
Abstract
Introduction
For many years, periodontal therapy was traditionally performed by hand instruments, and numerous studies have reported beneficial outcomes from this treatment modality in both clinical and microbiological studies. 3,4 However, there are limitations to manual instrumentation because of the need for operator skills, and the complex anatomy of root surfaces, particularly in deep pockets. 5 Ultrasonic scalers were first designed for gross supragingival scaling and removal of stains, but recently, by modification of the diameter and length of the tips, they have become a routine part of scaling and root planning (SRP) procedure. 6,7 Studies investigating the removal of endotoxins have revealed that endotoxins are superficially attached to the cementum and can almost be completely removed by gentle scaling with hand instruments or ultrasonic scalers. 8,9 Evidence suggests that SRP with either hand instruments or ultrasonic scalers has similar clinical and microbiological outcomes. 10,11 In addition to that, studies indicate that ultrasonic instrumentation takes less time to achieve the same clinical results. 7,8 However, production of pathogenic bacterial aerosol formation is an important concern for clinicians, unless necessary precautions are taken. 12
More recently, parallel to the technological development in medicine, lasers have been proposed for use in periodontal therapy. Unlike neodymium-doped: yttrium, aluminium and garnet and diode lasers, erbium-doped: yttrium, aluminium and garnet (Er:YAG) lasers are well absorbed in water so that they can ablate hard tissues without causing any major thermal side effects. 13 Because periodontal tissues consist of both hard and soft tissues, Er:YAG lasers are the most promising lasers for periodontal therapy. In vivo and in vitro studies have shown that Er:YAG lasers are able to remove calculus and that furthermore, lasers seem to have a bactericidal potential and endotoxin removal effect on diseased root surfaces; however, there are conflicting results concerning the efficacy of calculus removal. 14 –17 Histological and scanning electron microscopic (SEM) studies have shown that Er:YAG lasers ablate not only the calculus, but also the superficial layer of cementum, leaving a “microstructured” root surface, and that its functions are not fully understood yet. 18,19 Although most of the clinical studies revealed beneficial results of Er:YAG lasers, it is not clear if they have any additional benefits to hand instruments or ultrasonic scalers. 20 –24 The aim of this randomized, controlled clinical study is to compare the efficacy of SRP with hand instruments, ultrasonic scalers, or Er:YAG lasers alone for the treatment of moderately deep and deep pockets, through the use of clinical parameters and micro-organism and leukocyte counts by phase-contrast microscope.
Material and Methods
This study was designed as a randomized, single blind, prospective controlled clinical trial. All the patients were recruited from Clinic of Periodontology, Department of Marmara University Dentistry Faculty, between October 2008 and January 2010. The Ethical Committee of Marmara University, Turkey, evaluated the study protocol and approved it in 2007 (Protocol: MAR-YC-2007-0184). All participating patients signed the informed consent at the beginning of the study.
Study population
Thirty patients (11 women and 19 men), between 41 and 67 years of age (mean age 48.83±7.23) with chronic periodontitis 25 participated in this clinical study. Patients with generalized periodontal breakdown and who had at least four single-rooted teeth, two moderately deep (probing depth [PD] of 4–6 mm) and two deep pockets (PD≥7 mm) that had no endodontic lesion and no crown, with mobility 0–2, and with bleeding on probing (BOP) were selected. Exclusion criteria were as follows: periodontal treatment within the last 6 months, any systemic disease that would influence the periodontal tissues, antibiotic use within last 6 months, pregnancy, and smoking.
Study design
Patients were randomly assigned to three study groups (n=10) as: hand curettes (Group H), ultrasonic scalers (Group U), and Er:YAG lasers (Group L). At the first appointment, alginate molds of the dental arches were made to prepare stents for standardized probing, full-mouth radiographs were taken, and all the patients received oral hygiene instructions. Four single-rooted teeth with radiographic bone loss (two sites PD 4–6 mm, two sites PD≥7 mm) that met the inclusion criteria were probed and assigned for subgingival sampling. One week later, subgingival samples were collected and evaluated (T.K.) from 4 preselected teeth from each patient and full mouth clinical measurements were done (U.N.).
Treatment procedures
After the recordings were taken, all patients had supragingival scaling by ultrasonic scalers, and patients of all experimental groups received debridement of whole dentition by the same operator (E.M.) up to four to six sessions by weekly intervals (30–45 min sessions).
