
Abstract
Introduction
Periodontopathogens include many bacterial species, among which the most aggressive are Porphyromonas gingivalis, Fusobacterium nucleatum, Eikenella corrodens, Treponema denticola and Aggregatibacter actinomycetemcomitans. 3 –5 These bacteria, through the release of multiple virulence and pathogenic factors, such as lipopolysaccharide (LPS), activate and sustain the host inflammatory response 6 eventually causing alveolar bone resorption. 7 Moreover, most periodontopathogenic bacteria are capable of binding to and entering gingival/buccal epithelial cells, where they can escape immune reaction and traditional antiseptic therapies. 8 –12 Recent evidence suggests that bacteria can internalize within epithelial cells not only of the periodontal pocket but also of the outer gingiva, 13 thus creating a microbial reservoir that can favor post-treatment relapses and chronicization of periodontitis. 14 –19
In the last decade, the application of laser medicine for the treatment of oral diseases has attracted considerable attention. Laser therapy offers several advantages over conventional surgical treatments, such as a noninvasive approach; selective targeting; repeatability; marked bactericidal effect; reduced pain, inflammation, and edema; improved and accelerated wound healing; and reduced need for antibiotics and local anesthetics. 20,21 Growing evidence indicates that Nd:YAG, Er:YAG, CO2, and diode lasers in photoablative mode can be used for the treatment of inflammatory periodontal diseases. 20 –24 In particular, Er:YAG is also effective for removing calculus and debris adherent on the root surface. 21 In principle, laser treatment should be capable of effectively targeting periodontal tissues infected by bacteria, including the epithelial sanctuaries. 25 On the basis of these beliefs, in the present study we analyzed and compared the bactericidal and morphological effects of different laser devices widely used in medicine and dentistry [diode GaAs (λ 810 nm), erbium- or neodymium-doped yttriumaluminum-garnet (Er:YAG, Nd:YAG), and carbon dioxide (CO2) lasers], in the gingiva outside the periodontal pocket of patients treated with conventional therapy for chronic periodontitis.
Methods
Subjects
Sixteen patients (10 males and 6 females; 40–65 age range; mean range 55.6 years) with moderate-to-severe chronic periodontitis were included in this study. The protocol was designed in compliance with the ethical guidelines of the Declaration of Helsinki, as amended in Edinburgh in 2008, and was approved by the Ethical Committee of the Faculty of Medicine, University of Florence, Italy. The patients underwent a screening visit during which they gave written informed consent to their enrollment in the study. Exclusion criteria were: systemic diseases (diabetes mellitus, cancer, HIV, metabolic and endocrine diseases), pregnancy and lactation, chronic high-dose steroid therapy, radiation or immunosuppressive therapy, heavy smoking (more than 10 cigarettes/day), orthodontic treatments, extensive carious lesions, and antibiotics taken within the 6 months preceding the study. The enrolled patients were visually examined and the depth of periodontal pockets was measured with a conventional manual periodontal probe (Hu-Friedy, Chigago, IL) at six sites per tooth. Clinical measurements included: clinical attachment level (CAL), pocket probing depth (PD), and gingival index and bleeding on probing (GI/BOP).
Conventional periodontal treatment
The patients were subjected to supragingival and subgingival scaling and root planning (SRP) with a combined use of hand (Hu- Friedy, Chicago, IL) and ultrasonic instruments, under local anesthesia. During SRP, a subgingival irrigation with chlorhexidine (CHX; 0.3% in water, 10 mL per quadrant for an approximate period of 5 min for each selected site) was performed, followed by gentle brushing with a sterile gauze rinsed in 0.3% CHX for supragingival antisepsis. The patients received oral hygiene instructions corresponding to their individual needs.
Cytodiagnostic assay
Before laser irradiation, samples of exfoliated cells were taken from each patient in proximity to the free gingival margin with a sterile microcurette and processed for cytodiagnostic fluorescence analysis, as detailed previously. 6 Briefly, the LIVE/DEAD BacLight™ bacterial viability kit (Invitrogen Molecular Probes, Milan, Italy), originally developed to monitor the viability of micro-organisms through the evaluation of integrity of bacterial membranes, 26 was used. By this method, dead bacteria stained red, whereas the viable ones stained green. This method allowed us to detect additional diagnostic parameters, such as the occurrence of inflammatory leukocytes, erythrocytes, and altered gingival epithelial cells. 6 The collected material was smeared on a histological slide, fixed in 90% ethanol, air dried and stained with 1 mL of the fluorescent dye solution for 2 min at 37° C. After thorough rinsing in distilled water, the samples were immediately observed under a Leica 4000B fluorescent microscope (Leica Microsystems, Milan, Italy). The results were combined with the standard clinical parameters to obtain an objective, semiquantitative scoring of disease severity, as reported in Table 1. Some samples were also examined by a Leica TCS SP5 confocal microscope (Leica Microsystem, Mannheim, Germany) to detect the exact cellular location of bacteria. To this aim, a series of optical sections, 0.4 μm thick, were taken through the depth of the cells and projected onto a single image.
