
Abstract
Introduction
The Er:YAG laser at 2.94 μm is a promising alternative technique for cavity preparation and caries tissue removal. Based on a thermally induced mechanical ablation process, the removal of hard dental tissues is enabled by microexplosions 8 without any thermal changes to the surrounding tissue. 9 Substituting rotating instruments with laser technology has its advantages, such as reduced pain 10 and decreased noise and vibrations 11 during cavity preparation. Furthermore, Er:YAG laser is selective in caries removal because of the high absorption in the humid caries tissue, which allows a conservative caries excavation without extending the preparation into the sound tooth structure. The additional advantage is that the Er:YAG laser creates a surface that appears similar to acid-etched surfaces, 12 which should be favorable for bonding procedures.
Another possibility for caries removal is a modification of the Er:YAG laser with fluorescence. This fluorescence feedback-controlled Er:YAG laser is a combination of a diagnostic device and the Er:YAG laser, which removes caries tissue selectively and perserves the healthy tissue. Within this system, the removal of dental hard tissues by the Er:YAG laser is controlled by the fluorescence signal from the tooth surface induced by the red-infrared indium gallium phosphate diode diagnostic laser. 13 The excitation wavelength induces a fluorescence signal that has been assigned to a protoporphyrin, a bacterial breakdown product. 14 An internal analysis unit calculates the intensity of the fluorescence light in the range from 0 to 100. A sensor for the detection of fluorescence radiation of the dentinal tissue indicates whether any infected caries in dentin is still present in the cavity, depending upon the threshold level (values from 0 to 100). The threshold level determines the end point of caries removal and the laser cannot emit beyond the indicated threshold level.
However, the lower ablation rates of the early Er:YAG lasers in comparison with the mechanical bur presented a limitation of their use in dental practice. 4,10,15 –18 The introduction of the Variable Square Pulse technology (VSPt) enabled ablation rates even higher than those obtained with a mechanical hand piece. 19,20 With the VSPt-based Er:YAG laser, at high energies and low pulse durations, the speed of ablation is faster than the difussion of heat into the tissue, enabling a “cold” and efficient ablation. 19
The present in vitro study aimed to evaluate the ablation rate of caries in dentin with fluorescence-feedback controlled Er:YAG, VSPt-based Er:YAG working in different pulse durations, and steel bur.
Materials and Methods
Sixty human molar teeth with caries in dentin, extracted for periodontal reasons, were selected for this study. The teeth were thoroughly cleaned of all residual debris using brushes and currettes and stored in physiological saline until use. All selected teeth were randomly divided into five groups, each containing 12 specimens: (1) Group FFC, fluorescence feedback-controlled Er:YAG laser, Key III, (KaVo, Biberach, Germany). Er:YAG laser, Fidelis Plus II (Fotona, Ljubljana, Slovenia) was used for three experimental groups: (2) Group SSP (Super Short Pulse: 50 μs); (3) Group MSP (Medium Short Pulse; 100 μs); (4) Group SP (Short Pulse; 300 μs). The control group was: (5) Group SB, steel bur in a slow-speed hand piece.
Fluorescence-feedback controlled Er:YAG laser
The pulse energy was set at 350 mJ for the enamel preparation and at 250 mJ for the dentin preparation. The pulse duration was 400 μs and the pulses were applied using a repetition rate of 10 Hz. The energy density for the enamel was 54.7 J/cm2/pulse and for the dentin was 39.1 J/cm2/pulse. During laser preparation, hard dental tissues were moistened with continuous water irrigation at a rate of 3 mL/min. The contact handpiece (No 2063, KaVo) with a spot size of 0.9 mm in diameter was used for caries removal. The threshold level was set at 7. All parameters were chosen according to the manufacturer's instructions.
Fidelis Plus II laser
A second generation Fidelis Plus II Er:YAG (Fotona, Ljubljana, Slovenia) laser was used for caries excavation in three experimental groups. Cavities were prepared using different pulse durations for each group of teeth: SSP (super short pulse: 50 μs), MSP (medium short pulse; 100 μs), and SP (short pulse; 300 μs). The pulse energy was 350 mJ for the enamel and 250 mJ for the dentin, with a pulse repetition rate of 10 Hz. The energy density for the enamel was 54.7 J/cm2/pulse and for the dentin was 39.1 J/cm2/pulse. The Er:YAG laser energy was delivered by a non-contact RO2-C hand piece with a spot size of 0.9 mm in diameter, under continuous water spray (3 mL/min) at a focus distance of 7 mm from the target point. All parameters were chosen according to manufacturer's instructions.
Low-speed hand piece apparatus
The enamel was opened with a fissure diamond drill (S 68535KR 090, Komet/Gebr. Barasseler, Lemgo, Germany) 0.9 mm in diameter with diamond particles 125 μm in size. The rotation speed was 300,000 rpm. Caries in dentin was removed with a round steel bur (310 104 1.104.009 Komet/Gebr. Barasseler, Lemgo, Germany) 0.9 mm in diameter. The bur rotation was 30,000 rpm. The hand piece was operated and controlled by the dental unit (Kavo Primus, 1058 S/TM/C/G, Biberach/Riss, Germany).