For the treatment of Group H, an assortment of manual periodontal curettes (Gracey, SG # 5/6, 7/8, 11/12, 13/14, Mini Five Gracey SAS # 5/6, 11/12, Hu-Friedy Ins. Co., USA) were used. The curettes were sharpened at the operator's request. For Group U, a magnetostrictive ultrasonic scaler (Cavitron® Bobcat Pro®, Dentsply International Inc, USA) with metal tips (Cavitron® Insert 25K TFI-1000, FSI Slimline Left, FSI Slimline Right, Dentsply International Inc, USA) was used under water irrigation according to manufacturer's instructions. For the treatment of Group L, Er:YAG laser treatment was applied at an energy level of 160 mJ/pulse and a repetition rate of 10 Hz with water irrigation (AT Fidelis, FOTONA, Slovenia). Chisel type fiber tips (1.5×0.5 mm) (R14C Handpiece, Chiseled Tip) were used with a coronal to apical way in parallel paths with an inclination of 15–20 degrees to the root surface. For all groups, SRP was finished when the surface was felt to be smooth by a supervisor (U.N.). Local anesthesia was used in all three groups according to the patients' needs.
After the active therapy was completed, all patients were included in a maintenance program composed of reinforcement of oral hygiene instructions on days 30 and 60.
Clinical parameters
The baseline data were recorded before treatment and 90 days after the treatment. Plaque index (PI), 26 gingival index (GI), 27 and PD were measured from the gingival margin to the bottom of the pocket, and relative attachment level (RAL) was measured from the margin of the stent to the bottom of the pocket by a calibrated researcher (U.N.). BOP was assessed 30 sec after probing, as presence (+) or absence (-) of bleeding. PI and GI measurements were made at four aspects (mesial, distal, vestibular, and oral) and BOP, PD, and RAL measurement were made at six aspects (mesiovestibular, midvestibular, distovestibular, disto-oral, mid-oral and mesio-oral) of the tooth using a manual periodontal probe (University of North Carolina PCPUNC15, Hu-Friedy Ins. Co., USA). PDs were grouped as 4–6 and ≥7mm.
Subgingival sampling
Subgingival samples were collected at baseline and 7 and 90 days after treatment from two moderately deep and two deep pockets. After the supragingival plaque was removed and the area was isolated with a cotton roll, the subgingival samples were collected with a sterile curette. The samples were immediately placed in 0.2 mL phosphate buffered saline solution (phosphate-buffered saline, PBS tablets, Medicago AB, Uppsala, Sweden) and were homogenized with a gauge needle. Within 15 min, one drop of plaque suspension was applied to a microscopic slide and cover-slipped, and the collected samples were evaluated with a phase-contrast microscopy (Olympus CH-2 light microscopy, Japan) (T.K.). Crevicular leukocyte levels were scored quantitatively at ×400 magnification in at least five fields that contained the greatest concentrations of accumulated leukocytes as described by Rams et. al. 28 From the same plaque suspension, a new specimen was prepared and the samples were evaluated following the procedures of Listgarten and Shifter. 29 The first 100–200 microbial cells that were encountered in randomly selected microscopic fields under a ×1000 magnification were classified into the morphologic categories: spirochetes, motile rods, rods, and cocci.
Statistical analysis
Data collected in this study were statistically analyzed by NCSS software program (Number Cruncher Statistical System 2007&PASS 2008 Statistical Software Utah, USA). All clinical data were normally distributed. and to analyze the relation among groups, one-way ANOVA among time periods paired sample t tests were used. For non-normally distributed laboratory data, Mann–Whitney U test was used to compare between two groups when Kruskall–Wallis test presented a significant difference (p<0.05). Between time periods, non-normally distributed data were first tested by Friedman test, and if significance was observed, Wilcoxon sign tests were used for further evaluation.
Results
Clinical measurements
During the treatment period, two patients in Group L had developed periodontal abscesses. Pocket depth of the teeth with periodontal abscesses was>11 mm and because they were not sampling teeth, the patients were not excluded from the study. At the baseline, PI was 2.06±0.29, 1.76±0.25, and 1.92±0.35 for Group H, Group U, and Group L, respectively. Ninety-day examination showed that the scores were significantly reduced to 0.25±0.05, 0.22±0.07, and 0.23±0.04 (p<0.01), respectively). The GI scores of 1.97±0.21, 1.85±0.26, and 1.86±0.19 found during the baseline examination were significantly reduced to 0.23±0.07, 0.25±0.16, and 0.22±0.09 for Group H, Group U, and Group L, respectively (p<0.01). The BOP scores for Group H, Group U, and Group L were %87.10±8.73, %81.20±15.91, and %83.20±14.77 at the baseline examination and significantly reduced to %15.20±2.90, %13.50±2.89, and %15.50±2.59, respectively, at the 90-day examination (p<0.01). For the PI, GI, and BOP scores no statistically significant differences were observed among groups (p>0.05).
From baseline to 90 days, a significant reduction in PD and a significant attachment gain were observed for the three study groups (p<0.01). There were no statistically significant differences among methods of instrumentation (Table 1).
