
Abstract
The aim of this clinical report is to demonstrate the efficiency of Er:YAG laser in reducing symptoms and lymphoplasmocytic infiltrate in case of oral lichen planus (OLP). In addition to medical therapy and conventional surgery, laser has been proposed for the treatment of this disease, but currently, use of Er:YAG laser (2940 nm) has not been reported. Two clinical cases of female patients who came to our clinic with lesions in the internal portion of the cheek and in the hard palate mucosa close to the upper right molars, surgically treated by Er:YAG laser, are described. The parameters used were as follows: energy, 80–120 mJ; frequency, 6–15 Hz; non-contact hand piece; spot size diameter, 0.9 mm; pulse duration, 100 μsec (VSP) to 300 μsec (SP) ; fluences, 12.6–18.9 J/cm2; and air/water spray (ratio: 6/5). In the two patients, the peeling of the lesions was completed with much less discomfort (<25% in visual analogue scale). A very small recurrence was observed in one case (cheeks) after 15 months, and the same protocol was applied successfully. The use of this wavelength offers several advantages including, a good and fast healing process, a very low level of discomfort during and after intervention, and a rapid disappearance of symptoms. Even if this methodology seems to be an interesting new surgical approach in the management of non-erosive OLP, this clinical report has to be considered as a preliminary one because of the limited number of cases. As a consequence, further studies and long-term follow-up will be necessary.
Introduction
From the clinical point of view, OLP generally may be classified into two main forms with specific and identifiable aspects, reticular and erosive, 2 even if four other forms are described: papular, “plate-like”, bullous, and atrophic. 5 The reticular form occurs more frequently and is characterized by white lacy streaks known as Wickham's striae, which generally are surrounded by discrete erythematous borders. OLP is often asymptomatic, but in some cases there are areas of erosion or ulceration, and the patient may have variable amounts of discomfort, particularly when eating spicy or acidic types of foods. 6
Although OPL was initially described in 1869, little is known about the mechanisms by which the disease develops even if it is believed to be an autoimmune disorder mediated by T lymphocytes. Many authors suggested that a combination of specific and nonspecific mechanisms may be involved in the etiopathogenesis of this condition: this theory may explain the T lymphocyte accumulation in the lamina propria underlying the epithelium, as well as the rupture of the basement membrane, characteristic of OLP. 7 Other authors think that hepatitis C could be one of the factors able to set this process in motion 8 even if a direct association between lichen planus and hepatitis C cannot always be demonstrated. 9,10
Psychological factors have recently been strongly associated with lichen planus, in particular, high stress and anxiety levels. Although this association has been known for decades, difficulties in objectively measuring these variables has meant that only recently has the importance of anxiety and stress been widely recognized. 11,12
Regarding the risk of OLP to malignant transformation, opinions are very controversial. Even if the World Health Organization (WHO) classified this condition as a premalignant condition, several authors are convinced of the malignant potential of this disease, and others believe that there is enough data to prove this association. 13 –15 For this reason, even if the typical clinical features of OLP are generally sufficient to make a clinical diagnosis, biopsy is always mandatory to confirm it and mainly to exclude epithelial atypia and signs of malignancy. 2 However, other conditions may present similar histopathological findings to those of OLP: lichenoid reactions, lupus erythematosus, leukoplasia, erythroleukoplasia, and proliferative verrucous leukoplakia. For this reason, some authors have suggested using routine direct immunofluorescence in the diagnosis of OLP, particularly when other autoimmune diseases are included in the differential diagnosis. 16
Although OLP can spontaneously regress, many lesions eventually require treatment. The most commonly used agents for the treatment of OLP are topical corticosteroids. 2 Intralesional and systemic corticosteroids also are used. Topical and systemic medications include immunosuppressants such as cyclosporine and tacrolimus and topical or systemic retinoids. 17 The treatment of refractory disease has also been attempted with other agents, including thalidomide, 18 and even nonpharmacologic agents such as psoralen-UVA. 19
Considering the possibility of transformation of OLP, many authors have proposed the surgical excision of the premalignant lesions using conventional techniques 20 and with a free gingival graft. 21 In an alternative to the scalpel surgery, other authors have proposed cryosurgery; 22 and the oral mucosa, because of its characteristics of humidity and smoothness, is an ideal site for this technique. The vaporization of the OLP lesions by laser in patients whose condition causes spontaneous pain during eating and is unresponsive to topical corticosteroid, can lead to a long-term remission of symptoms and may even be the treatment of first choice. 23
In this clinical report, we propose the use of Er:YAG laser (2940 nm wavelength), which is normally used in oral surgery and in dermatology, 24,25 but which has not yet been described in the treatment of OLP lesions. The efficacy of ablation is given by its great affinity to the water, whereas the scanty thermal elevation and the consequent absence of tissue carbonization are responsible for the good healing process. The aim of this clinical report is to demonstrate the efficiency of an Er:YAG laser in reducing symptoms and lymphoplasmocytic infiltrate in cases of OLP.