Treatment procedure
During the treatment, all the teeth were fixated. The caries removal for groups SSP, MSP, SP, and SB was performed under visual control, by testing the hardness of the remaining tissue with a dental probe. The caries excavation procedure was considered completed after the dental probe was able to induce a sharp sound and was not able to penetrate dentin. In the FFC group, the laser stopped emitting the laser beam when the fluorescence radiation of the dentinal tissue was beyond the previously set threshold level (7), and this was considered the end point of the caries excavation. A stopwatch (Motorola C 139, Schaumburg, IL) was used to measure the time needed for caries excavation for each experimental group. The time needed for the removal of the enamel, visual and tactile inspection, or the changing of the energy settings on the control panel of the laser apparatus were recorded separately.
Volume measurement apparatus and methods
The cavity volumes were measured before and after the caries excavation for each specimen with a laser triangulation profilometer, constructed at the School of Mechanical Engineering (University of Ljubljana, Slovenia). A profilometer system consists of: a laser projector, a digital camera, a movable table and a computer unit (Fig. 1). The profilometer can measure 80 cross-sections per second with an accuracy of 0.02 mm. After measuring the cross-sections of all the cavities, their volumes are determined using a specially designed computer program. A non-uniform, rational B-spline (NURBS) surface, representing the tooth surface prior to cavity formation, is approximated onto the already measured cavity cross-sections. The NURBS surface is a mathematical model commonly used in computer graphics for generating and representing curves and surfaces. The computer program determines cavity volumes by comparing the NURBS and cross-section surfaces. The accuracy of this measurement method is 5%. The results are presented by a computer program as a three-dimensional (3D) image. Measured cavities are differently colored depending upon their depth. Negative and positive volumes are given beside the 3D image of the tooth and cavity. The negative volume is the missing volume of the tooth after the laser or bur preparation, taking into consideration the NURBS surface. The positive volume is the least possible, because this is the remaining volume of the NURBS surface after the cavity preparation. The final cavity volume was gained by subtracting the aforementioned two volumes. The final volume of excavated caries tissue is calculated by subtracting the volume of the cavities before and after the caries removal.
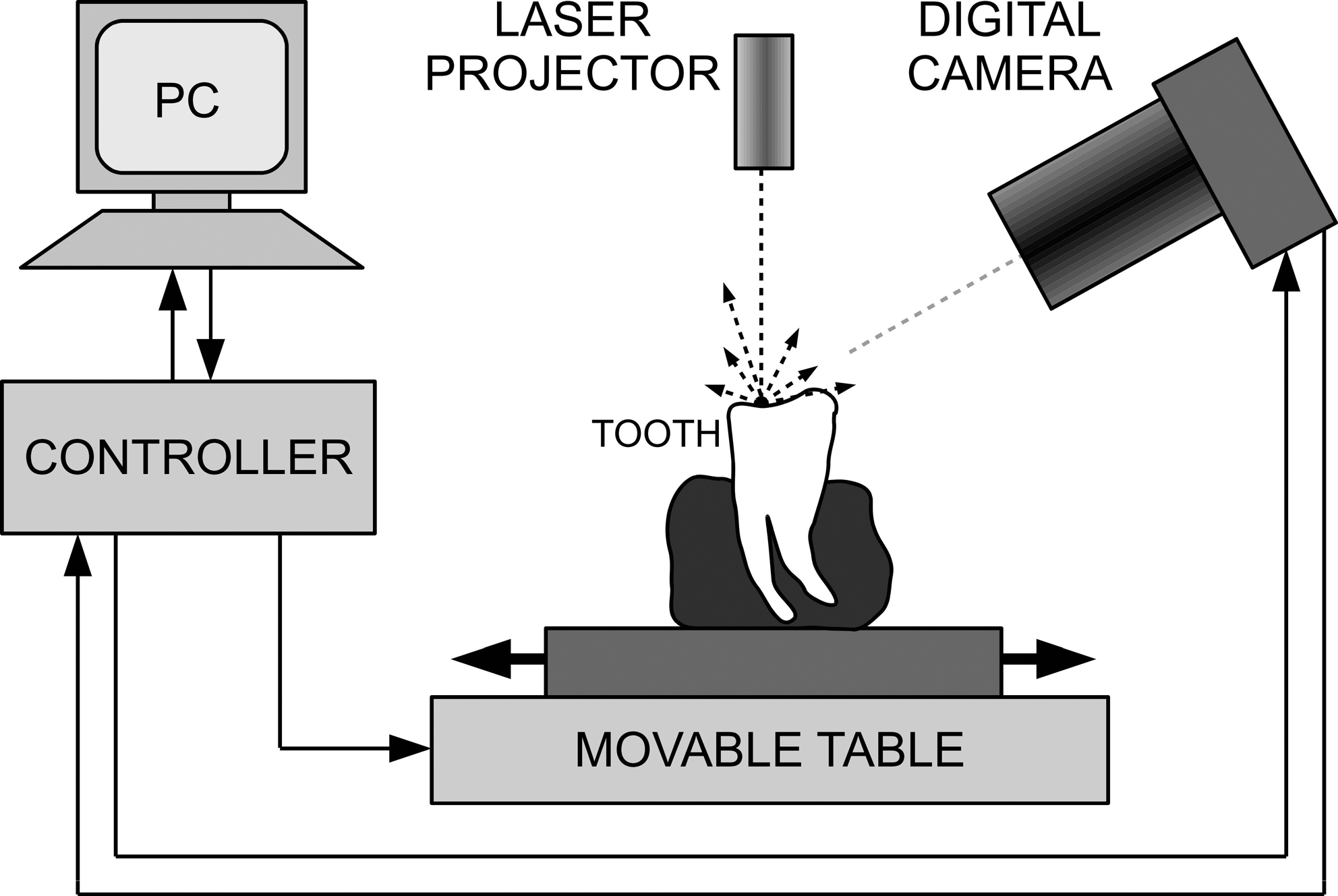
Measurement of cavity volumes with a laser triangulation profilometer.