Subgingival evaluation
Measurements made 7 and 90 days after the treatment show that all three treatments led to significant reduction in spirochete, motile rods, and leukocyte counts, and significant increase in nonmotile rods and cocci counts at 7 and 90 days after treatment (p<0.01). From day 7 to day 90, observed changes varied according to treatment groups and PD intervals. From day 7 to day 90, motile organisms had significantly elevated in Group U (p<0.05) in moderately deep pockets and, in Group U (p<0.01) and Group L (p<0.05), in deep pockets. For the spirochetes, whereas the increase in Group H (p<0.05) was significant in moderately deep and deep pockets, both Group U (p<0.01) and Group L (p<0.05) showed significant increases. From day 7 to day 90, the decrease in the nonmotile rod ratios was only significant in Group L (p<0.01) in deep pockets, and no significant changes were observed in the cocci ratios (p>0.05). The noted elevation of leukocyte counts was significant in Group U (p<0.05) in moderately deep pockets and, in Group U (p<0.05) and Group L (p<0.01), in deep pockets (Figs. 1 –5).
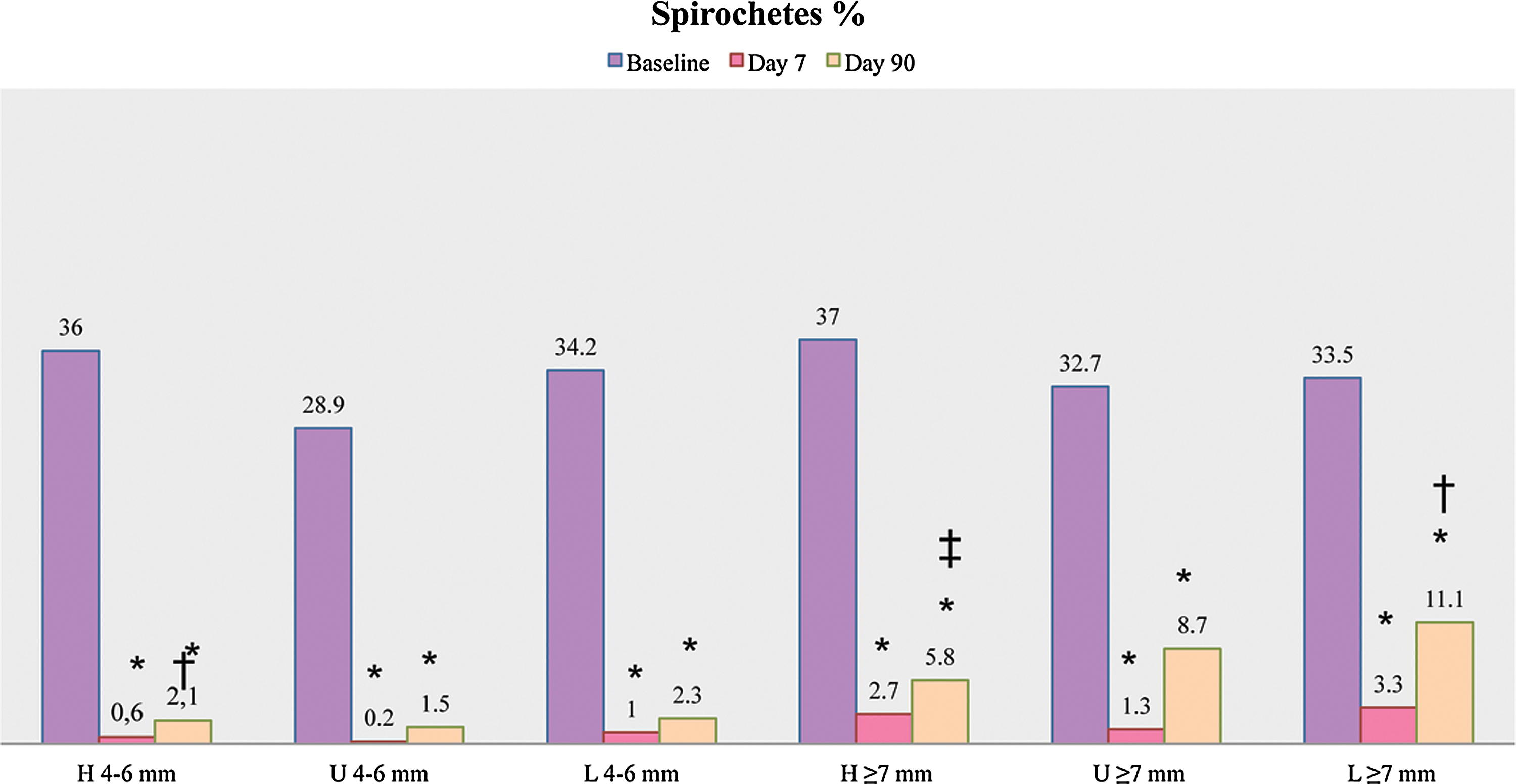
Spirochetes ratios in all groups and intragroup statistics. *Statistically significant from baseline (p<0.01), †statistically significant from day 7 (p<0.05), ‡statistically significant from day 7 (p<0.01).