CAL, clinical attachment level; PD, probing depth; GI, gingival index; II, inflammatory infiltrate; DE, damaged epithelium; PMN, polymorphonuclear leukocytes; MN, mononuclear leukocytes; RBC, erythrocytes; DEC, damaged epithelial cells.
Photoablative laser treatments
To remove the contaminated periodontal tissues, the patients were laser irradiated on the inner and outer free gingiva using the following devices: 1. Er:YAG (OpusDuo ECTM, Lumenis, Milan, Italy) 2. CO2 (OpusDuo ECTM, Lumenis) 3. Nd:YAG (Pulse Master 600 IQ, American Dental Technologies Inc., Corpus Christi, TX) 4. Diode laser (4x4 Dental Laser, General Project, Montespertoli, Italy)
The irradiation parameters, chosen on the basis of those widely accepted for the treatment of periodontitis, 6,27,28 are specified in Table 2. Energy output of the lasers was measured with a power meter before each procedure. Eye protection of the operator, assistant, and patients was assured by wearing safety glasses. Treatments were performed with the patient under local anaesthesia (articain HCl, Ultracain, Frankfurt, Germany) in all circumstances for Er:YAG and CO2 lasers, and only on patient's request for diode and Nd:YAG lasers. Air flow cooling was used to minimize the photothermal effects of laser irradiation. Of note, laser therapy was performed by expert operators (M.G., L.L.) who were not involved in the subsequent analysis of data.
Biopsy collection and morphological analysis
Upon admission and after laser treatments, small biopsies of gingival soft tissues, ∼2×2 mm, including surface epithelium and lamina propria, were taken with the patient under local anesthesia (articain HCl) using a biopsy punch, 2-mm diameter, from the buccal aspect of the gingiva, taking care not to expose the marginal alveolar bone and periostium. Usually, biopsies were taken at the oral sites in which there was a therapeutic indication to reduce the periodontal pockets: hence, their number and tooth site varied from patient to patient. The biopsies [n=32, with 16 taken before and 16 (4 per laser type) after laser treatments] were fixed by immersion in 4% (w/v) formaldehyde in 0.2 M phosphate-buffered saline, pH 7.4, dehydrated in graded ethanol, and embedded in paraffin. Five μm-thick sections were stained with hematoxylin and eosin, viewed, and photographed under a light microscope (Nikon, Tokyo, Japan). Semiserial sections of each sample were made and submitted to immunohistochemistry to reveal intercellular cell adhesion molecule (ICAM)-1 expression by the vascular endothelium, using a mouse monoclonal anti-human ICAM-1 antiserum (Santa Cruz Biotechnology, Santa Cruz, CA; 1:200) and goat anti-mouse Alexa-488-conjugated IgG (Molecular Probes Inc., Eugene, OR; 71:200). The immunostained samples were counterstained with propidium iodide (Molecular Probes) and observed under the Leica TCS SP5 confocal microscope. Some small gingival samples were also fixed in 4% cacodylate-buffered glutaraldehyde, post-fixed in 1% phosphate-buffered osmium tetroxide, dehydrated in graded ethanol, and embedded in EPON® 812 epoxy resin. Ultrathin sections, 0.7 μm thick, and stained with uranyl acetate and lead citrate, were examined under a JEM 1010 electron microscope (Jeol, Tokyo, Japan) at 80 kV.