Calculation of real and clinical ablation rate
The real ablation rate was calculated by dividing the volume of ablated hard dental tissue by the time needed for caries tissue removal. The clinical ablation rate was calculated by dividing the volume of ablated hard dental tissue by the sum of time needed for caries tissue removal, time needed for removal of enamel, visual and tactile inspection, or changing of energy settings on the control panel of the laser apparatus. The ablation rate was measured in mm3/sec.
Scanning electron microscopic (SEM) observation
Two specimens from each experimental group were selected randomly and subjected to SEM examination. For the SEM observation, samples were cleaned in an ultrasonic bath for 5 min. The interface was brought into relief by etching with a 32% silica-free phosphoric acid (Bisco, Schaumburg, IL) for 30 sec, washed with de-ionized water and air dried. Samples were dehydrated in an ascending ethyl alcohol series (25%, 50%, 70%, 80%, 90%, and absolute alcohol) and dried using hexamethyldisilazane (HMDS, Carlo Erba, Rodano, Italy). Specimens were then mounted on aluminum stubs, coated with a 15–20 nm thick layer of gold with a SC7620 Sputter Coater device (Polaron Range, Quorum Technologies, England) and inspected by SEM (JSM-6060LV, JEOL, Tokyo, Japan).
Statistical analysis
For the statistical analysis, the data were compared with the one-way ANOVA and post-hoc least significant difference (LSD) test. The level of significance was set at 5%. Statistical analysis was performed using Statistica 7.0 (StatSoft, Tulsa, OK).
Results
Caries dentin ablation
The volumes of the ablated caries dentin in SSP and SB group were statistically significantly different in comparison with other experimental groups (p<0.05), (Fig. 2). There was no statistically significant difference in volume of the ablated caries dentin between the SSP and SB groups (p>0.05), or between the FFC, MSP, and SP groups (p>0.05), (Fig. 2).
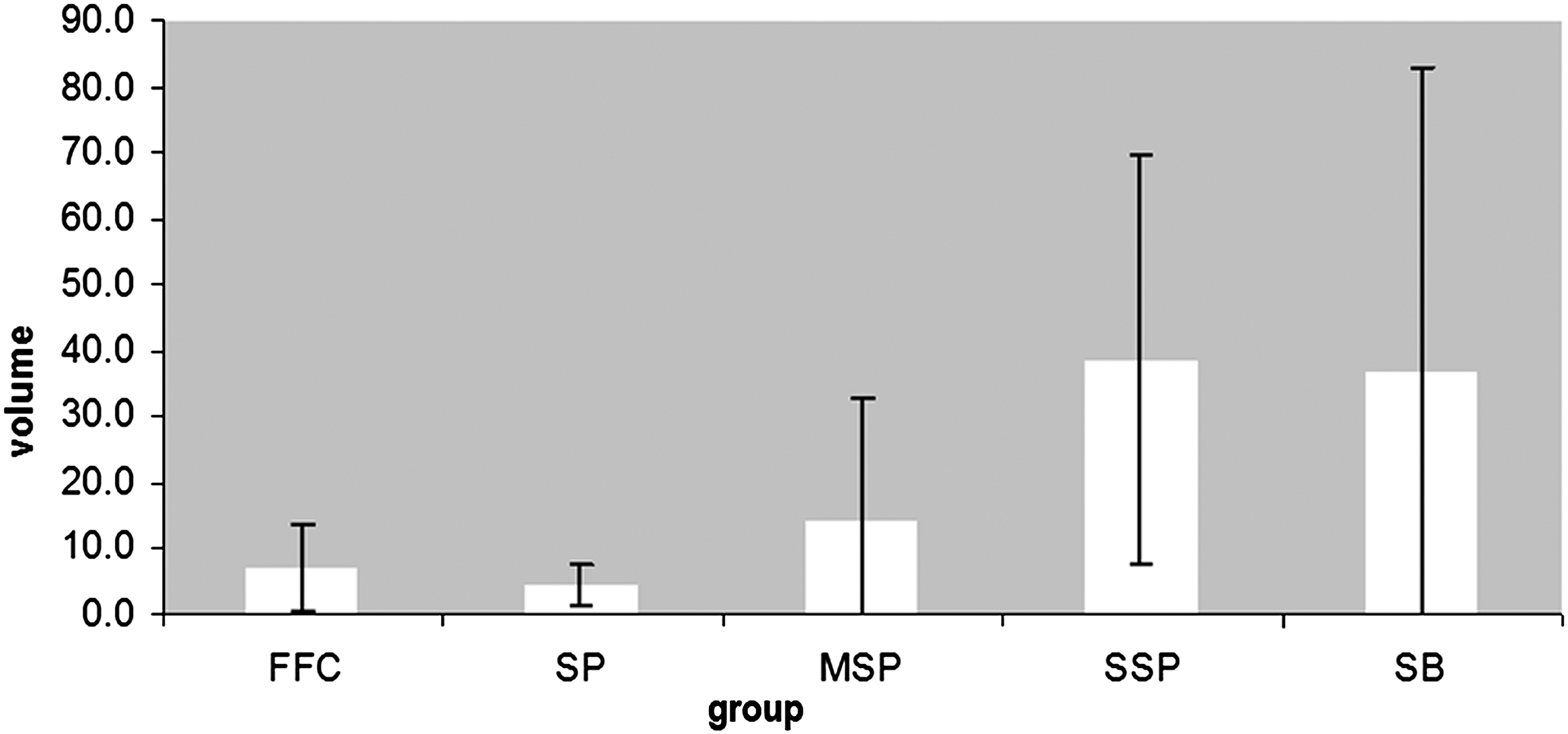
Volume (in mm3) of ablated caries dentin in the FFC, SP, MSP, SSP, and SB groups. SSP and SB groups are statistically significantly different in comparison with other experimental groups (p<0.05).