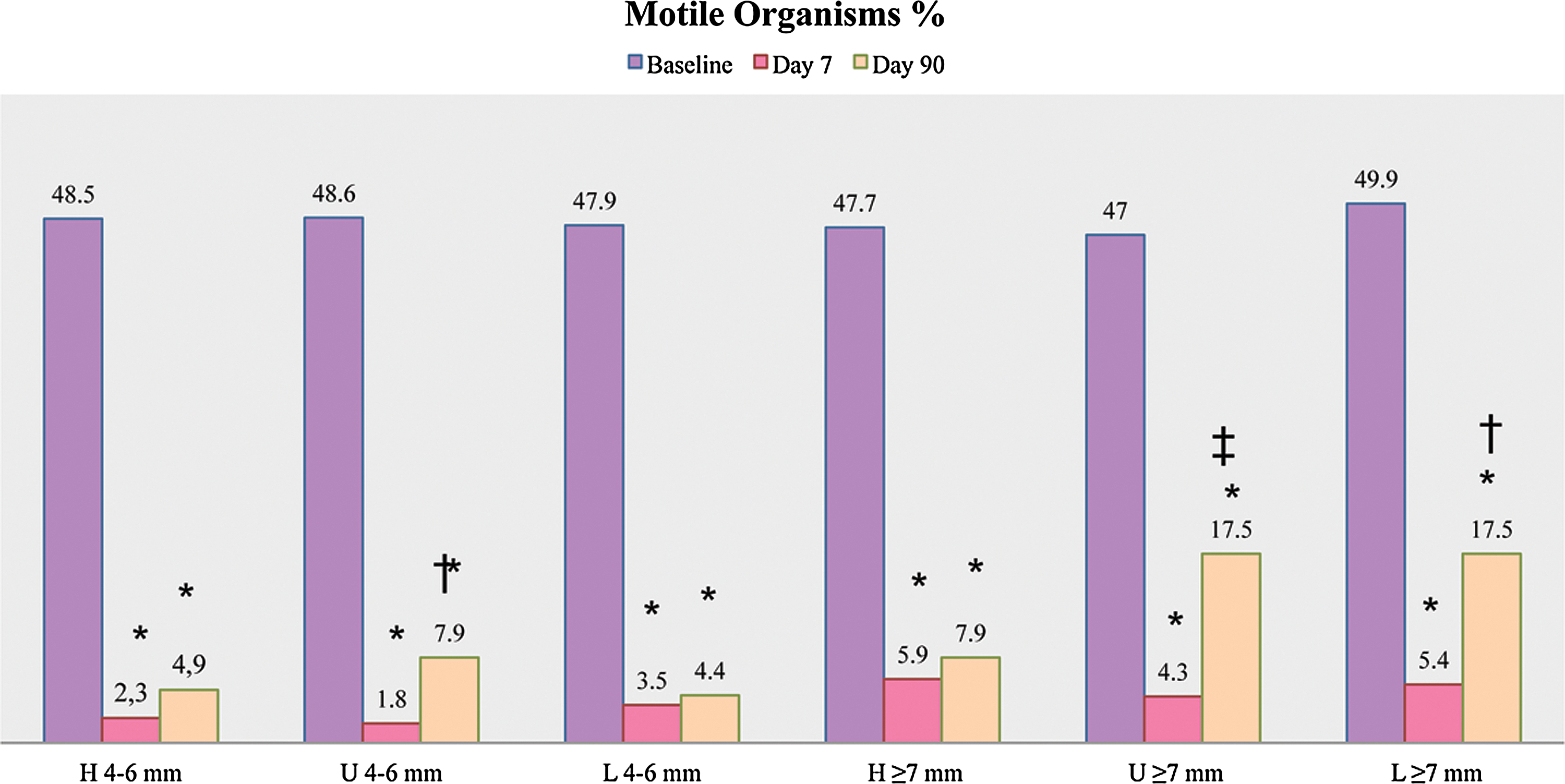
Motile organism ratios in all groups and intrgroup statistics. *Statistically significant from baseline (p<0.01), †statistically significant from day 7 (p<0.05), ‡statistically significant from day 7 (p<0.01).
