser-assisted photodynamic therapy (US-aL-PDT). Therefore, we recommend this procedure as a treatment modality for BCCs of varying thickness.
Materials and Methods
All patients were informed of the experimental nature of the treatment and signed informed consent approved by the ethical committee of Charles University (IGA MZ 8390-3). All patients were diagnosed in the Department of Dermatology of Charles University with at least one histologically confirmed primary BCC. All diagnoses were made by punch biopsy and histopathological examination that included a thickness measurement. Exclusion criteria were histologically-verified morpheaform BCC, pigmented BCC, and/or the inability of the patient to attend regular follow-up and monitoring of progress at 1, 3, and 6 months after initial treatment. If patients failed to attend a checkup or second PDT within 30 days of the appointment date for any reason, or if any medical operation intervened in the treatment schedule, the patient was removed from the study. As a result, 75 lesions of the original 100 treated (25 were excluded for reasons mentioned). Lesions from a total of 67 patients were evaluated. The study population consisted of patients who received both primary and secondary dermatological care. All patients were adult Caucasians with a mean age of 68.7 years (range 28–85 years), and the study population consisted of 38 males and 29 females. The average diameter of the lesions was 18.96 mm, and the overall range of the lesion size was 3–130 mm. Lesions were located at different sites of the body (Table 1), but the most commonly treated lesion was located on the face. Seventy-five lesions from 67 patients were histologically or dermatoscopically verified. Each lesion was measured for depth by an experienced independent dermatologist, and then assigned to one of three groups based on tumor depth determined by ultrasound (20 MHz, Atys Médical, France).
Group A included 44 lesions with a depth <2 mm and no pre-ablation was used. The skin surface was cleaned with a water solution of chlorhexidine digluconate 0.12% and dried. MAL was applied to the surface of the lesion and 10 mm beyond the visible edge, to the surrounding tissue, which was considered a “safe margin” according to the treatment protocol recommended by the manufacturer. 14 The cream was then covered with an occlusive bandage and a second cotton bandage to protect it from light penetration. The treatment was then left in place for exactly 3 h according to the manufacturer's protocol, and during that time, the patients were kept calm and not allowed to leave the facility, in order to minimize the influence of environmental conditions during the treatment. After 3 h, the bandage was removed and the tumor was cleaned with a physiological solution to remove unabsorbed residual cream. The lesion was then examined in a dark room under a Wood's lamp (366 nm wavelength), as protoporphyrin IX (PpIX) appears red under ultraviolet (UV) light and can be visualized by FD. The surface was illuminated, and the maximal diameter of fluorescence was measured (data not shown). Illumination with an Aktilite CL-128 (630 nm, Photocure, Denmark) with a dosage of 37 J/cm2 was then performed and a fan was used to improve cooling and minimize patient discomfort. Patients were advised to use cooling at home in cases of pain, burning sensation, and/or swelling. After illumination, the lesion was covered with a sterile dressing that was secured for at least 72 h or as necessary. Patients were informed of the need to protect the lesion from light after illumination in order to avoid cutaneous phototoxicity. After 1–3 weeks, the second PDT was performed using the same procedure and conditions. 13
Group B consisted of 19 lesions with a tumor depth of 2–3 mm determined by ultrasound, and received additional tumor curettage prior to PDT. The curettage was performed on the day of the first PDT session. In this group, an Er:YAG laser with a wavelength of 2940 nm (Skinlight, Fotona, Slovenia) was used with an energy level of 450–650 mJ and a frequency of 7 Hz. When necessary, articaine (Supracain, Zentiva, Czech Republic) was administered by subcutaneous injection, and the tumor was ablated until there was subjective certainty that the lesion had been completely removed. The risk of bleeding was minimized by the alternation of the laser between the focal point and the area outside the focal point. The PDT procedure, bandaging, and patient instructions followed those described for Group A.
Group C consisted of 12 lesions with a tumor depth that exceeded 3 mm, which were treated with a 980-nm diode laser (Ceram, UK) with an energy level of 4–8 W. Articaine injection was used as an anesthetic, and the tumor was completely removed. The PDT procedure, bandaging, and follow-up were identical as those described for Group A.