The clinical and real ablation rate of caries dentin was highest for the SSP group (0.15±0.05 and 0.17±0.05 mm3/sec, respectively) and statistically significantly different in comparison with the MSP and SB groups (p<0.05), (Figs. 3 and 4). There was no statistically significant difference in ablation rates between the MSP and SB groups (p>0.05), (Figs. 3 and 4). The MSP and SB groups showed higher ablation rates than did the SP and FFC groups (p<0.05), whereas no statistically significant difference was found for the SP and FFC groups (p>0.05) (Figs. 3 and 4).
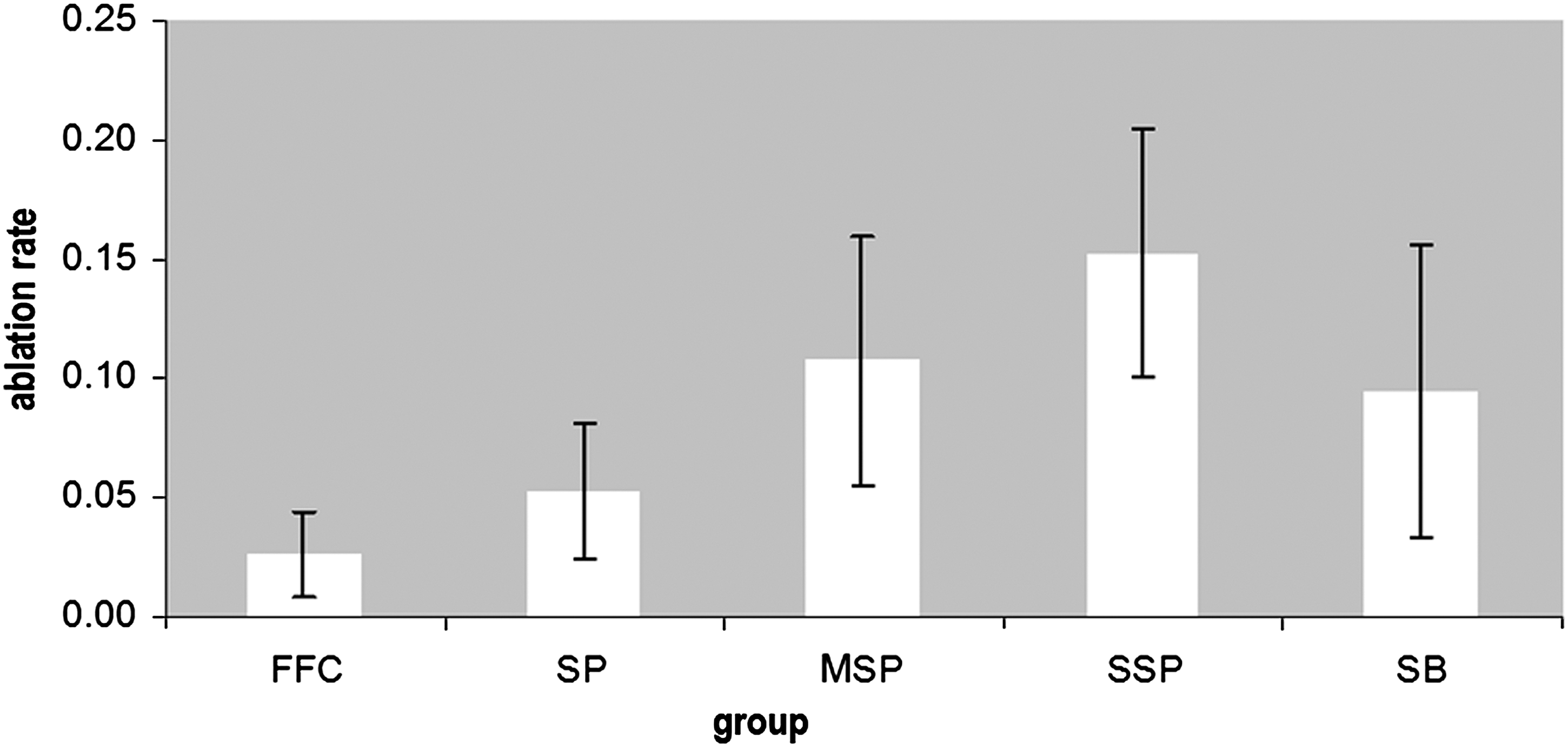
Clinical ablation rate (in mm3/sec) of caries in dentin in the FFC, SP, MSP, SSP, and SB groups. The SSP group is statistically significantly different in comparison with the MSP and SB groups (p<0.05). The MSP and SB groups are statistically significantly different in comparison with the SP and FFC groups (p<0.05).