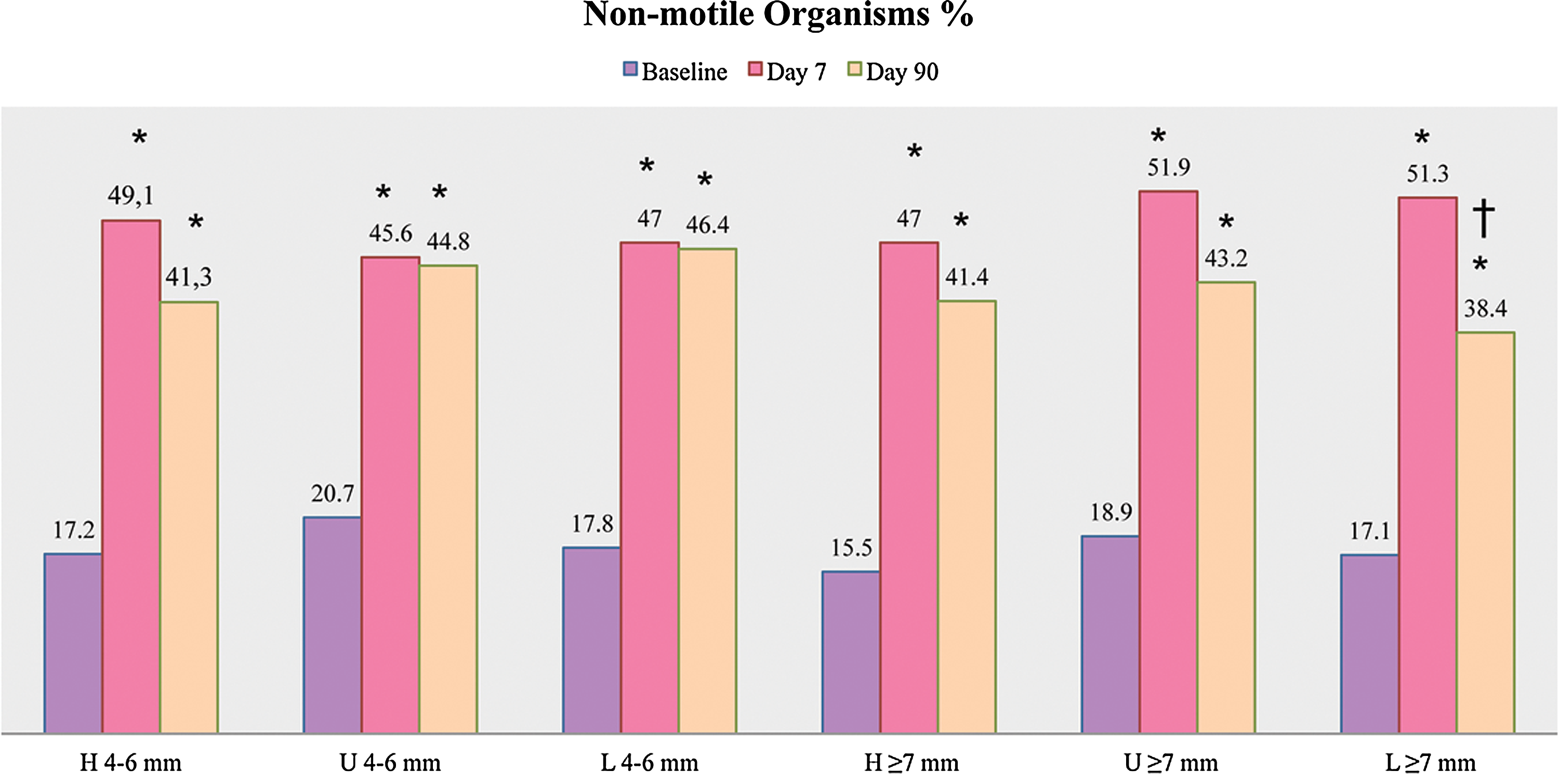
Nonmotile organism ratios in all groups and intrgroup statistics. *Statistically significant from baseline (p<0.01), †statistically significant from day 7 (p<0.01).
