
Abstract
Introduction
Nipple trauma is characterized by rupture of the skin that covers the nipple, 4 with fissures, cracks, and abrasion being the most common injuries, which are usually accompanied by local pain. 5 They are one of the significant factors in early weaning and, if not treated, can eventually lead to mastitis. 6
There are many predisposing factors for nipple trauma. 7,8 However, the main cause is inadequate breastfeeding technique, such as a wrong positioning and latch-on of the infant. 9,10 The usual therapeutic approaches for nipple trauma include orientation on correct techniques of breastfeeding and nipple care, and application of sunlight, warm water compress, teabag compress, lanolin, and freshly extracted breast milk. 11 –14 These, however, may not be enough for the healing of nipple trauma, or their effectiveness has not been adequately assessed. 15
A promising alternative for the treatment of nipple trauma is low intensity phototherapy, which promotes photobiomodulation, a process in which an irradiated light, in the red to near infrared region of the spectrum (630–1000 nm), modulates numerous cellular functions. 16 LED phototherapy is a fairly recent category of phototherapy, and there is evidence that it accelerates wound healing and promotes analgesia. 17,18 The LED radiation is deemed to stimulate fibroblast proliferation; 19 to enhance synthesis of collagen, RNA, DNA, and adenosine triphosphate (ATP); 20,21 and to promote increases in the local vascularization 22 and changes in nerve conduction. 23
As there is no scientific evidence of an effective treatment for nipple trauma, 14 the study of new therapeutic approaches is of relevance to alleviating the problems associated with incorrect breastfeeding practices. In view of the aforementioned, the aim of this pilot study was to evaluate the effectiveness of an LED-based prototype apparatus for the phototherapeutic treatment of nipple trauma.
Materials and Methods
Study design and participants
The pilot study was designed as a randomized, placebo-controlled intervention trial. The study protocol was approved by the Research Ethics Committee of the Universidade Federal de Minas Gerais (protocol No. ETIC 205/07, August 30, 2007), Brazil.
Participants were consecutively recruited between August and October 2010 at the Hospital das Clínicas in Belo Horizonte, Brazil. Inclusion criteria were the following: (1) presence of nipple trauma (abrasion, crack, or fissure), (2) no clinical signs of infection, (3) being up to 5 months postpartum, and (4) being between 18 and 40 years of age.
Abrasions are excoriations of the skin in which a portion of the dermis is exposed. Cracks and fissures are lesions of the slit type, with either vertical or curved shape, that occur at the surface of the nipple or at the nipple–areola junction. The crack is a superficial skin lesion that at its deepest level extends at most to the epidermis. A fissure is a lesion that can reach the topmost portion of the dermis layer. The identification of the type of lesion was done by visual inspection by a qualified medical professional.
The exclusion criteria were: (1) presence of cancer, (2) photosensitivity or any adverse reactions to exposure to sunlight, (3) pregnancy, (4) use of other forms of treatment for nipple trauma, and (5) cognitive impairment.
Of the 30 participants with nipple trauma who were recruited, 14 were excluded because of: cognitive impairment (1); age <18 years (2); and lack of interest in the research (11). Of the 16 participants who met inclusion criteria and initiated intervention, 6 were excluded for concomitant use of another form of treatment, for interrupting breastfeeding, or for abandoning the study.
The study was conducted at the Hospital das Clínicas and at the Instituto Jenny Andrade Faria, both part of the Universidade Federal de Minas Gerais (UFMG) hospital complex. Oral and written descriptions of the study and explanations regarding the voluntary and confidential nature of the research were given to all participants. Also, they were made aware they were free to withdraw from the study at any time. An informed consent was obtained.
Randomization
Socio-demographic and clinical information was obtained from the participants and a clinical evaluation of the breasts and nipples was performed by a specialized medical practitioner. After clinical evaluation, the participants were randomized into two therapeutic groups by means of sealed envelopes. Identification tags corresponding to therapeutic groups A or B were placed in sealed unmarked envelopes and shuffled. The number of envelopes was the same for both groups. With each new participant who entered the study, an envelope was randomly selected and opened, with the participant being duly assigned to either group A or B.