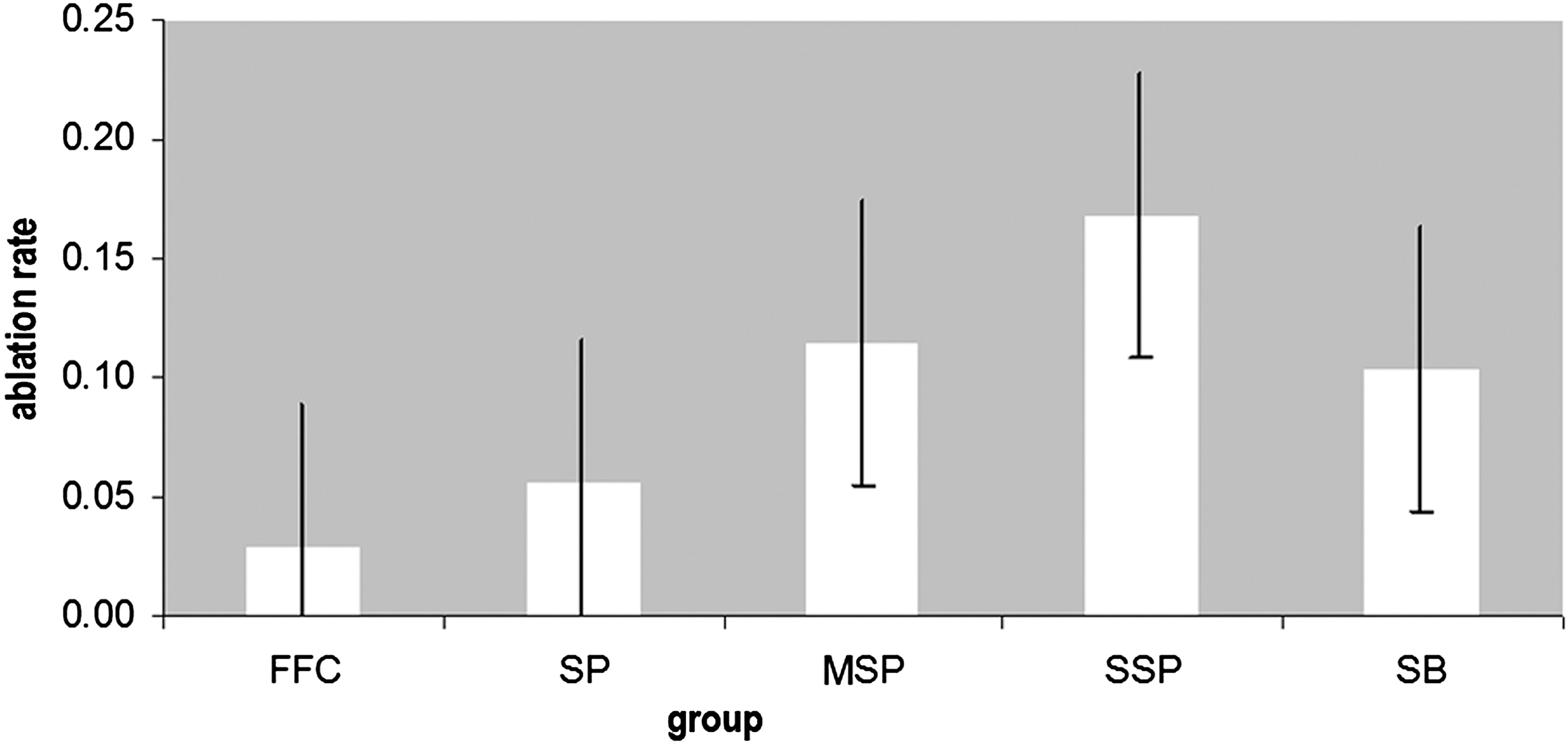
The real ablation rate (in mm3/sec) of caries in dentin in the FFC, SP, MSP, SSP, and SB groups. The SSP group is statistically significantly different in comparison with the MSP and SB groups (p<0.05). The MSP and SB group are statistically significantly different in comparison with the SP and FFC groups (p<0.05).
SEM observation of dentin surfaces
The SB and FFC groups revealed a dentin surface with a smear layer and closed dentinal tubules (Figs. 5 and 6).
SEM (original magnification ×2000) showing dentin surface after caries removal in the SB group. A smear layer and closed dentinal tubules are visible on the dentin surface.

SEM (original magnification ×2000) showing dentin surface after caries removal in the FFC group. A smear layer and closed dentinal tubules are present.