Quantification of bacteria by real-time polymerase chain reaction (PCR) analysis
Genomic DNA was entracted from formalin-fixed paraffin-embedded histological sections according to the RecoverAll Total Nucleic Acid Isolation Protocol (Ambion-Applied Biosystems, Foster City, CA). Slides were kept in xylene for 10 min at 50°C and air dried for 10 min. Tissue sections were detached from slides by scraping, collected in Eppendorf tubes, incubated in xylene at 50°C for 3 min to remove paraffin from the tissue, and centrifuged at 13,000 rpm for 5 min at room temperature. The supernatant was discarded and the pellet washed twice in 96% ethanol. Pellets were treated with the digestion buffer and protease following manufacturer's instruction for 48 h: as indicated in the protocol, increasing the incubation time up to 48 h at 50°C usually resulted in recovery of DNA with increased functionality. RNAse was added to tubes transferred from 50°C to room temperature for 1 h. On these samples, genomic DNA was extracted with phenol/chloroform method and spectrophotometrically quantified with NanoVue Plus Spectrophotometer (GE Healthcare, Milan, Italy). The numbers of 16S rDNA-gene copies of P. gingivalis, A. actinomycetemcomitans, F. nucleatum, T. denticola, Prevotella intermedia, and E. corrodens, 16S rDNA-gene copies of total bacterial cells and human DNA copies were quantified using SsoFast EvaGreen Supermix (Bio-Rad, Milan, Italy) following manufacturer's instructions. All reactions were performed in a final volume of 15 μL containing 10 ng of total genomic DNA (5 μL of sample at 2 ng/μL) and primers at 300 mM final concentration, using CFX96 Cycler (Bio-Rad) programmed as follows: 2 min 98°C for initial heat activation, 40 cycles of 5 sec at 98°C for denaturation, and 20 sec at 60°C for annealing/extension steps. Melting curves were also collected in the temperature range 65–95°C. Negative controls without DNA and standard samples were included in each real-time plate. Data were analyzed to provide an estimate of the total number of bacterial cells. When a gene was used as target for quantification of a specific bacterium, we assumed that the 16s rDNA gene copy numbers and overall genome size were basically similar among the different bacteria analyzed. 29,30 The standard curves for each bacterial strain were built on serial 5× dilutions, starting from 10 ng of species-specific genomic DNA (DSM, Milan, Italy), corresponding to nearly 10-4×106 cells The standard curves were performed in triplicate and quality parameters were analyzed systematically. The DNA starting quantity determined by comparing cycle threshold (Ct) values with standard curves were converted to theoretical bacterial numbers, normalized to human DNA.
Results
Pretreatment
Histological and cytodiagnostic analysis of the gingival samples taken outside the periodontal pocket (Fig. 1) in periodontitis patients performed before the treatment showed marked abnormalities. The histological changes mainly consisted of: focal epithelial ulceration, diffuse infiltration of inflammatory cells in the lamina propria, and dilated blood vessels (Fig. 2A). By confocal microscopy, the endothelial lining of capillaries and post-capillary venules showed a marked immunostaining for ICAM-1, a typical endothelial adhesion molecule regulating leukocyte trafficking during inflammation (Fig. 3A). The morphological damage was associated with severe bacterial contamination of the gingival tissues, as judged by real-time PCR analysis (Fig. 4A,B). In particular, high DNA levels of periodontopathogenic species, namely P. gingivalis, A.actinomycetemcomitans, F. nucleatum, T. denticola, P. intermedia, and E. corrodens, were detected in all the samples. In particular, the cytofluorescent analysis performed on exfoliated gingival epithelial cells showed numerous bacteria (cocci, bacilli, spirochetes), located both at the cell surface and within the cytoplasms, as well as several erythrocytes and polymorphonuclear leukocytes (Fig. 4A,B). Of note, the presence of intracellular bacteria endowed into gingival 9 epithelial cells was further confirmed by confocal and transmission electron microscopy (Fig. 5C,D).