Materials and Methods
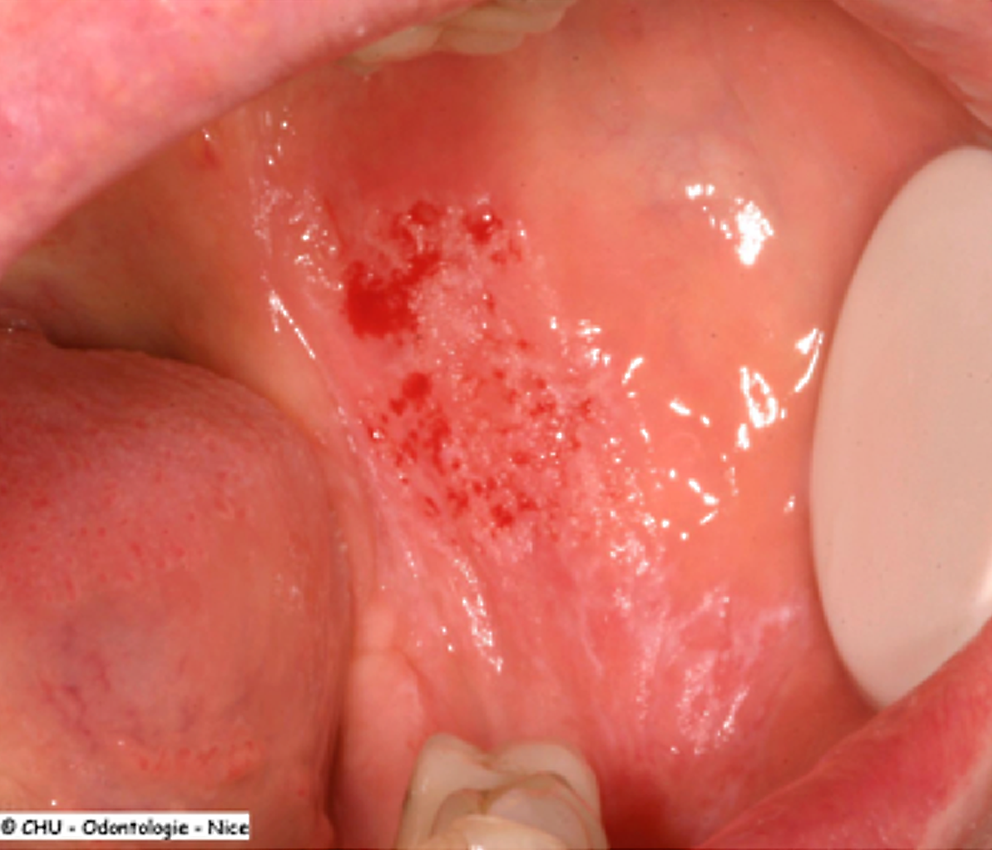
Two female patients, 52 and 56 years old, came to our clinic with lesions in the internal portion of the cheek and in the hard palate mucosa close to the upper right molars (Fig. 1). A clinical diagnosis of OLP based on clinical observation; anamnesis; and research of etiologic factors such as systemic medications, dental materials, chronic liver diseases, stress, and genetics; had been previously addressed in both of the cases by the family physician, and corticosteroids had been prescribed topically (prednisolone 5 mg dissolved in 15 mL of water and used as a mouth rinse up to 4 times daily) without any symptom remission.