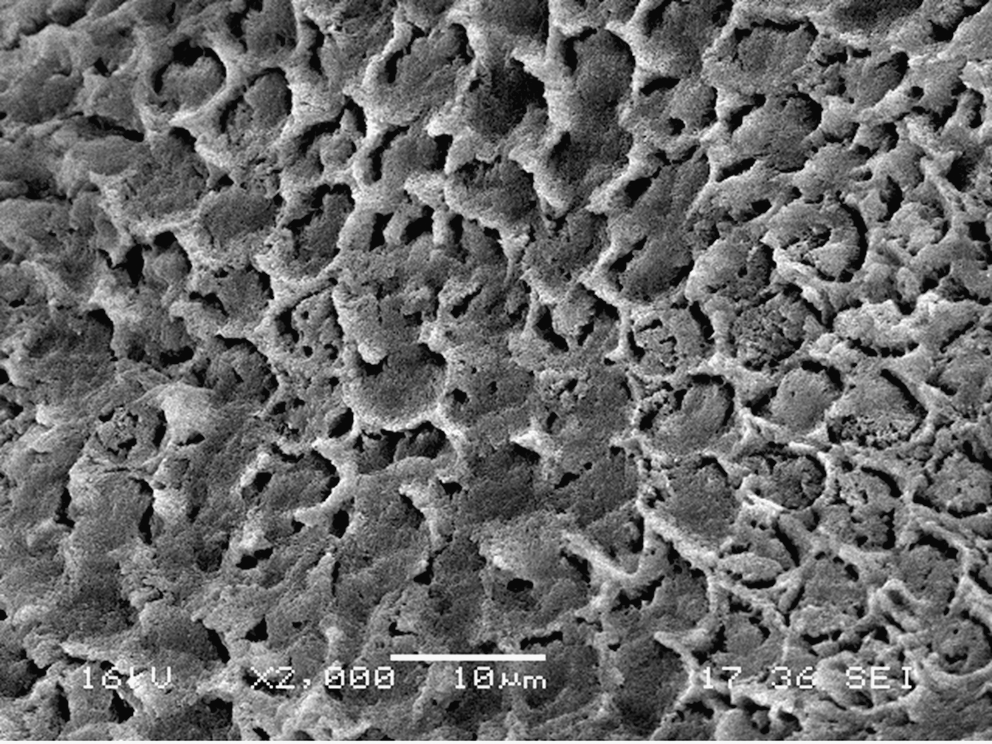
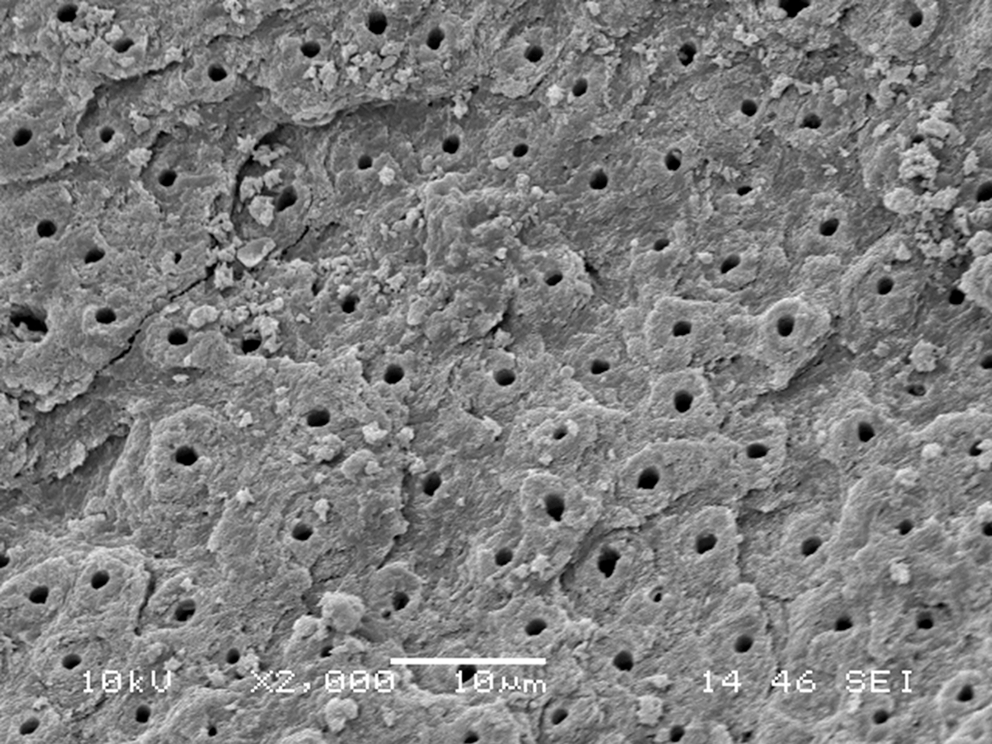
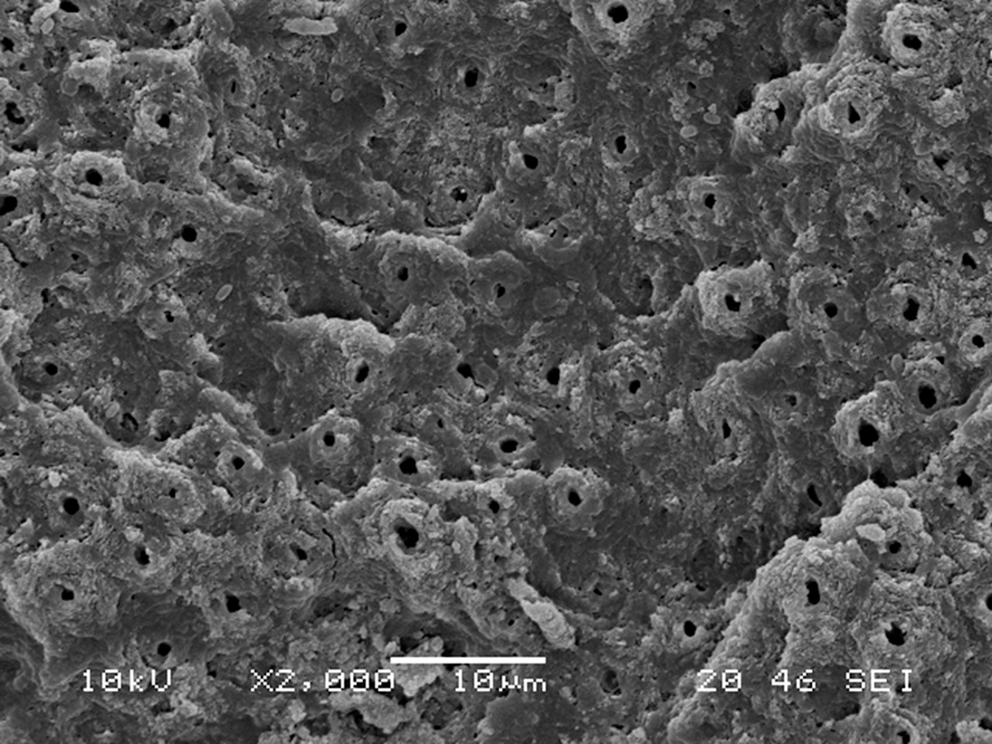
In the SSP, MSP, and SP groups, irregular, crater-like surfaces were observed (Figs. 7 –9). Dentin surfaces were clean of the smear layer, especially in the SSP group, exposing the orifices of the dentinal tubules (Figs. 7 –9). Intertubular dentin was selectivly ablated more than the peritubular dentin, making the tubules protrude (Figs. 7 –9).