Patients in all groups were required to attend follow-up visits at 1, 3, and 6 months after treatment or when needed. After 6 months, a clinical evaluation was performed. In cases in which there was doubt, histological testing was performed to clarify the result.
Results
Patients were initially evaluated by an experienced dermatologist who assessed the depth of the tumor by means of clinical investigation and digital dermatoscope only. Thereafter, the same patients were assessed with a 20 MHz skin ultrasound, and 75 identified lesions were divided into three groups based on tumor depth (Table 2). An experienced dermatologist incorrectly assessed the depth of 10 lesions (13.3%). Of these, the dermatologist determined that seven lesions were superficial, but ultrasound determined that the depth was 2–3 mm. The three remaining lesions were determined to have a depth >3 mm (Table 3). In these cases, treatment with PDT only would have been inadequate and most likely would have resulted in early recurrence. The diameter of the lesion fluorescence was measured by FD and compared to the visible margins (data not shown). All of the patients were treated according to the depth of lesion measured by the skin ultrasound. In Group A, none of the lesions showed any scarring, changes in pigmentation, or redness at the 6-month evaluation. In Group B, the 6-month evaluation found only moderate changes of pigmentation and/or redness, but no scarring. In Group C, all patients showed flat scarring (smaller than the original tumor) with no traction, and only moderate changes in pigmentation 6 months after treatment. The total recurrence rate in the study was 12%, and the maximum recurrence rate of the study occurred in Group A (18.8%; Table 4). In Group B, the recurrence rate was 5.3%, and no recurrences were observed in Group C.

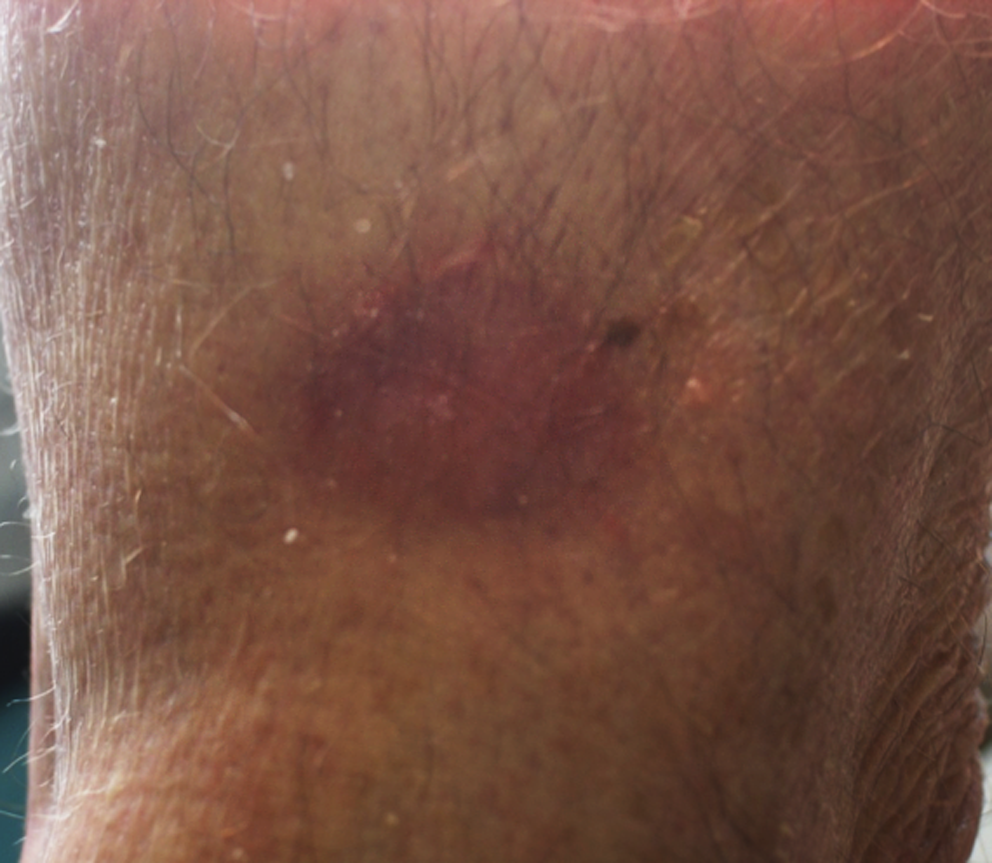
Nodular BCC, lower extremity, before treatment.