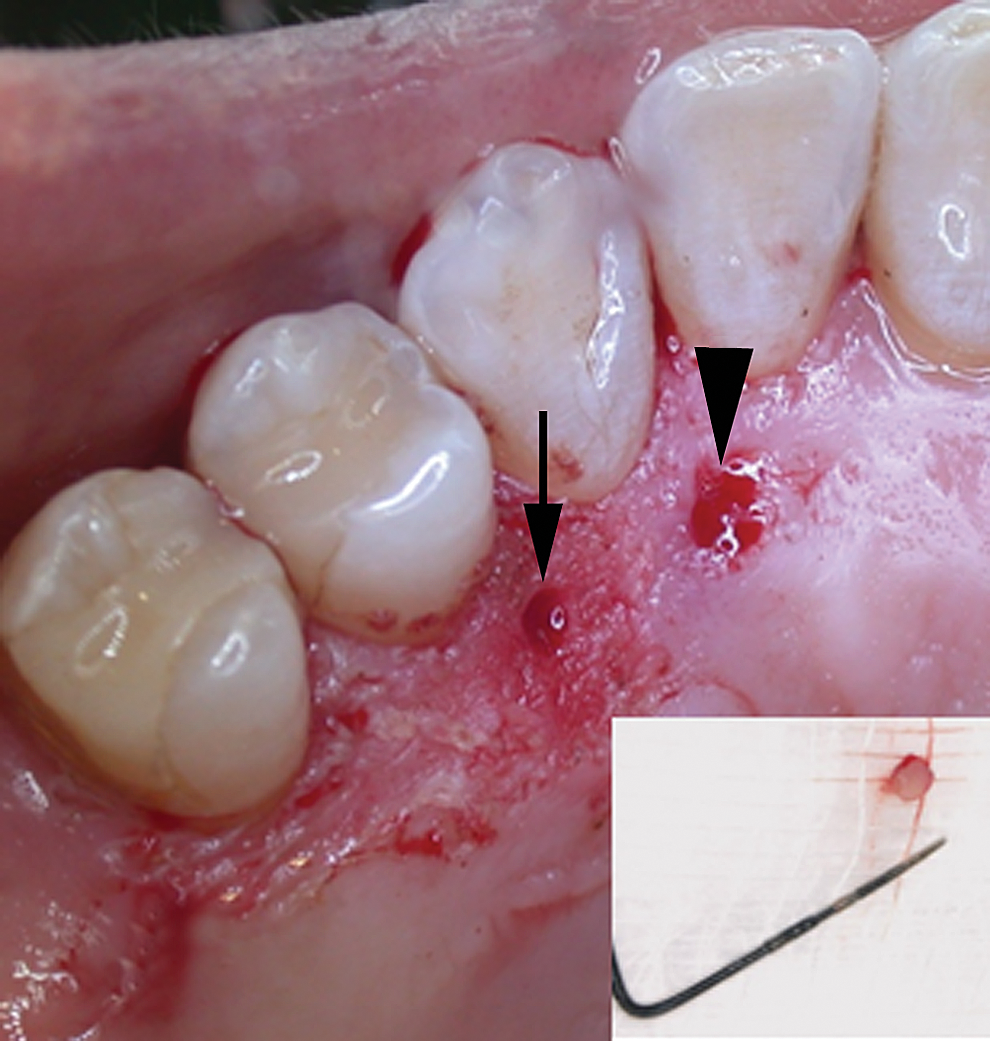
Representative image of gingival biopsy sites in a diode laser-treated (arrow) and untreated area (arrowhead). Inset: detail of the biopsy specimen.
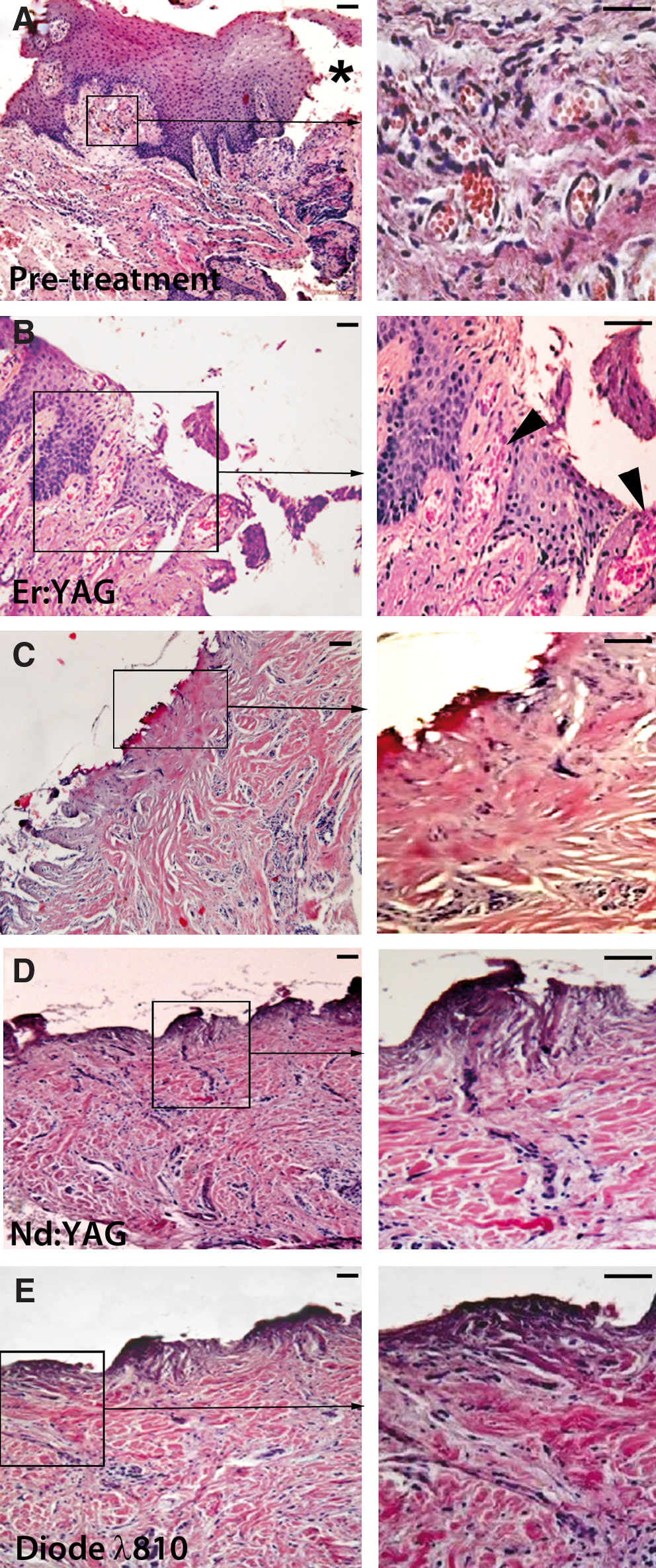
Histopathological analysis of gingival tissue biopsies taken
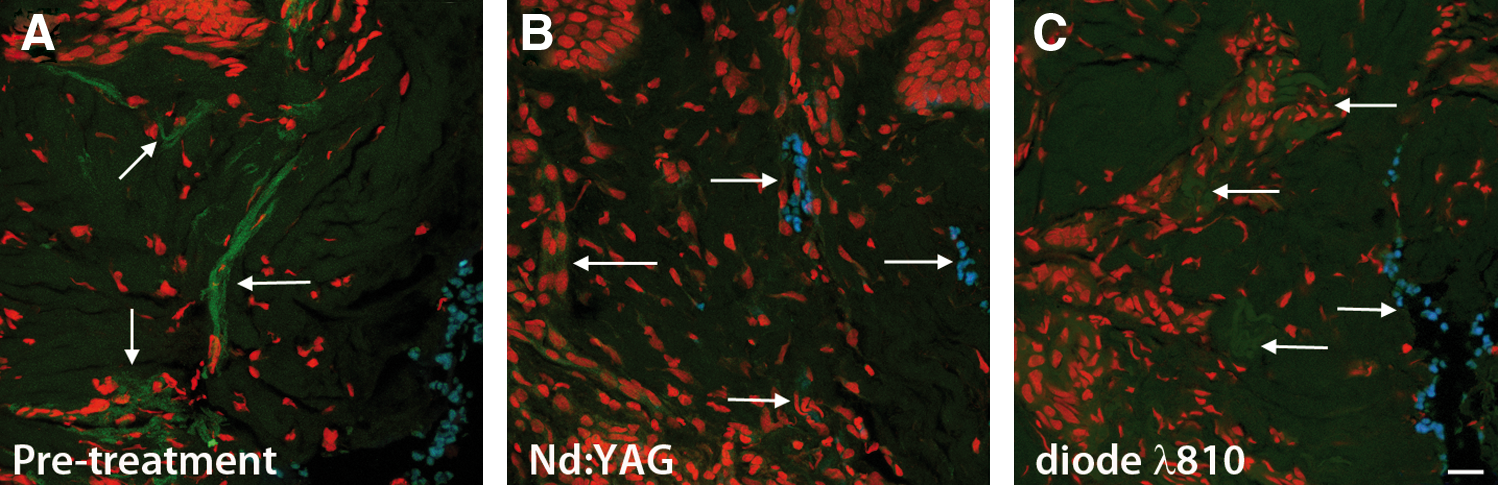
Confocal immunofluorescence analysis of ICAM-1 expression by gingival microvessels (arrows)
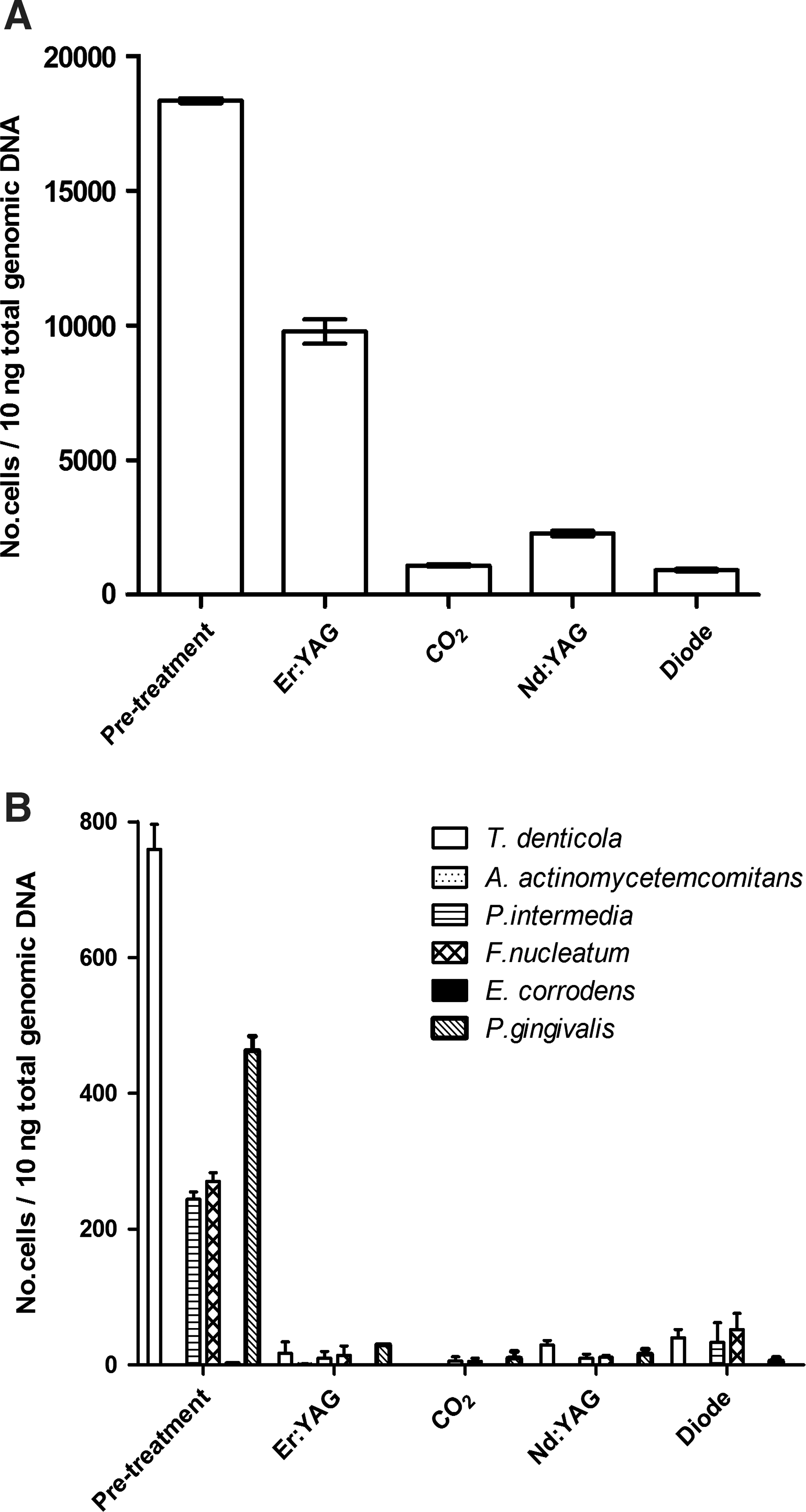
Real-time polymerase chain reaction (PCR) of
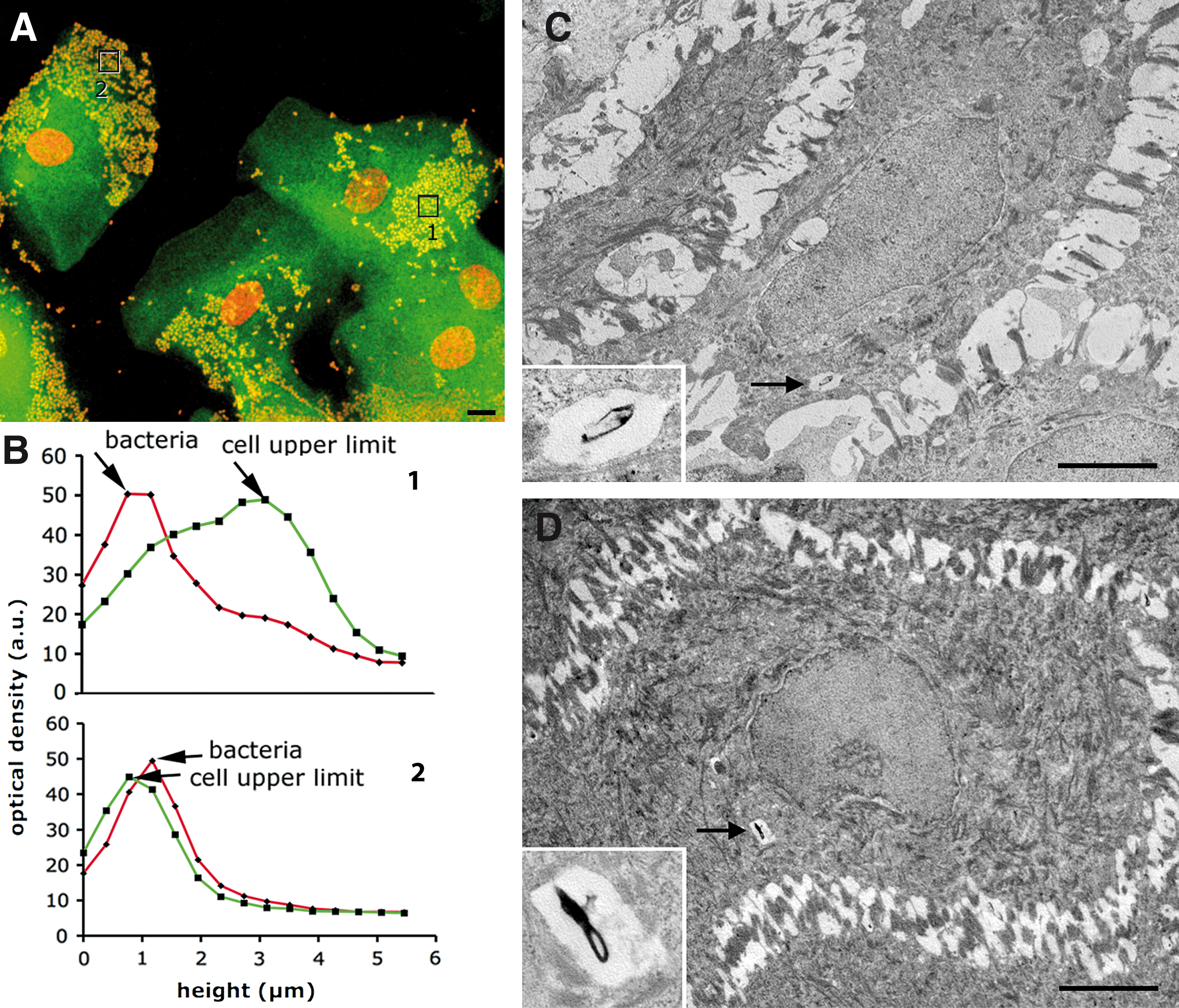