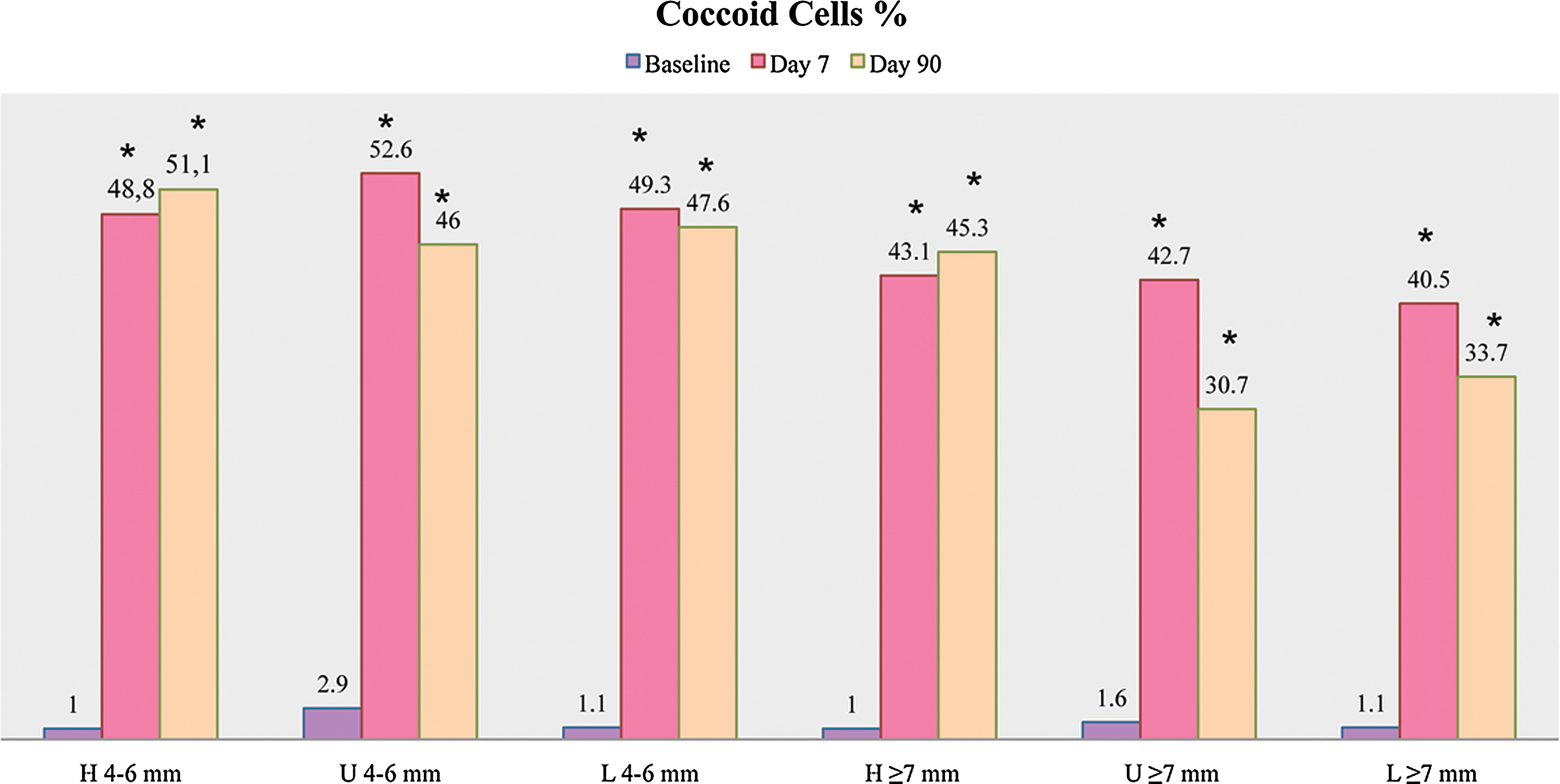
Coccoid cell ratios in all groups and intrgroup statistics. *Statistically significant from baseline (p<0.01).
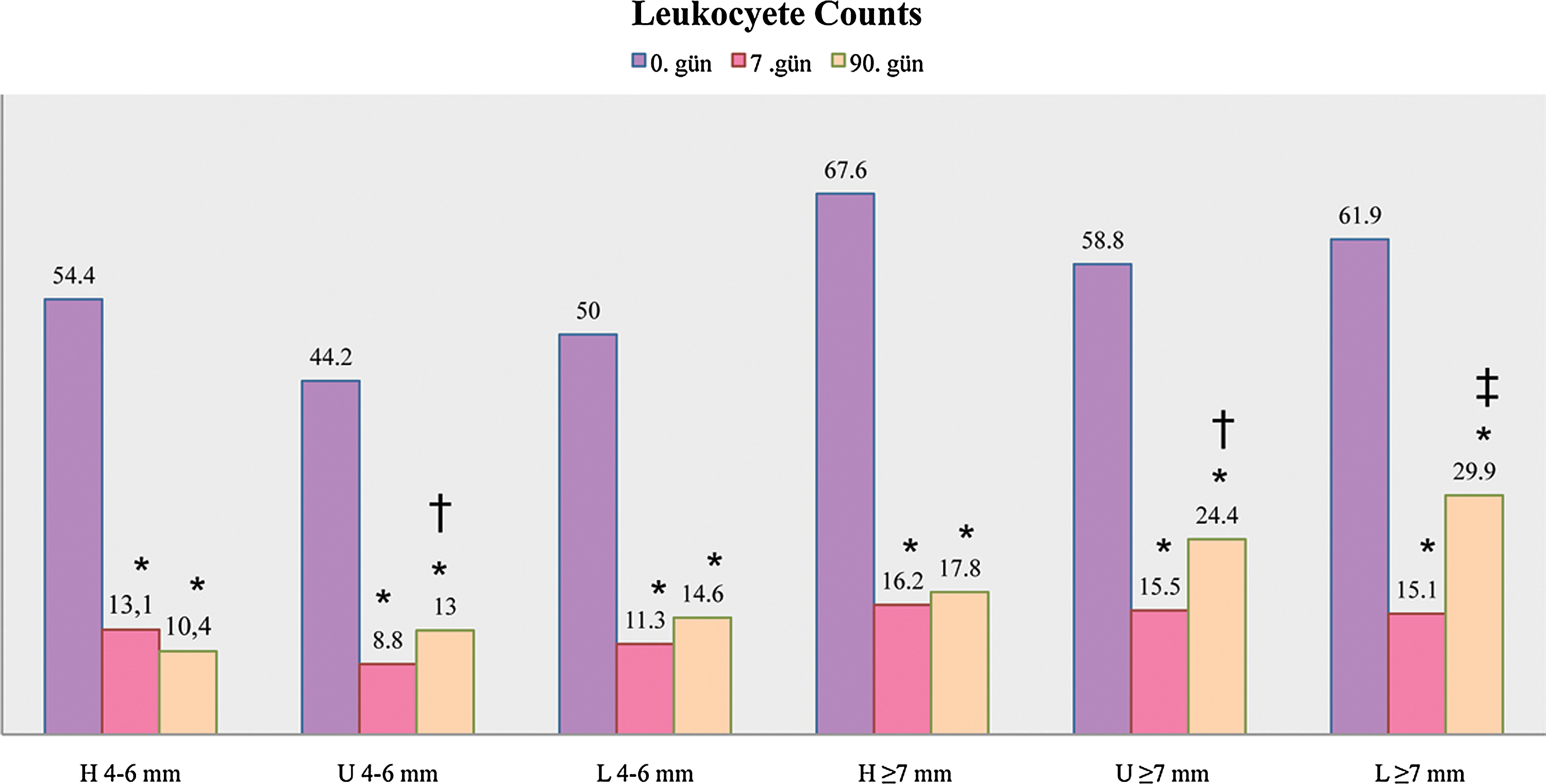
Leukocyte counts in all groups and intrgroup statistics. *Statistically significant from baseline (p<0.01), †statistically significant from day 7 (p<0.05), ‡statistically significant from day 7 (p<0.01).
There were statistically significant differences when the microorganism and leukocyte changes from day 0 to day 90 and from day 7 to day 90 were evaluated among groups (Table 2). According to the statistical analysis, the increase of motile organisms from day 7 to day 90 in Group H was significantly lower than the increase in Group U (p<0.05) in deep pockets. The increase of cocci ratios from day 0 to day 90 was significantly higher in Group H than in Group U and Group L (p<0.05) in deep pockets. In Group H, whereas the leukocyte counts still decreased, the counts leaned toward increase in Group U and Group L, and the changes in Groups U and L were significantly higher than in Group H (p<0.05) in moderately deep pockets. In deep pockets, changes in Group H were significantly lower than in Group L (p<0.05).
Statistically significantly different from Group U (p<0.05).
Statistically significantly different from Groups U and L (p<0.05).
Statistically significantly different from Group L (p<0.05).
Discussion
The results of the present study indicate that nonsurgical periodontal therapy by hand instruments, ultrasonic scalers, or Er:YAG laser may lead to statistically significant improvements in all clinical parameters 90 days after the treatment was applied. These results are in accordance with the previous studies evaluating the effect of nonsurgical periodontal therapy in the treatment of chronic periodontitis. 2 –4,10,30 The comparison of hand instruments to ultrasonic scalers has revealed that use of both resulted in similar clinically and microbiologically successful outcomes; however, there are certain limitations such as the depth of the pocket and the anatomic structure of the roots. 31 Regarding the contribution of variable lasers to dentistry, Er:YAG laser has been the focus of periodontal therapy because of the high absorption in water caused by its wavelength. However, there are conflicting results considering the adjunctive benefits of Er:YAG laser use in periodontal therapy over hand instruments or ultrasonic scalers. 20,23,32 Our study aimed to compare the effectiveness of Er:YAG laser with two formerly successful instruments, hand instruments and ultrasonic scalers, and to determine the subgingival cell population changes in moderately deep and deep pockets, separately.