Same location as in Fig. 1: after single treatment.
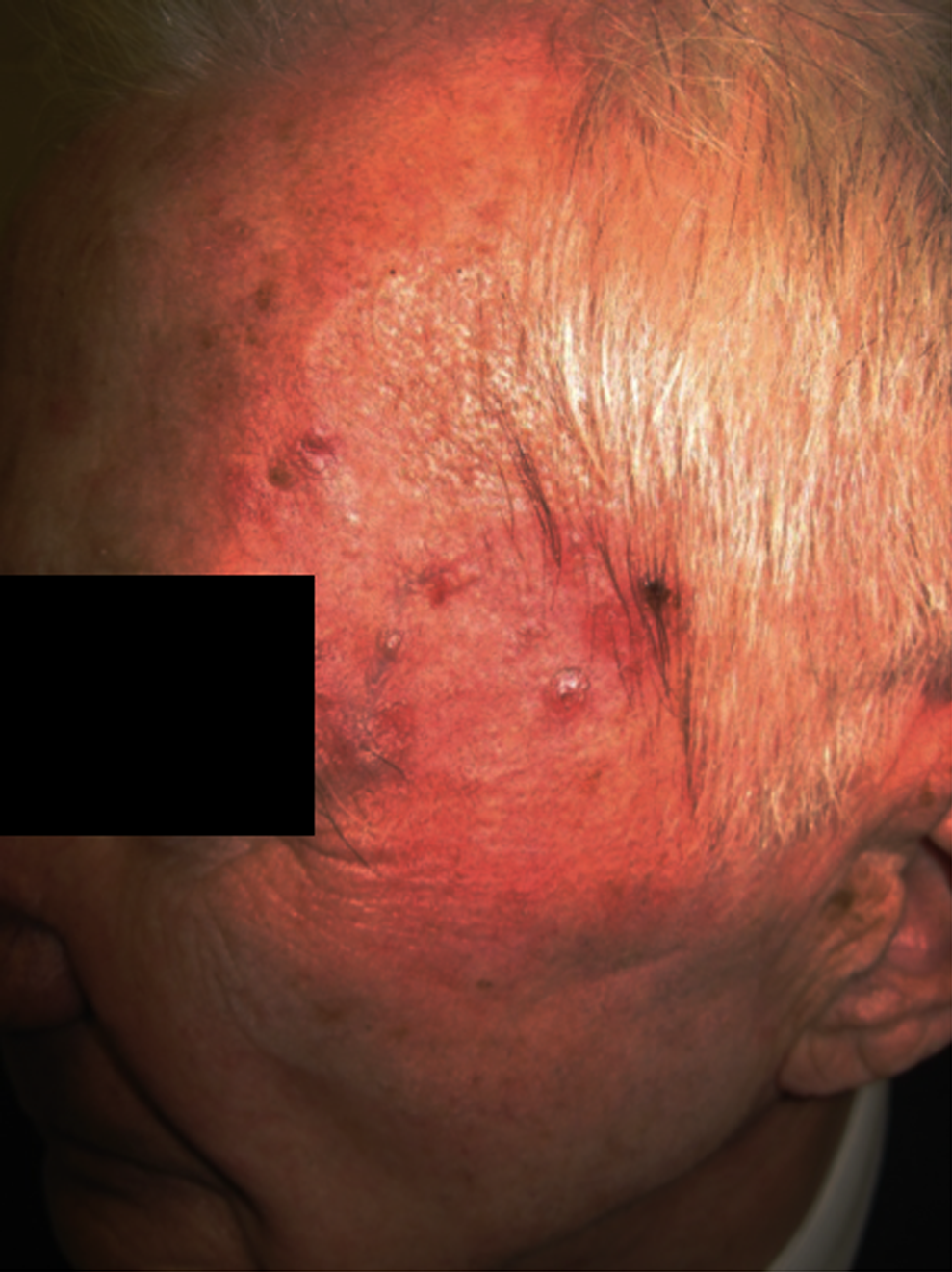
Patient with multiple BCCs: clinical picture.