Cytodiagnostic analysis (left panels) and transmission electron micrographs (right panels) of gingival epithelial biopsies taken before laser irradiation.
Laser treatment
Histological and cytodiagnostic analysis of the gingival samples from the patients, which were performed after photoablative laser irradiation, showed an almost complete eradication of bacterial contamination, in terms of total bacterial and specific periodontopathogenic DNA (Fig. 4A,B). However, substantial histological differences were observed among the different laser devices used. In particular: 1. Er:YAG laser caused an incomplete ablation of the gingival squamous epithelium associated with dilatation and rupture of the underlying blood microvessels (Fig. 2B). This finding was consistent with the sustained bleeding observed during the treatment. 2. CO2 laser yielded a complete removal of the squamous epithelium accompanied by a diffuse heat-induced coagulation of the papillary connective tissue and microvessels (Fig. 2C). 3. Nd:YAG laser also caused a complete removal of the squamous epithelium, in the absence of appreciable changes of the stromal and microvessel components of the lamina propria (Fig. 2D). Of note, microvessels appeared collapsed, consistently with reduced bleeding at treatment, and showed a significant reduction of ICAM-1 expression (Fig. 3B). 4. The diode laser (λ 810 nm) yielded similar effects as those of the Nd:YAG laser, inducing a complete ablation of the surface epithelium, prominent microvessel constriction associated with ICAM-1 downregulation, and negligible stromal coagulation (Figs. 2E and 3C). Even in this case, intraoperative bleeding was minimal.