Macroscopic aspect of the lesion, extended in the internal face of the check and the retromolar area, before intervention.
Because the patients complained a lot of discomfort while eating, particularly with acidic foods, and presented roughness of the lining of the mouth and oral ulceration persistence, it was decided to perform a biopsy by scalpel, which confirmed the clinical diagnosis (Fig. 2).
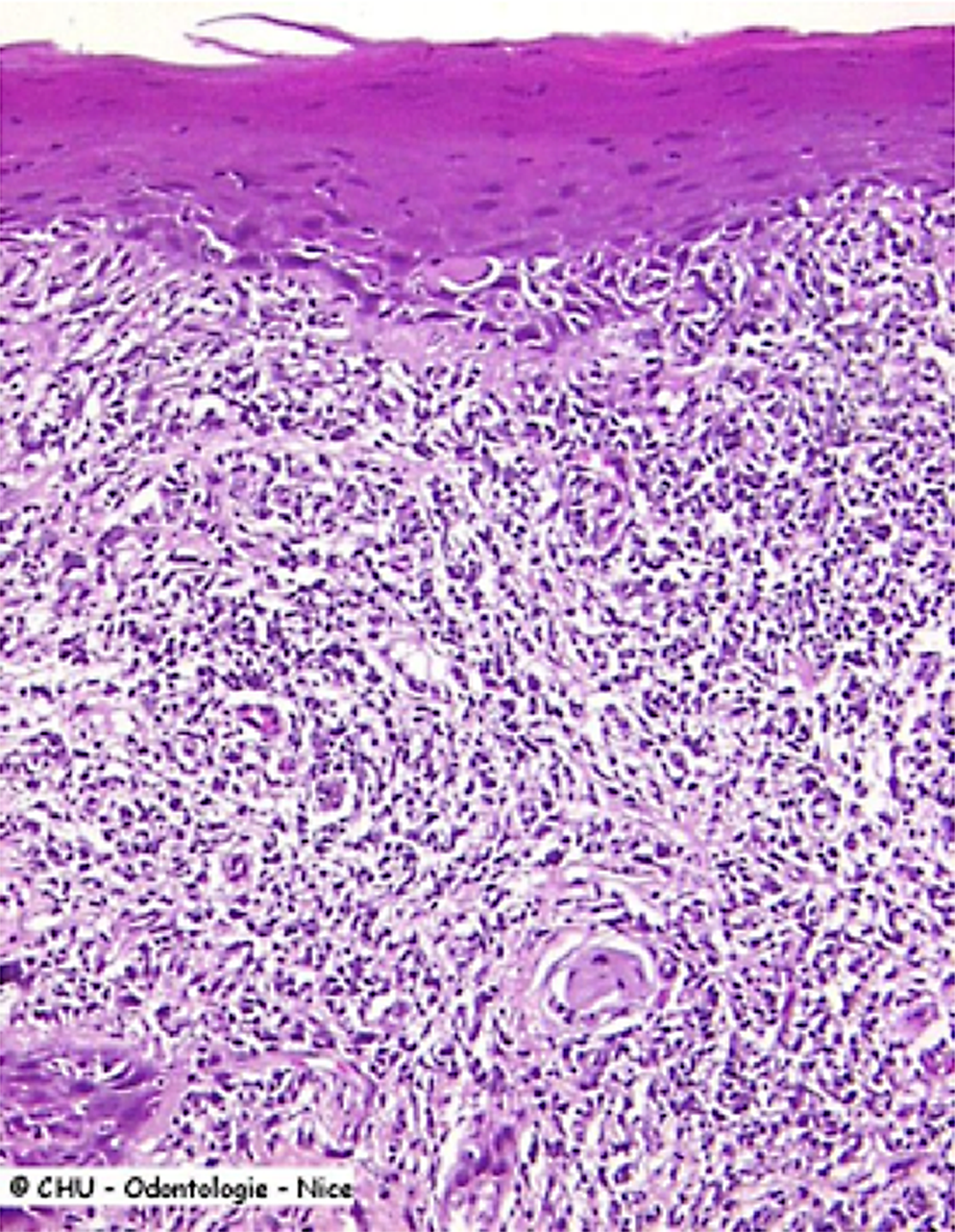
Histological observation of the lesion after incisional biopsy (original magnification x40). Presence of a band-like infiltration of lymphocytes in the connective tissue. Presence of colliquative degeneration in the keratinocyte basal layer.