Interventions
Standard treatment and active phototherapy were applied to both nipples of the women in group A (experimental), and standard treatment and placebo phototherapy were applied to both nipples of the women in group B (control) (Fig. 1). During the first days, most of the measurements were undertaken in the hospital setting. After discharge from the hospital, the participants were subjected to therapy at the Instituto Jenny Andrade Faria.
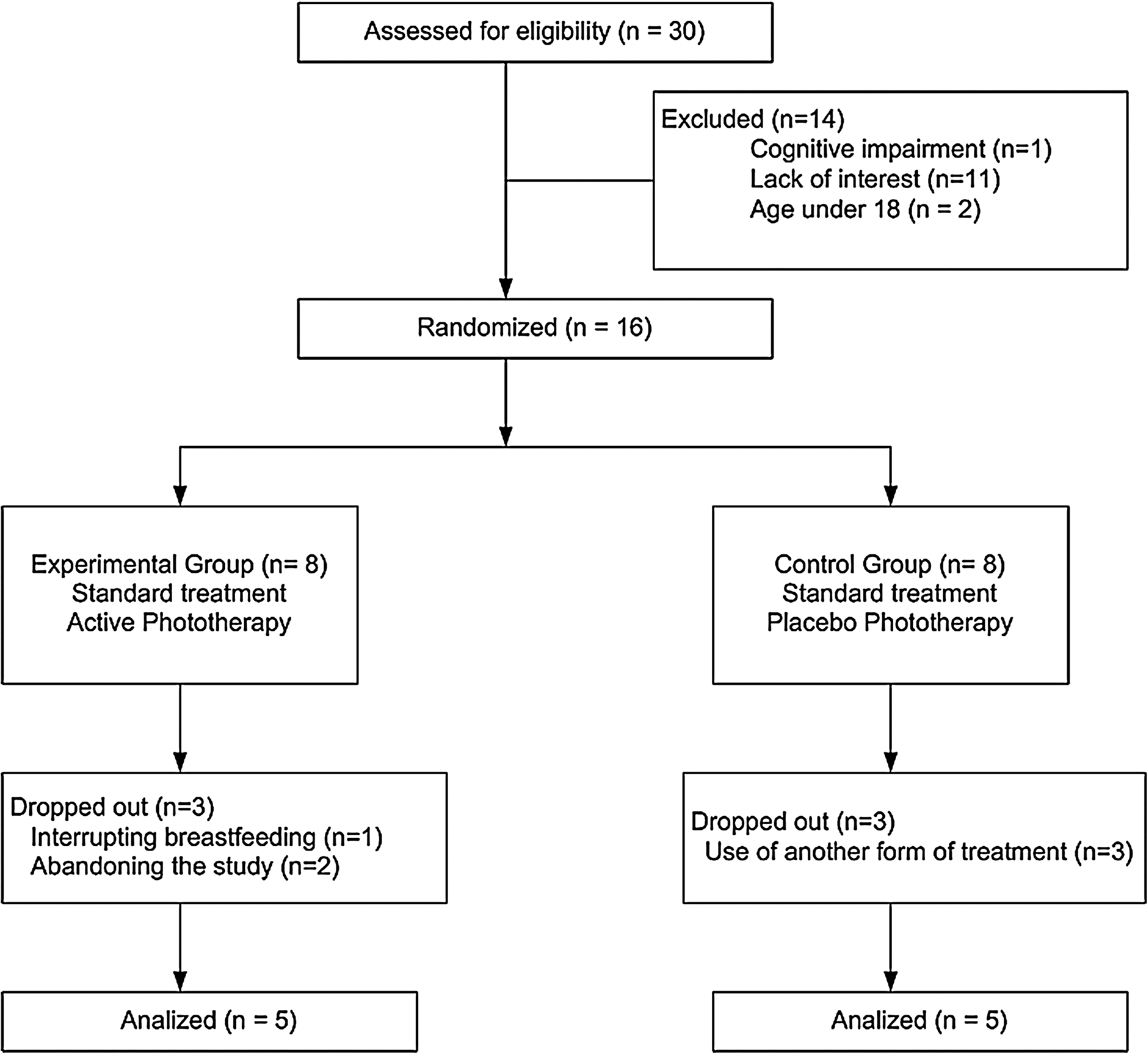
CONSORT flow diagram of the study.