Discussion
There is a general consensus that periodontopathogenic bacteria can invade host gingival epithelial cells and establish an intracellular niche, which is critical for their survival mechanisms. This relationship with the host cells is initially innocuous, but can potentially became dangerous, being the prerequisite for the spreading to neighboring cells. 13,15,25 This is a crucial issue in periodontology, because the silent persistence of periodontopathogens within oral epithelial cells surrounding the gingival pocket, ostensibly uninvolved in the disease at clinical observation, can explain the frequent post-treatment relapses and the need for extended oral decontamination. 8,11,14 Although laser treatment has generated considerable interest among dentists and the public, there is still substantial controversy on the actual clinical efficacy of laser treatment over SRP and conventional surgical curettage for the therapy of chronic periodontitis. 10,20,31 –33 This controversy likely exists for two main reasons: (1) the use of non-univocal laser irradiation protocols, such as different wavelengths and setting parameters, which do not allow a reliable comparison of results; 20,32,33 and (2) the fact that most of the previous studies limit the laser treatment to periodontal pocket curettage, 31,32 which has been recently stated to be substantially ineffective in a consensus report of the American Academy of Periodontology. 34 In such a view, the data of the present study provide evidence that periodontopathogens, such as P. gingivalis, A.actinomycetemcomitans, F. nucleatum, T. denticola, P. intermedia, and E. corrodens, can persist into the epithelial cells outside the periodontal pocket of patients treated with conventional therapy for chronic periodontitis, and that laser treatment is suited to achieve de-epithelization of the infected gingiva. Moreover, combining the microbiological data and morphological analysis, we have compared the effects of the different laser treatments to define the most appropriate irradiation protocols for successful bacterial removal with minimal tissue damage. We found that Er:YAG, although being adequate to control microbial contamination, caused prominent blood vessel dilatation associated with marked bleeding at treatment. This vascular modification could favor the systemic spread of periodontopathogenic bacteria and their harmful by-products (such as LPS), which represent a major concern in the treatment of periodontitis, as they may predispose the patients to cardiovascular disease. Indeed, recent clinical studies have reported the presence of P. gingivalis DNA and rRNA in carotic and coronary atherosclerotic plaques, 35 and there is in vitro evidence that P. gingivalis-derived LPS promotes leukocyte adhesion to vascular endothelial cells. 36 Moreover, Er:YAG laser failed to completely and selectively ablate the gingival epithelium, accounting for the persistence of intracellular bacteria in the remnant gingival tissue. On the other hand, CO2 laser, although being capable of achieving a complete de-epithelization, caused heat-induced coagulation of the papillary connective tissue and microvessels, thus delaying gingival healing and representing a favorable substrate for bacterial re-growth.
Among the tested devices, the Nd:YAG and diode (λ 810 nm) lasers gave the best results. At the reported irradiation parameters, both instruments yielded a complete removal of the gingival surface epithelium, without causing major signs of stromal damage and microvessel dilation. These features indicate that Nd:YAG and diode lasers are capable of removing the epithelial sanctuaries, which represent a barrier against traditional antisepsis methods and host immunity defenses. Of note, epithelial removal by Nd:YAG and diode laser irradiation was accompanied by microvessel constriction, possibly related to direct vasomotor effects and/or deactivation of local pro-inflammatory cytokines by laser light. 37,38 This feature provides obvious clinical advantages, as it can prevent bleeding, reduce the chances for systemic bacterial spreading during the treatment, and favor the formation of a dry surgical field for direct visual control in deep pockets and better access for SRP procedures. Moreover, compared with the pretreatment findings, Nd:YAG and diode lasers were capable of reducing ICAM-1 immunolabelling by the vascular endothelium. This finding, together with our previous observation that Nd:YAG and diode lasers are capable of inactivating bacterial LPS, 28,39 a potent pro-inflammatory mediator, further underscore that Nd:YAG and diode lasers, by reducing endothelial activation and leukocyte extravasation into the gingival stroma, can exert prominent anti-inflammatory effects on the gingival/periodontal tissue.
Conclusions and Summary
The present findings show that Nd:YAG and diode lasers are effective for the immediate removal of the contaminated gingival epithelium outside the periodontal pocket in patients with chronic periodontitis, and suggest that, when used as a complement to conventional therapy, they may be adequate to attain periodontal health and reduce the incidence of post-treatment relapses. Future long-term, clinical trials are needed to support the efficacy of Nd:YAG and diode laser as an adjunctive therapeutic approach to periodontal disease.
Footnotes
Author Disclosure Statement
Lucia Formigli was recipient of a research grant from General Project, Montespertoli, Italy. The other authors have no conflicts of interest to disclose.