SEM (original magnification ×2000) showing dentin surface after caries removal in the SSP group. Dentin surface is irregular, clean, and with open dentinal tubules.
SEM (original magnification ×2000) showing dentin surface after caries removal in the MSP group. Surface is irregular and clean of smear layer, and the dentinal tubules are opened.
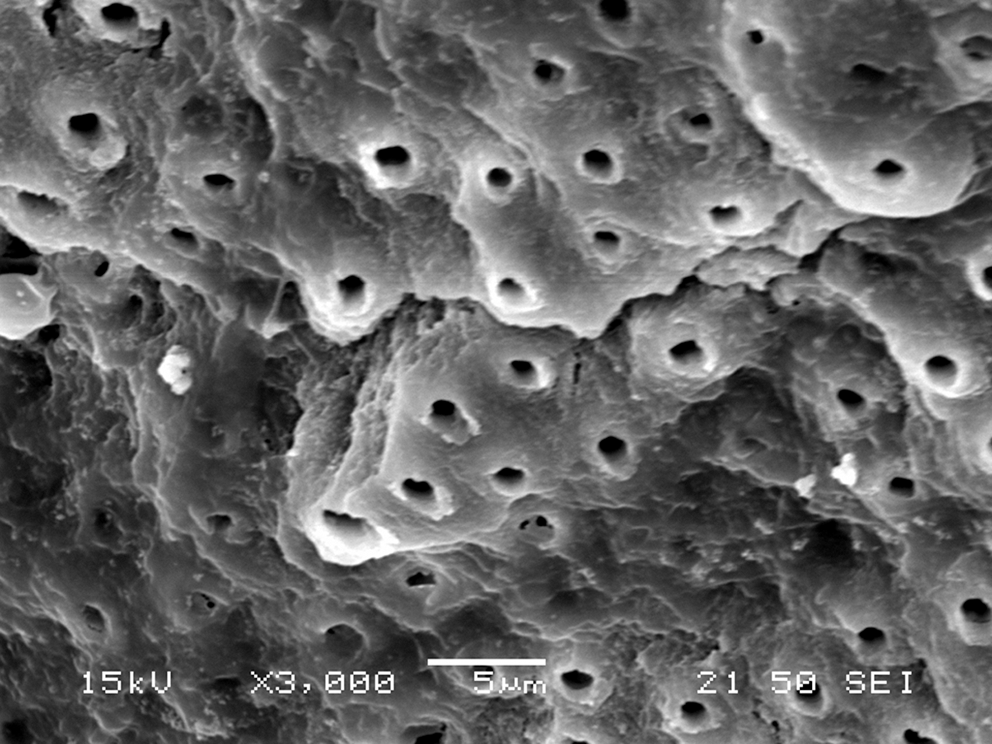
SEM (original magnification ×3000) showing an irregular and clean dentin surface with open dentinal tubules after caries removal in the SP group.