Standard treatment
The standard treatment consisted of adequate techniques of breastfeeding and nipple care orientation, with regard to: positioning of infant and mother during breastfeeding; proper latch-on of the infant; correct technique for removal of the infant from the breast; number, duration, and intervals between feedings; stating that breast milk was the ideal food until the infant was 6 months of age; no interruption of breastfeeding; no use of creams or any other products on the nipples; and wearing of a suitable brassiere. 11,3
This information was orally given to participants by a therapist who was blinded to the group the participant belonged to, during the initial evaluation, and reinforced by an educational brochure given to each participant.
Phototherapy
The prototype apparatus for LED phototherapy was developed by the company Bios Serviços e Comércio Ltda in partnership with the Bioengineering Laboratory (Labbio) of UFMG. The LED phototherapy prototype apparatus is composed of two distinct components: an applicator and a control system. The applicator is composed of a base structure (component to the right in Fig. 2A) and a fuse (component to the left in Fig. 2A) that is connected to the base structure. The base structure is the part that contacts the breast, being designed to be compliant with the female breast shape. Five LEDs are embedded in the fuse and the fuse is screwed into the base in such a way that the LEDs do not touch the nipple or the areola. The applicator is attached to a brassiere (Fig. 2B) that holds it in place in a way that its fuse is aligned with the nipple and areola of the breast being irradiated. The control system is connected to the outer portion of the fuse, which in turn is connected to a computer through a USB port and is managed by specific software developed for this purpose. The software calculates the irradiation time as a function of the desired dose and allows for a user- friendly control of the apparatus based on the defined parameters.
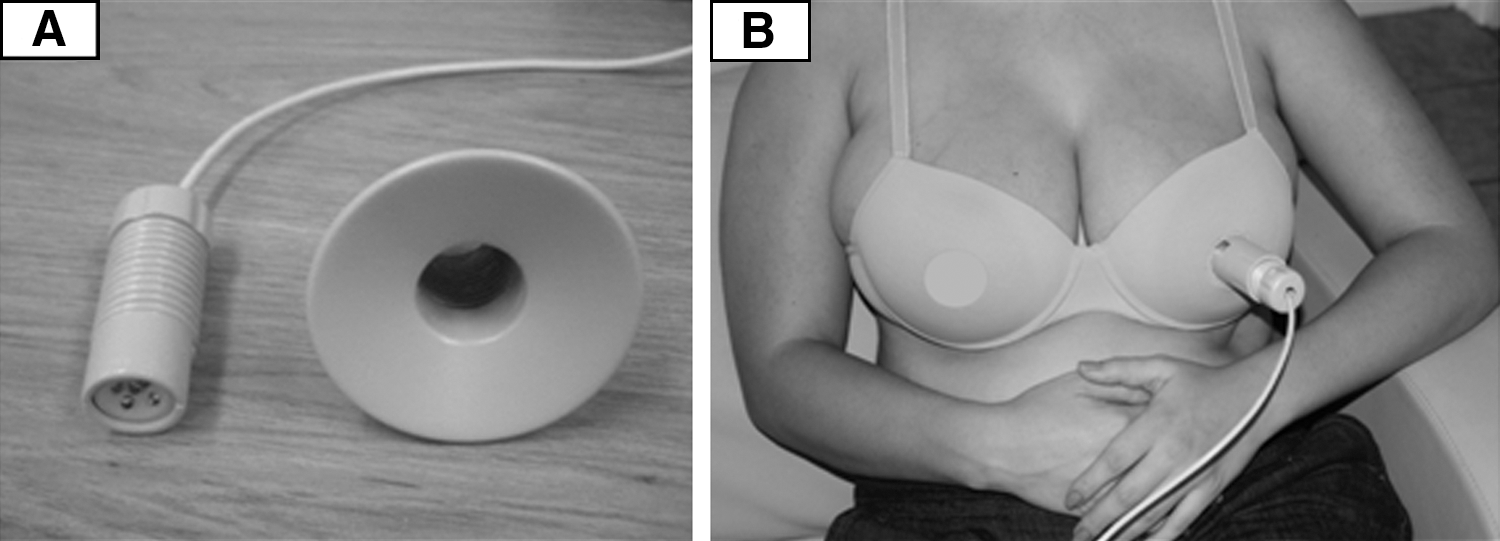
LED phototherapy prototype and placement of prototype during application.