After obtaining the written informed consent of the patients, superficial vaporization (peeling technique) of the oral lesions was performed using Er:YAG laser (Fidelis Plus III, Fotona, Slovenia).
A topical anaesthetic (EMLA, Astratech) was applied in the surgical area 10 min before surgery, and the following parameters were used: Energy: 80–120 mJ Frequency: 6–15 Hz Non-contact hand piece, spot size diameter: 0.9 mm Pulse duration: 100 (VSP) to 300 μsec (SP) Fluences ranging from 12.6 to 18.9 J/cm2
Air/water spray (ratio: 6/5)
The durations of the interventions were 70 and 120 sec. and the technique used consisted of the movement of the hand piece on the mucosa with a slow gliding motion, maintaining a distance of 7 mm from the target tissue.
Because of the impossibility of maintaining this working distance precisely and also of measuring it, the 0.9 mm dimension of the spot of must be considered as approximate.
A visual analogue scale (VAS) was used during the intervention and in the period after to grade the subjective discomfort severity. No drugs (antibiotics and/or anti-inflammatories) were prescribed, and no sutures were used.
Results
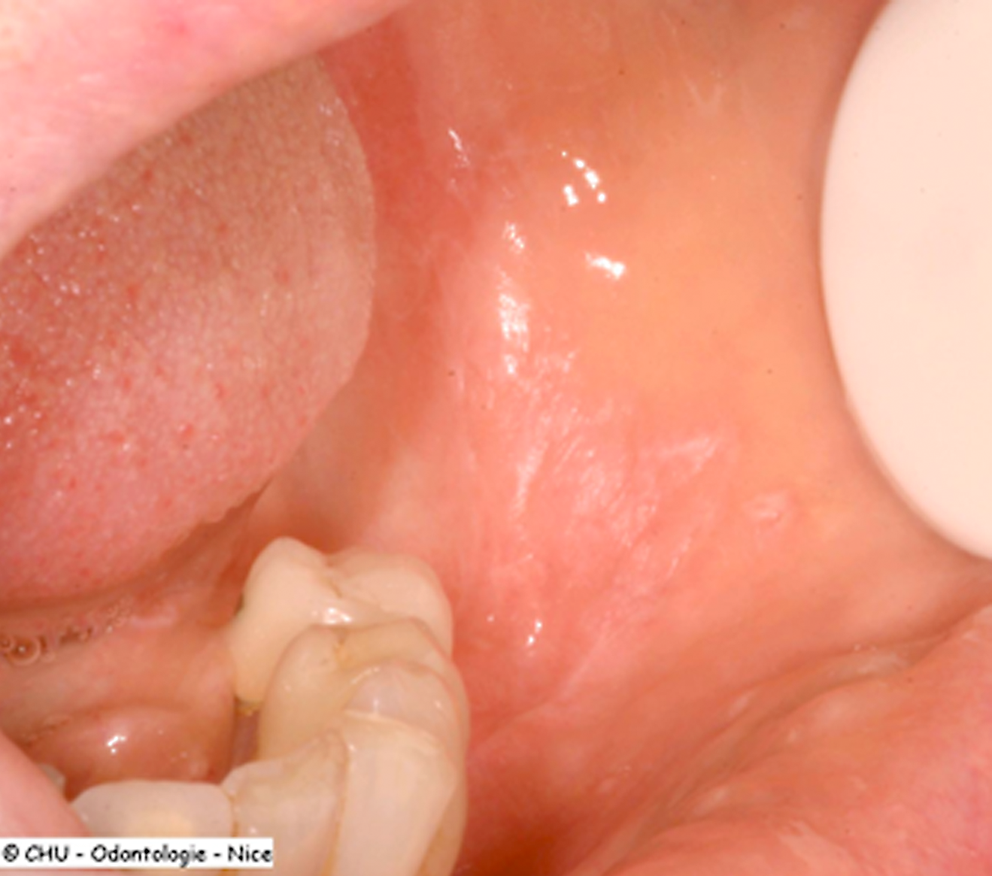
In the two patients, the peeling of the lesions was complete with much less discomfort (<25% in the VAS). Bleeding was very scanty, and carbonization was never observed (Fig. 3). The healing process was fast and without complications (Fig. 4) and was completed in 10 days (Fig. 5). The patients were checked at 3, 7, 10, and 15 days, after 1 and 3 months, and also during this period, the discomfort reported was minor (<25%) in the VAS.
