
Abstract
Introduction
Few clinical studies have compared ERL to mechanical treatment (ultrasonic or manual). The results of those that have are controversial, showing no or little superiority on the part of ERL. A recent meta-analysis concluded that future clinical trials are needed to assess the efficacy of Er:YAG lasers in the nonsurgical treatment of chronic periodontitis. 12
This report describes a split-mouth design, randomized controlled pilot study that used clinical periodontal parameters and procedure comfort to compare ERL to mechanical SRP.
Methods
Study sample
The difference in clinical attachment level between the two treatment modalities was expected to be 1 mm±1 (α=5%).
Twenty-three subjects (12 men and 11 women, mean age: 60.7) with chronic generalized periodontitis were selected for inclusion. Patient recruitment and treatment were conducted at the periodontology unit of the university hospital of Nantes (CHU), France. During the study, four patients were excluded (n=19) for not attending reevaluations.
Inclusion criteria
Inclusion criteria were: • Being an adult (≥18 years of age) diagnosed with chronic periodontitis • Having at least four sites with PPD ≥4 mm in each quadrant • Being enrolled in an oral hygiene program (that included professional prophylaxis and daily oral care instructions) • Having the mental ability to express informed consent
Exclusion criteria
Exclusion criteria were: • Systemic conditions that could affect periodontal treatment output (e.g., diabetes, immunosuppression) • Pregnancy • Antibiotic use in the 6 months preceding recruitment • Tobacco use
Informed consent
All subjects received written information about the study and expressed their informed consent, in accordance with guidelines issued by the Patient Protection Committee at the Nantes CHU (SC 07/9-N).
Clinical parameters
Clinical parameters evaluated were • PPD at six sites/teeth • Gingival recession (GR) at six sites/teeth • CAL at six sites/teeth
A computerized periodontal probe, with a constant pressure of 17g (Florida Probe®, FL), was used to assess PPD and gingival recession and to calculate CAL. BOP was evaluated (six sites/teeth) by noting the presence/absence of bleeding 30 sec after pocket probing. Clinical examinations were performed at baseline (D0) and repeated at reevaluation visits, 2 months after the first treatment sessions (D60).
The mean score for all sites receiving the same procedure was calculated for each parameter.
Operators
The same examiner, who was different from the operator, was responsible for the blinded measurement of all clinical parameters at D0 and D60.
Clinical treatment
Randomization of patient assignment was ensured by placing treatment procedures in sealed envelopes for the first quadrant. At the beginning of the first treatment visit, each operator opened a sealed envelope and discovered the treatment modality and the first quadrant to be treated. The following quadrant received a different treatment and was chosen by moving in a clockwise direction on a map of the mouth:
right/maxillary〉left/maxillary〉left/mandibular〉right/mandibular
SRP was performed with a set of Gracey curettes (5/6, 11/12, and 13/14; Hu-Friedy, Chicago, IL) and with locally injected anesthetic (Primacaine Adrenaline 1/200000™, Acteon, Merignac, France). The treatment end point was determined by the operator, using a probe.
ERL was performed with an Er:YAG laser device that had a wavelength of 2940 nm (Laser Key 3, Kavo, Biberach, Germany; hand piece 2061), combined with an automatic calculus detection system. 11 The latter detected the fluorescent properties of calculus when calculus was excited with an InGaAsP laser beam of 655 nm. An Er:YAG laser beam was automatically emitted via water irrigation when the system detected calculus fluorescence (feedback threshold of 5 [U]). A special chisel-shaped tip (0.5×1.1mm, 114 mJ/pulse at the tip end) was set according to the manufacturers' recommendations (160 mJ, 10 Hz). Irradiation was performed from the coronal to the apical with a 15–20 degree tip inclination. ERL was performed without anesthetic. When patients complained of pain, a topical periodontal anesthetic gel (Oraqix®, Dentsply, USA) was applied in the periodontal pocket.
A total of 586 and 678 sites were treated with ERL and SRP, respectively.
Procedure comfort
A visual analogue scale (VAS) was used to evaluate patient comfort after each treatment session. Zero corresponded to total discomfort and 100 to maximum comfort.
Statistical analysis
A Wilcoxon signed-rank test was performed to determine the significance of the results pertaining to CAL and PPD (significance level of 5%). For BOP and patient comfort scores, a paired Student's t test was used (significance level of 5%). Normality was assessed via the Kolmogrov–Smirnov test. Statistical analysis was performed using SAS 9.2.