For the double-blind study, two identical prototypes were assembled, both designed in compliance with the anatomy of the female breast (Fig. 2A), with one of them active and the other inactive. The active prototype, herein referred to as A, emitted radiation and was applied to participants in the experimental group. The placebo prototype, herein referred to as B, did not emit radiation and was applied to participants in the control group. The applicant therapist and the participants were blinded in regard to the prototype being used during the therapeutic sessions. They had no contact with the manufacturer of the prototypes during the study.
The values selected for the prototype operational parameters were based on literature available on phototherapy and were set to: wavelength of 860 nm; frequency of 100 Hz; average power of 50 mW; power density of 50 mW/cm2; total emission area of 1 cm2; pulsed emission mode with 50% duty cycle; and dose of 4 J/cm2. The prototype was controlled by a software that estimated the time of application based on the selected dose. For a dose of 4 J/cm2 the calculated application time was 79 sec.
The therapist cleaned the participant`s nipple with a 0.9% physiologic solution and a brassiere with the LED prototype mounted on it was carefully adjusted to the participant's breast (Fig. 2B), with prototype A and B being used for participants of the experimental and control group, respectively. During phototherapy, the eyes of all participants were covered with protective goggles. The application of the LED phototherapy to participants in both groups was performed twice a week for a period of 4 weeks.
Evaluation of nipple lesions and image analysis
Photographs of each nipple lesion were obtained before application of the phototherapy in all sessions during the 4 weeks of therapy. The photographs were always taken by the same subject, blinded to the group the participant belonged to.
A Canon EOS Rebel XS (USA), 10.1 megapixels, with 18×55 mm lens, was used in the photographic sessions. Image acquisition was standardized by positioning the participant in a chair with the camera mounted on a tripod in front of her at a constant focal length of 25 cm. Photographs were taken in frontal view with a caliper placed close to the nipple lesion to allow for standardization of the length scale in the measurements of lesion area. The digital images obtained were analyzed by the software Quantikov, 24 which calculated lesion area based on the user's definition of the lesion boundaries (Fig. 3).

Lesion area demarcation with Quantikov image analyzer.
Evaluation of pain intensity
Pain intensity was measured by an 11-point pain intensity numerical rating scale (PI-NRS), 25 where 0 is equal to no pain and 10 is equal to severe pain. The PI-NRS instrument was applied to all participants in all therapeutic sessions, before and after phototherapy. A standard seven-point patient global impression of change (PGIC) instrument was applied, 2 in which the scale for “pain status” of the participant was: very much improved; much improved; minimally improved; no change; minimally worse; much worse; and very much worse. At the end of each session, the participants recorded their pain status in the PGIC scale. The association between specific PI-NRS change scores and clinically relevant pain reduction was evaluated and improvements were considered relevant when the associated PGIC categories of ‘much improved’ or better where recorded by the participant.
Statistical analysis
The statistical analysis was performed by nonparametric tests, with intra-group differences being assessed by the Wilcoxon test and Spearman correlation, and inter-group differences by the Mann–Whitney test. The Wilcoxon test was used to compare median values at the beginning and at the end of the therapeutic sessions for all groups on each outcome measured. The Spearman test was used to check whether or not there was a correlation between two variables. The Mann–Whitney test was used to compare median values from two independent groups. The level of significance in all tests was p<0.05 and statistics software used was SPSS 12.0 and MINITAB 14.
Results
There was no significant differences between the groups regarding age (p=0.46), postpartum time (p=0.19), or initial nipple lesion area (p=0.21) (Table 1).
Nipple lesion area analysis
There was significant reduction in area of nipple lesions in both the experimental and control groups with the increase in the number of therapeutic sessions (p<0.001). However, inter-group analysis showed a significant difference between the groups as the therapy progressed (p<0.001).
Figure 4 shows the evolution of nipple lesions, specifically in sessions 1, 4, and 8. Figure 4A–C shows a participant in the experimental group and Fig. 4D–F shows a participant in the control group. The participant in the experimental group had her initial trauma completely healed by the fourth therapeutic session (Fig. 4B); whereas the participant in the control group presented complete healing only at the eighth session (Fig. 4F).

Healing evolution of nipple lesions in a participant of the experimental group in the
A complete wound healing was attained in both groups by the end of intervention (8 sessions), as observed in Fig. 5. However, the nipple lesions in the experimental group (active phototherapy) healed faster than did the lesions in the control group (placebo phototherapy). Lesions in the experimental group were completely healed by the fourth session, whereas lesions in the control group were completely healed only by the eighth session.