Aspect of the lesion just after intervention, with scanty bleeding and absence of carbonization.
The lesion observed 1 week after intervention, with healing process not fully completed.

The lesion 10 days after intervention. The healing process is completed and the aspect of the mucosa appears normal.
The burning sensation as well as the pain accompanying the OLP disappeared. A very small recurrence was observed in one case (cheeks) after 15 months, and the same protocol was applied again successfully.
Discussion
Several laser wavelengths have been used in the treatment of OLP lesions. In 1984, Frame described the first three cases treated by vaporization with a CO2 laser 26 with the process of re-epithelialization completed in 6 weeks; other authors suggested the use of this technique, considering the high level of precision as compared with the use of the scalpel, and giving an immediate relief of symptoms. 26,27 The use of different wavelengths, such as Nd:YAG laser (1064 nm), excimer laser (308 nm), and helium–neon laser, and more recently, the “photodynamic therapy” (PDT) treatment by association of light-emitting diodes and 5-aminolevulinic acid subsequently was reported. 28 –32 The main criticism of laser surgery for oral lesions in general and for potentially premalignant diseases in particular is that tissue-vaporized lesions cannot be completely examined histologically. 33
This is the first clinical report regarding the use of Er:YAG laser as a peeling methodology of non-erosive OLP, confirmed by incisional biopsy. Er:YAG laser is a solid active medium, which emits radiation in the infrared portion of the spectrum (2940 nm) and is highly absorbed in water and hydroxyapatite. 34
This laser was first used for cavity preparation because of its capacity—in synergy with an air-water spray—to ablate the dental enamel and the dentin without thermal damages for the pulp tissue. 35
For that reason, this laser produces a so-called “cold ablation,” and as a consequence, carbonization is never observed. This could explain the good healing process observed in oral surgery; 36,37 however, this wavelength is not absorbed in hemoglobin, and there is only a slight bleeding in the operative field.
Thermal elevation is the area in which this laser differs from the others normally used in dentistry, and this was the reason for the choice of this wavelength in treating these kinds of diseases. In fact, we observed that, whereas the intra- and postoperative bleeding was very scanty and without any risk or necessity to perform particular surgical or pharmacological acts, intra-operative pain was absent, even with use of only topical anesthetics, and the healing process, even without drugs, was fast and without any problems.
Conclusions
OLP is a chronic inflammatory oral mucosal disease in which the cell-mediated immunity plays a major role. In the past, its surgical management included cryosurgery and laser vaporization. Surgical excision with Er:YAG laser, using low fluences, associated with or following the removal of hypothetical causative agents, represents an improved OLP management, with several advantages that include a good and fast healing process, minor discomfort during and after intervention, and a rapid disappearance of symptoms. Moreover, it may also represent an effective opportunity to prevent malignant transformation of the lesions.
Even if this methodology seems to be an interesting new surgical approach in the management of non-erosive OLP, this clinical report has to be considered as a preliminary one because of the limited number of cases. As a consequence, further studies and long-term follow-up are necessary.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.