Both microbiological results and leukocyte counts significantly improved 7 and 90 days following therapy compared with baseline. But when the 7–90 day changes were evaluated, a slight increase in spirochetes, motile rods, and leukocytes and a decrease in nonmotile rods and cocci were observed. These changes were markedly higher in deeper pockets and hand instruments were significantly more successful then ultrasonic scalers and Er:YAG laser in maintaining the 7 day results. The PD reduction and attachment gain was also higher in deep pockets, and this is in accordance with previous studies. 10,20
The fact that there was no statistically significant difference in PI, GI, and BOP scores among groups indicates that, with nonsurgical periodontal treatment and personal oral hygiene procedures, decrease in vascular permeability and reconstruction of epithelial and connective tissue elements lead to resolution of the inflammation, independent of the treatment modality. 21,23,33
In the search to investigate the effect of Er:YAG lasers in nonsurgical periodontal therapy, there are conflicting results concerning the PD and attachment gain levels. In two clinical studies by Schwarz et al. 22,34 comparing Er:YAG laser (160 mJ/pulse, 10 Hz) with hand instruments, and in another study by Crespi et al. 20 comparing Er:YAG laser with ultrasonic scalers, it was reported that Er:YAG laser groups revealed significantly higher PD reduction and CAL gain 3 and 6 months and 1 and 2 years after therapy. Writers associated these results with atraumatic use of the laser handpiece. Similarly, Tomasi et al. 24 compared the effectiveness of ultrasonic scalers and Er:YAG laser. Although there were significant PD reduction and attachment gain in favor of the laser group on the 1 month examination, 4 months after therapy there were no significant difference among groups. In other clinical studies, Sculean et al. 23 evaluated the effect of ultrasonic scalers and Er:YAG lasers alone and Schwarz et al. 21 evaluated Er:YAG laser alone and SRP plus Er:YAG laser in periodontal therapy, and in both studies no significant difference were found between two groups for the PD reduction and clinical attachment gain. Although there is no agreement to what extent the hand instruments, ultrasonic scalers, and Er:YAG lasers have advantages or disadvantages over one another, all three treatment modalities have been significantly successful because of adequate SRP of the root surfaces and bacterial deposit removal. Likewise, in our study, all the treatments were clinically effective without any statistically significant difference among groups.
As the results of the subgingival samples of this study were evaluated, 7 and 90 days after therapy spirochetes, motile rods and crevicular leukocyte counts had statistically significantly decreased whereas nonmotile organisms and cocci ratios had significantly increased. However, considering the 7- to 90-day changes, the results were significantly different among groups and most of the significant results were detected in deep pockets. Spirochete and motile rod ratios had significantly increased from 7 to 90 days after treatment in Groups U and L. In addition, from 7 to 90 days after treatment, cocci ratio continued to increase in Group H whereas it decreased in Groups U and L. According to these results, ultrasonic scalers and Er:YAG lasers seem to fail to maintain the 7th day results compared with hand instruments. This could be related to increased bacterial retention in rough surfaces. Studies indicate that hand instruments sustain a smoother surface than do ultrasonic scalers and lasers, 35 which may be related to slower recolonization. 36 It has also been shown that the rough surface after laser application is suitable for fibroblast attachment in vitro, 37 but in in vivo conditions, this surface may also accelerate the bacterial colonization rate. There are still controversies about the role of “microstructured surface” of laser-treated root surfaces. Some studies suggests that it must be removed by SRP, although no clinical differences were observed by the use of Er:YAG lasers in combination with hand curettes or used alone in periodontal therapy. 21,32 However, the results of the present study indicate a faster recolonization in rough surfaces, and this may affect the long-term clinical results.
Periodontal pockets contain higher amounts of leukocytes compared with the healthy sulcus. 38,39 This may be the result of the constant activation of the immune system in chronic inflammation. 40 There are studies evaluating the leukocyte counts before and after treatment with an intrasulcular washing system. According to Claffey et. al. 41 the numbers of leukocytes tend to reduce after therapy. Likewise, Boretti et al. 39 compared the effectiveness of hand instruments and ultrasonic scalers with the washing technique, and reported that both the number and the vitality of the leukocytes decreased after treatment. One other finding of Boretti et. al. 39 was that, particularly in the 50 μL suspension group, hand instruments reduced leukocyte numbers significantly more than did the ultrasonic scalers. In the present study, we found, similarly to Boretti et al., that hand instruments were statistically significantly more successful in maintaining the 7 day results compared with both ultrasonic scalers and Er:YAG lasers.
Conclusions
Within the limitations of this study, it was found that although Er:YAG lasers are clinically as efficient as hand instruments and ultrasonic scalers in treating periodontal disease, they do not seem to be notably superior to conventional systems. However, it is known that all these systems have advantages and disadvantages of their own, and therefore, for better results, the speed of ultrasonic scalers, more efficient de-epithelization of Er:YAG lasers, and smooth root surface of hand instruments, should be combined, through using the three systems together.
Footnotes
Acknowledgments
This clinical study was supported by the project numbered SAG-DRP-120309-0048 of Marmara University Scientific Research Projects Department.
Author Disclosure Statement
No competing financial interests exist.