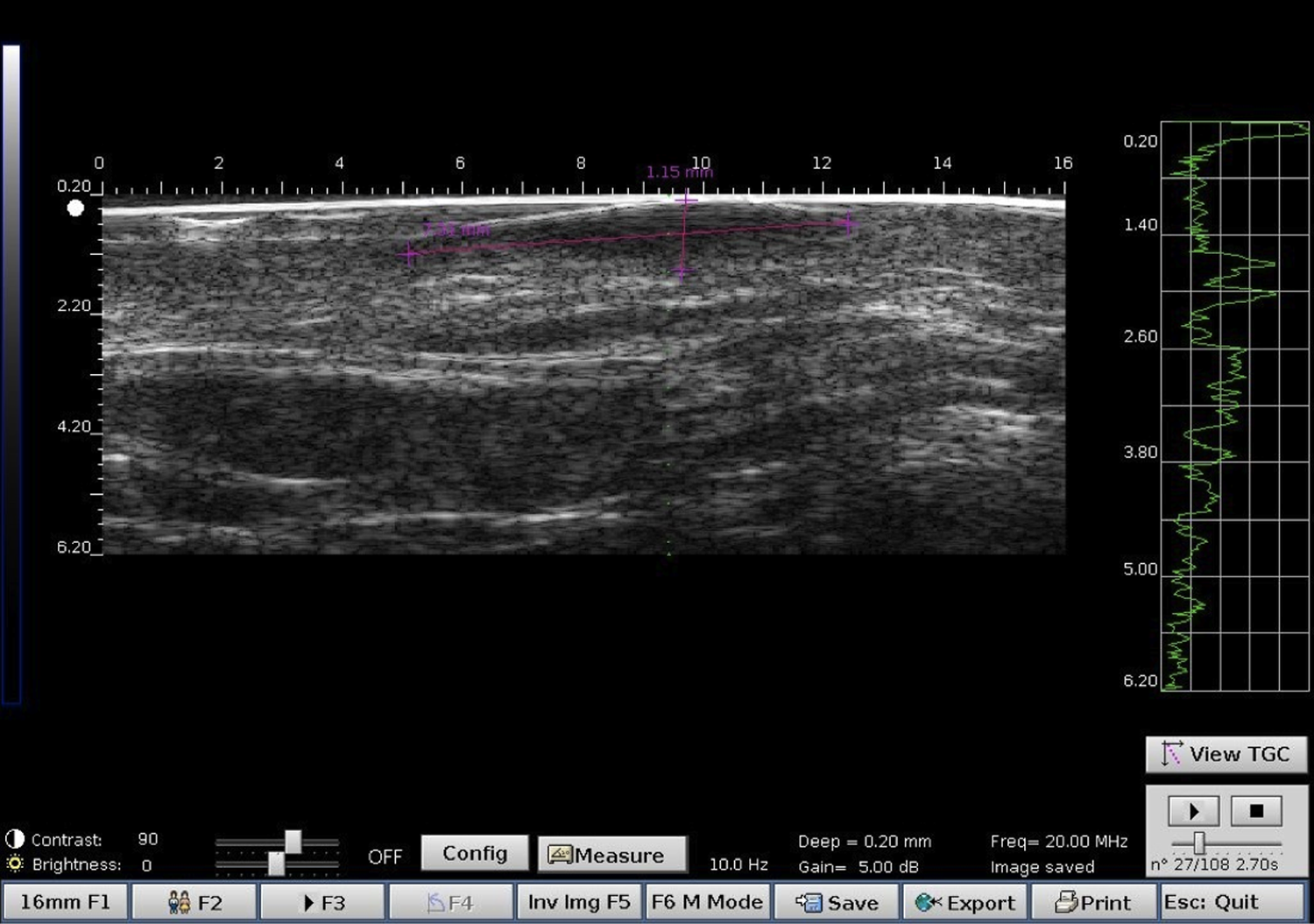
Same patient as in Fig. 3: ultrasound measurement of BCC.