Discussion
The ablation rate of hard dental tissue has been measured using different techniques: determination of the crater depth in tooth sections with an ocular micrometer of a microscope, 21 measuring the time needed for the complete perforation of a dental sample of a known thickness, 22 cavity diameter and depth measurements for further evaluation of the cavity volume, 15,23 optical coherence tomography, 24 3D X-ray microtomography, 25 measurement of the difference in the mass of the specimen before and after irradiation, 26 SEM-based techniques, or 3D laser scanning. 27,28 These methods have disadvantages such as inaccuracy, lengthiness, and complexity, or non-repeatability because of the destruction of the sample. In the present study, a method based on the optical triangulation principle has been used to determine the volume and calculate the ablation rate of the Er:YAG lasers and the steel bur in caries in dentin. Laser profilometry has advantages of being highly accurate with error in volume determination <5%, which was checked by comparing the results obtained through optical microscopy and mechanical stylus measurement. 29 Moreover, the repeatability of volume measurement was found to be >1.8%. 29 It is also interesting to note that this method is not time consuming. It takes just over a minute on average to prepare the sample, scan the surface, generate the 3D model, and determine the volume, without destruction of the sample. 29,30
Although in previously published studies a lower ablation rate of Er:YAG lasers for caries removal was found, 4,30 –32 results of the present study showed that Er:YAG laser working with SSP was the most efficient in caries removal. VSPt and short pulse duration can explain the higher real and clinical ablation rate of SSP in comparison with longer pulses of Er:YAG laser, FFC, and steel bur. The Er:YAG laser based on a new technology enables selection of short pulse durations, which allow the speed of ablation to be faster than the diffusion of heat into the tissue, and then all of the laser energy is used for hard dental tissue ablation. 19 This effect is less pronounced for longer pulses, when ablation efficiency is reduced because of the thermal effects. 19 Furthermore, the pulse shape in VSPt should also be considered, as it has strong influence on the pulse width and power. 30 The pulse profile is controlled and allows the power within the pulse to remain approximately constant. 30 This ensures that the pulse modality does not uncontrollably shift during a pulse from cold to warm and hot ablation, reducing the ablation and increasing the heating of hard dental tisssue. 30 Furthermore, higher water content and permeability of caries in dentin further facilitate the caries removal using the Er:YAG laser whose energy is apsorbed in water. 33 In the present study, SP and FFC were the groups with the longest pulse durations; 300 and 400 μs. When longer pulses are used, the efficiency in hard dental tissue removal is reduced because of conductive loss of pulse energy in the form of heat, 34 leaving less energy for the removal of dentin or enamel. Also, the absorption and scattering of a laser beam in tissue, which has been removed in microexplosions during laser irradiation, influence the ablation rate and the optical quality of the laser beam. 19 The measurement of the He-Ne laser tranmission through the “cloud” made of particles of tissue removed by different pulses of the Er:YAG laser 2 mm above the tooth surface, has shown that the biggest “cloud” is formed when longer pulses are used. 34 This lowers the ablation rate of hard dental tissue 19 as in the SP and FFC group in the present study.
The SEM observation of dentin after caries removal with the VSPt-based Er:YAG laser showed an irregular surface, free of the smear layer, and with open dentinal tubules. Protruded dentinal tubules on SEM micrographs indicate that the intertubular dentin was less resistant to laser action than peritubular dentin, which can be explained by the greater amount of water and collagen and lower mineral content in the intertubular dentin. 35 Similar results were found in other SEM studies. 36 –38 In addition, thermal changes such as melting or carbonization of the dentin surface after caries removal were not observed. Camerlingo et al. 37 showed with micro-Raman spectroscopy that after laser irradiation of dentin, different forms of β-tricalcium phosphate, which appear when crystals of hydroxyapatite are heated on high temperatures, are not found, 39 which can explain the lack of thermal changes on the dentin surface. The cleanest dentin surface was found in the SSP group because of the higher efficiency of shorter pulses in hard dental tissue ablation, 30 and therefore in the ablation of the smear layer, which consists of water and inorganic and organic parts, in which the energy of Er:YAG laser is absorbed. Husein 40 found open dentinal tubules and no smear layer after the Er:YAG laser irradiation with different combinations of energy, frequency, and pulse length, and the cleanest surface was found when shorter pulses were used, similar to the results of the present study. After the caries removal with the steel bur, the dentin surface was covered with a smear layer, and the dentinal tubules were closed, which is consistent with the findings of Camerlingo et al. 37 and Comte. 41 In the FFC group, the SEM observation showed a dentin surface similar to the SB group, with a smear layer and closed dentinal tubules. Although in the FFC group the Er:YAG laser was used, this laser is not based on VSPt and is less effective in dentin and smear layer removal, which was confirmed in the present study. The pulse shape in VSPt enables constant energy of laser beam during pulse duration and all the energy is used for tissue ablation, 30 increasing the ablation rate of hard dental tissues and the removal of the smear layer. Although SSP was the most efficient in caries tissue removal, leaving the dentin surface clean of a smear layer and with open dentinal tubules, further studies should examine the effect of different pulses of the Er:YAG laser and the lack of the smear layer on adhesion properties of different adhesive systems to dental hard tissues.
Conclusions
Taking into consideration the experimental conditions of the present study, SSP was the most efficient in ablation of caries in dentin, providing a smear layer-free surface with open dentinal tubules.
Footnotes
Acknowledgments
This study was performed and financed within the research project “Experimental and Clinical Endodontology” No. 065-0650444-0418, approved by the Ministry of Science and Technology of the Republic of Croatia.
Author Disclosure Statement
No competing financial interests exist.