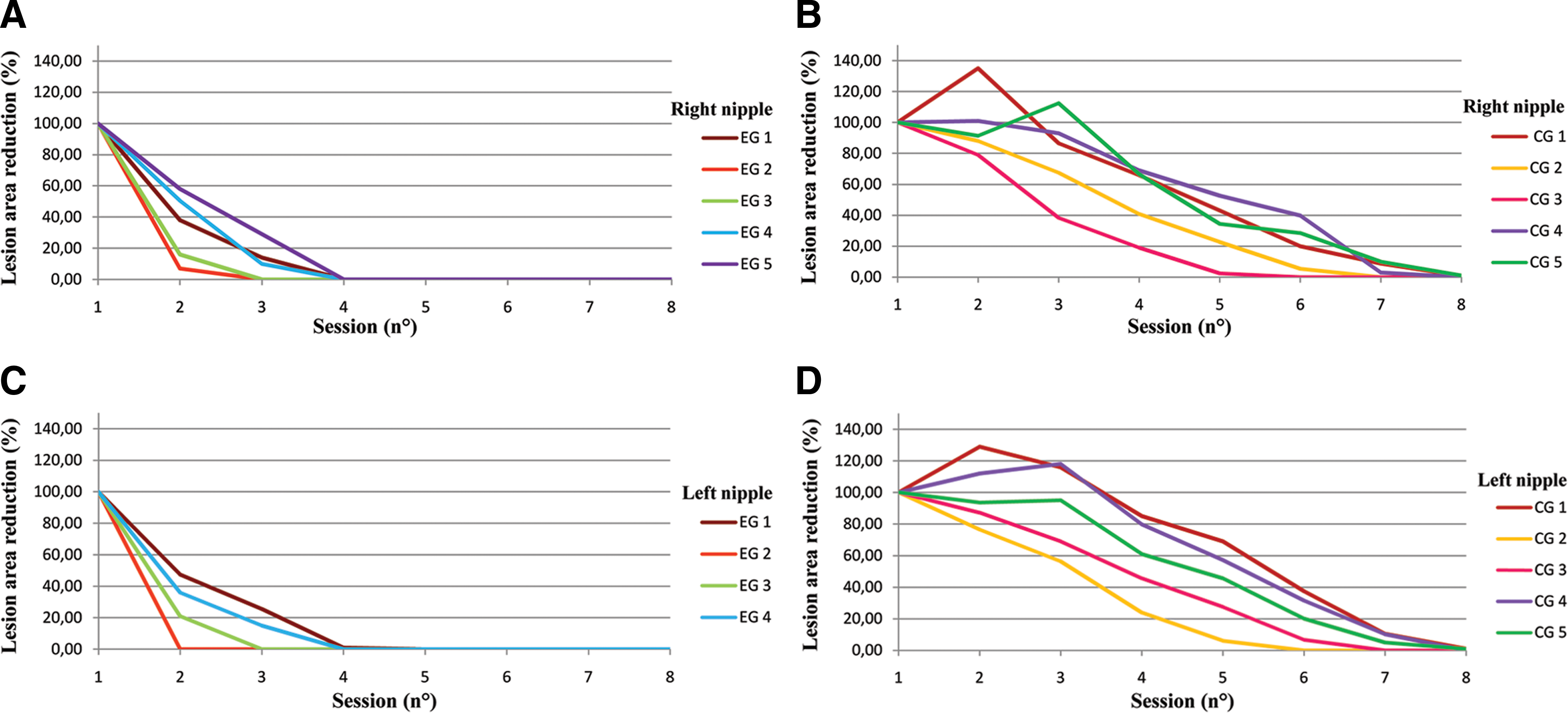
Percent reduction in area of the nipple lesions varying with intervention sessions:
Pain intensity analysis
The results for pain intensity, as measured by the PI-NRS, for both experimental and control groups in each therapeutic session, are presented in Table 2. The pain intensity, presented in the “median” column, decreased with the increase in the number of sessions for both experimental and control groups. The “median difference” represents the difference between measured pain before and after therapeutic session. For the control group, there was no difference between the pain at the beginning and at the end of the session. In regard to the experimental group, for a few sessions, the value for pain intensity at the end of the session was smaller than that at the beginning.