Discussion
Based on the observations of this study, we found that the measurement of tumor thickness with ultrasound prior to treatment improved the effectiveness of MAL-PDT for lesions thicker than 2 mm. In our previous study, we found that laser pre-ablation effectively treated BCC lesions, and may be even be more effective than the current standard of care of curettage or microdermabrasion. 10,11,14 We also found that high frequency ultrasound can be used as a precise guide for ALA-PDT in the treatment of noninvasive lesions. 12 Therefore, we hypothesize that the combination of these two modalities into one protocol will improve clinical outcomes even further. As treatment guidelines are become increasingly important in the field of dermatology, the results of this study may have important implications for future guidelines in PDT.
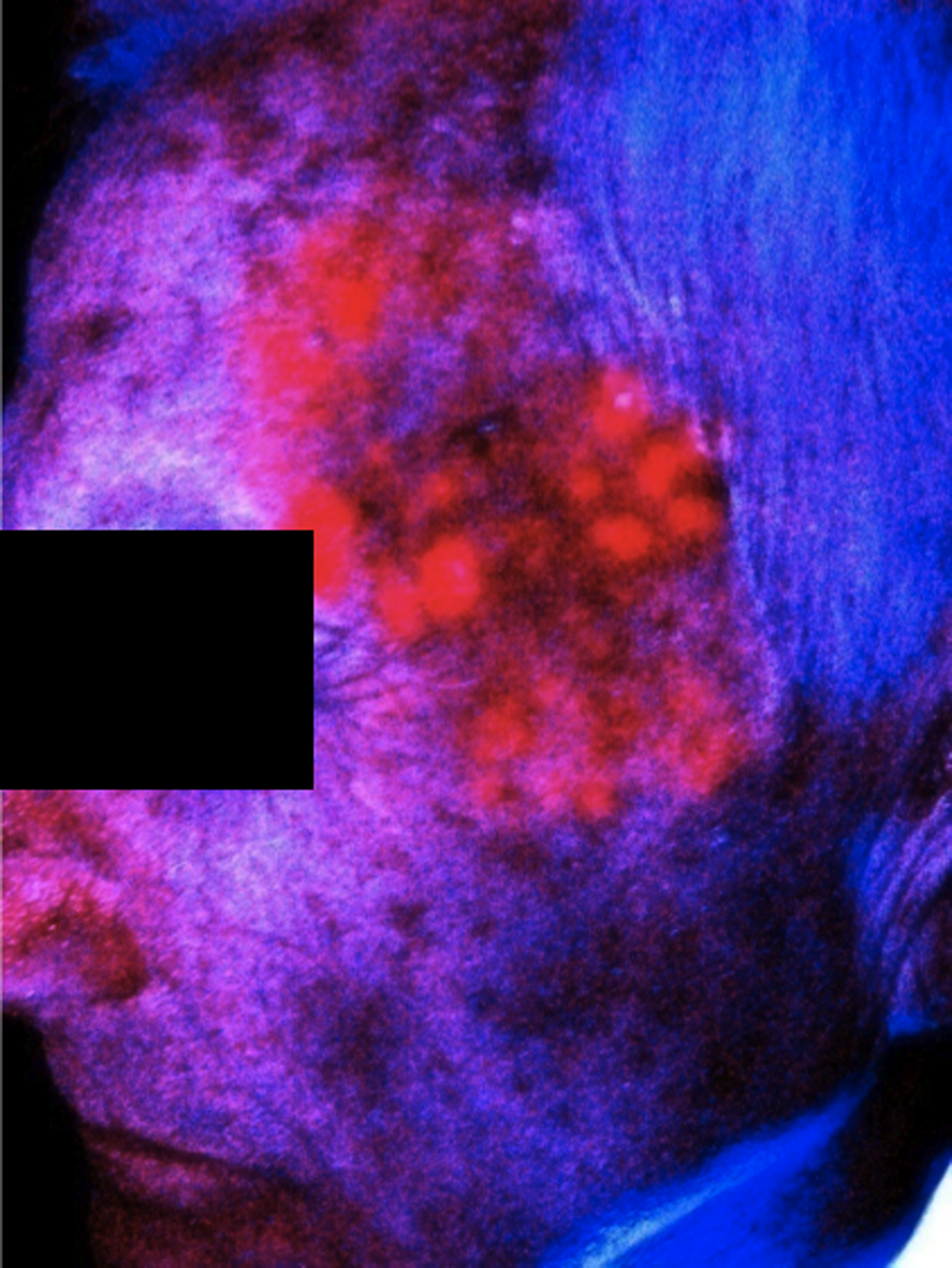
Same patient as in Fig. 3: real size of pathological process (fluorescence).
We found no correlation between the type of laser used and recurrence rate, but a correlation was identified between the fluorescence borders and clinical outcome. Although a 12% recurrence rate is considered high, there are several variables in our study that may account for these observations. First, our study included difficult-to-treat BCCs, and some patients experienced >5 recurrences after surgery (Moh's surgery was not performed). Second, the patients in this study had a mix of different types of BCCs, including superficial, nodular, and