Although a reduction in pain intensity was observed for both groups after the end of the intervention, the intra-group statistical analysis indicated a significant reduction only for the experimental group (p=0.00). A significant difference was observed for pain intensity between the experimental and the control groups (p=0.03).
A change score of −1.0 on the PI-NRS was determined to be associated with a clinically relevant reduction in pain according to the recorded status in the PGIC scale, i.e., the majority of participants in the experimental group recorded their pain status as “much improved” at the end of all therapeutic sessions.
Discussion
A number of interventions for the therapeutic treatment of nipple trauma have been referred to in the literature; however, it is still unclear whether they are effective or not. 26 Therefore, further studies are needed in this area in order to promote a more effective therapeutic approach to the healing of nipple trauma, especially for those puerperal women for whom the prescribed treatments have failed to do the task. In this study, the clinical effects of LED phototherapy on the healing of nipple trauma were evaluated. To our knowledge, this is the first study to examine this kind of therapy for the healing of nipple trauma.
In this study, participants with nipple trauma associated with nipple pain were included, with the nipple lesions in both groups showing a significant reduction in area with the increase in the number of therapeutic sessions. This finding may be explained by the fact that both groups received the standard therapy, that is, orientations on correct breastfeeding technique and nipple care. This practice allowed for the removal of causal factors: inadequate positioning and attachment of the infant. 8 However, the experimental group showed significantly faster healing than the control group did over the course of the intervention period. Similar results were found in other studies, such as those of Caetano et al. 27 and Minatel et al., 28 in which they assessed the effects of LED light on the healing of venous and diabetic ulcers, respectively. In both studies, the ulcers from the experimental group showed faster healing than did those from the control group.
These results are in accordance to the reports in the published literature, which demonstrate that LED phototherapy accelerates wound healing in both animals and humans 29 –31 and that this acceleration is attributed to the physiologic effects caused by LED radiation, such as stimulation of ATP synthesis, increase in proliferation of fibroblasts and production of collagen, and stimulation of angiogenesis. 19,20,32,33
The acceleration of wound healing promoted by LED phototherapy brings benefits to breastfeeding and improves the mother–child relation, and the mother feels less pain and enjoys the breastfeeding practice. As a consequence, there is no early weaning. According to Akkuzu and Taskin, 34 nipple trauma and pain, as complications associated with breastfeeding, are considered the most significant factors precluding maintenance of breastfeeding in the first weeks of motherhood.
The results in our study also indicated pain reduction in both experimental and control groups with the increase in the number of sessions. The decrease in pain intensity in both groups may be related to the removal of causal factors by the standard treatment, leading to the closure of nipple lesions, which indirectly reduced nociceptive levels. Furthermore, it was also demonstrated that LED phototherapy promoted immediate analgesia, that is, pain was reduced immediately after application of light. These findings are consistent with other studies reporting analgesic effects of LED light. 35,36
The LED phototherapy prototype effects in reducing pain in this study were confirmed by statistical analysis. The analgesia observed may be attributed to changes in nerve conduction. 37 Other authors believe that pain slows the healing process probably caused by recruitment of inflammatory cells to the site of injury. 29 LED phototherapy alters the expression of genes involved in wound healing and, possibly, pain modulation. 16
A limitation of this study was the sample size. The small number of participants was mostly because of lack of commitment to the study by some of the originally recruited participants.
Conclusions
Overall, there were significant differences between experimental and control groups regarding the final outcome for wound healing and pain reduction associated with nipple trauma under LED phototherapy. The LED phototherapy successfully accelerated the healing of nipple lesions and reduced the pain intensity in the participants in the experimental group when compared to those in the control group who were subjected solely to placebo phototherapy and orientations on nipple care and adequate breastfeeding techniques. Advantages of this particular intervention are ease of application, cost effectiveness, and acceptance by lactating women.
Footnotes
Acknowledgments
The authors thank the Brazilian Government Agency FAPEMIG for financial support. The authors also thank Alexandre Gonçalves Teixeira, manufacturer of the LED phototherapy prototypes, and Edson Borges de Souza, MD, for their invaluable contributions to this work.
Author Disclosure Statement
No competing financial interests exist.