invasive. The clinical course of these BCC types varies, where superficial BCC is easy to treat, nodular BCC is possible to treat with a high success rate, and invasive BCC is impossible to treat with ALA-PDT. Third, we performed PDT immediately after laser ablation, and a longer interval for the cleaning of necrotic tissue may be more appropriate. At the time of this study we did not have an appropriate method for measuring the fluorescence of PpIX properly, and we are currently addressing this issue in an ongoing study.
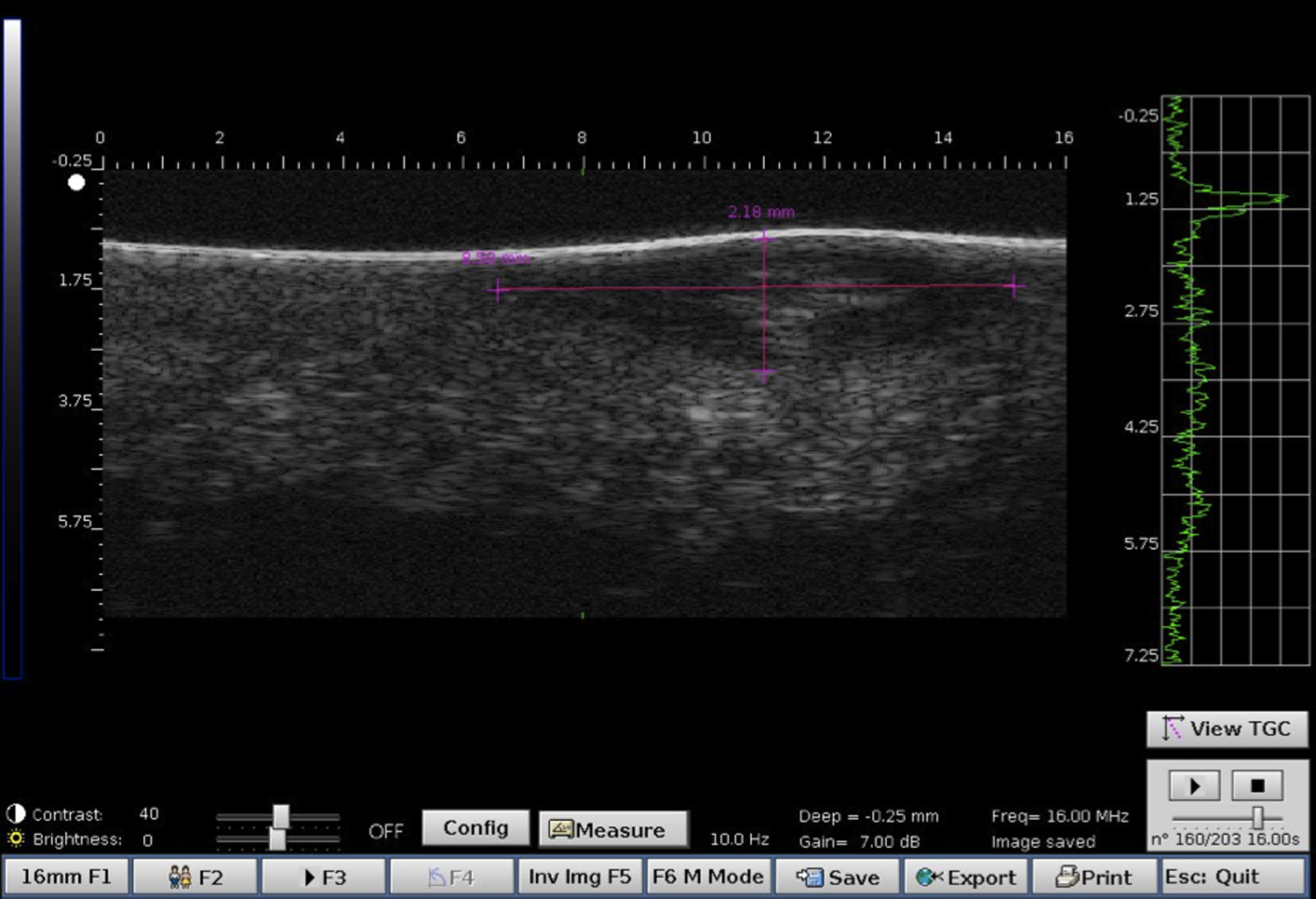
Ulrasound picture of BCC wrongly classified as superficial.
The recurrence rate was the highest in the group with lesions with superficial depth, and we did not find a statistically significant difference between recurrence rate and the size or site of the lesion. In this group, no laser curettage was performed, and therefore good penetration of MAL was critical for effectiveness. It may be possible to improve penetration through the use of fractional lasers 15 or microneedles, but additional studies are necessary to explore these options.
Our data showed that pure laser ablation, which is a simple and cheap modality for the majority of lesions, was highly effective for treating BCC. By using proper ultrasound-guided lesion measurement and full histopathologcal analysis, this procedure may provide acceptable outcomes for use in daily practice. One question that remains, however, is which laser is best for pre-treatment. The Er:YAG laser causes minimal thermal damage, but quick bleeding stops the treatment superficially. More aggressive lasers (800, 980, or 1470 nm) are effective at multiple depths, but it is unclear if it is necessary to wait for partial wound healing, and if so. for how long.
In this study, punch biopsies were performed after 6 months for a final evaluation; however, it is unknown whether 6 months or a partial punch biopsy is sufficient for this analysis. It is likely that a punch biopsy is not sufficient, but because of ethical concerns, a full excision was not possible. Therefore, a large multicenter study that includes precisely defined histopathological (invasive vs. nodular vs. superficial BCC) groups is currently underway.
Conclusions
In this study, we found that with proper case selection by ultrasound and subsequent laser ablation prior to MAL-PDT, the depth of a BCC tumor is not a limiting factor for PDT effectiveness. Ultrasound examination helps the clinician choose a proper treatment modality and is more precise than is common dermatoscopic evaluation. In addition, pre-treatment with an ablative laser may allow for the successful treatment of BCCs that exceed the current depth limit of 2 mm. We found that the aesthetic outcome of these patients was very good, and, therefore, that ultrasound-guided ablative laser-assisted PDT of BCC can be a method of choice, at least for aesthetically challenging cases.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.