Results
Anesthetic use during procedures
Only 5 of 19 patients complained of minimal pain during ERL.
Baseline scores
The initial scores for the clinical parameters investigated in both groups were similar, with non-significant differences of 0.12 (p=0,11), 0.09 (p=0,15), and 1.63 (p=0.55) for CAL, PPD, and BOP, respectively (Figs. 1 –3).
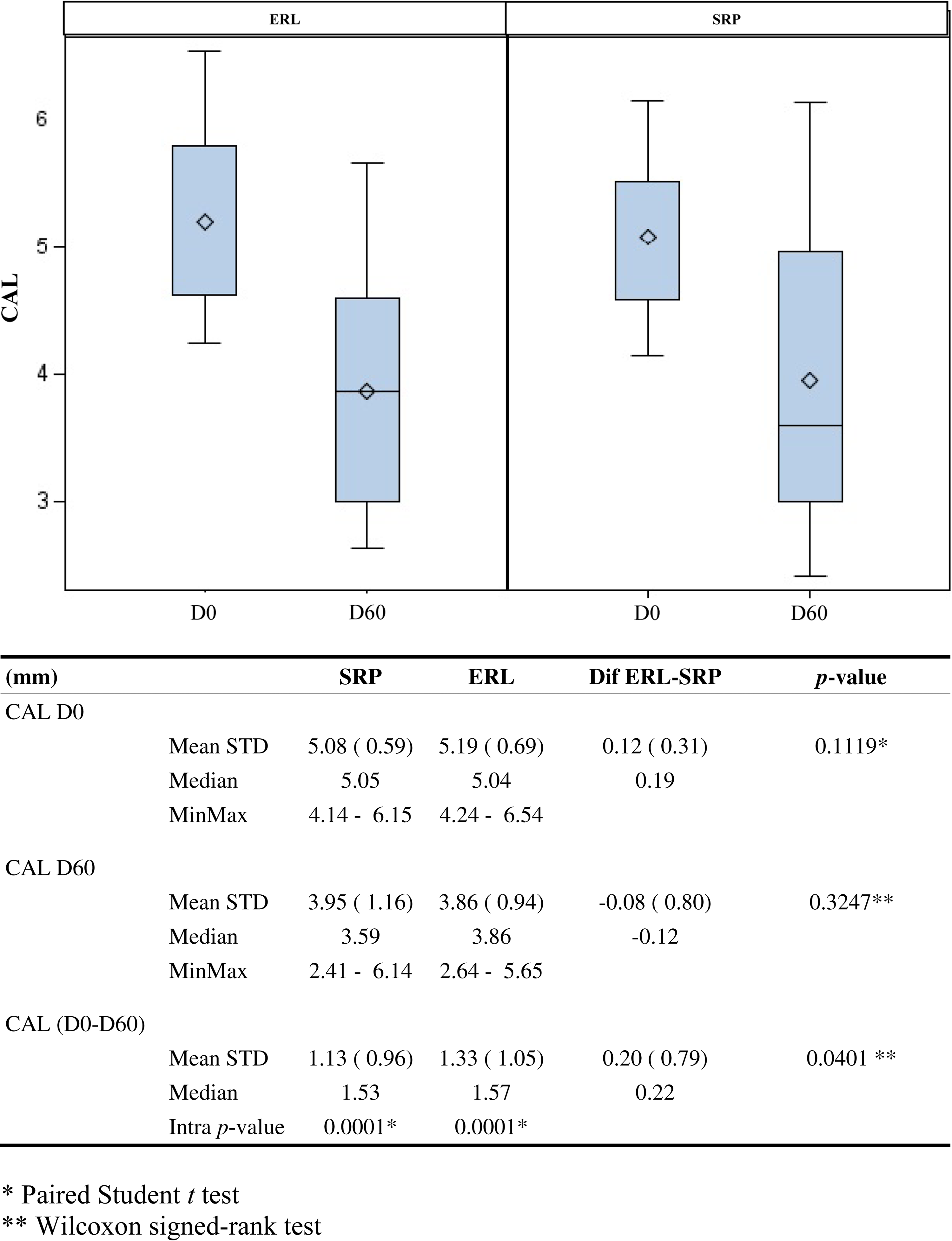
Clinical attachment scores at baseline (D0) and reevaluation (D60). CAL, clinical attachment level; SRP, scaling and root planing; ERL, Er:YAG laser debridement; STD, standard deviation; dif, difference; intra, intra-group.
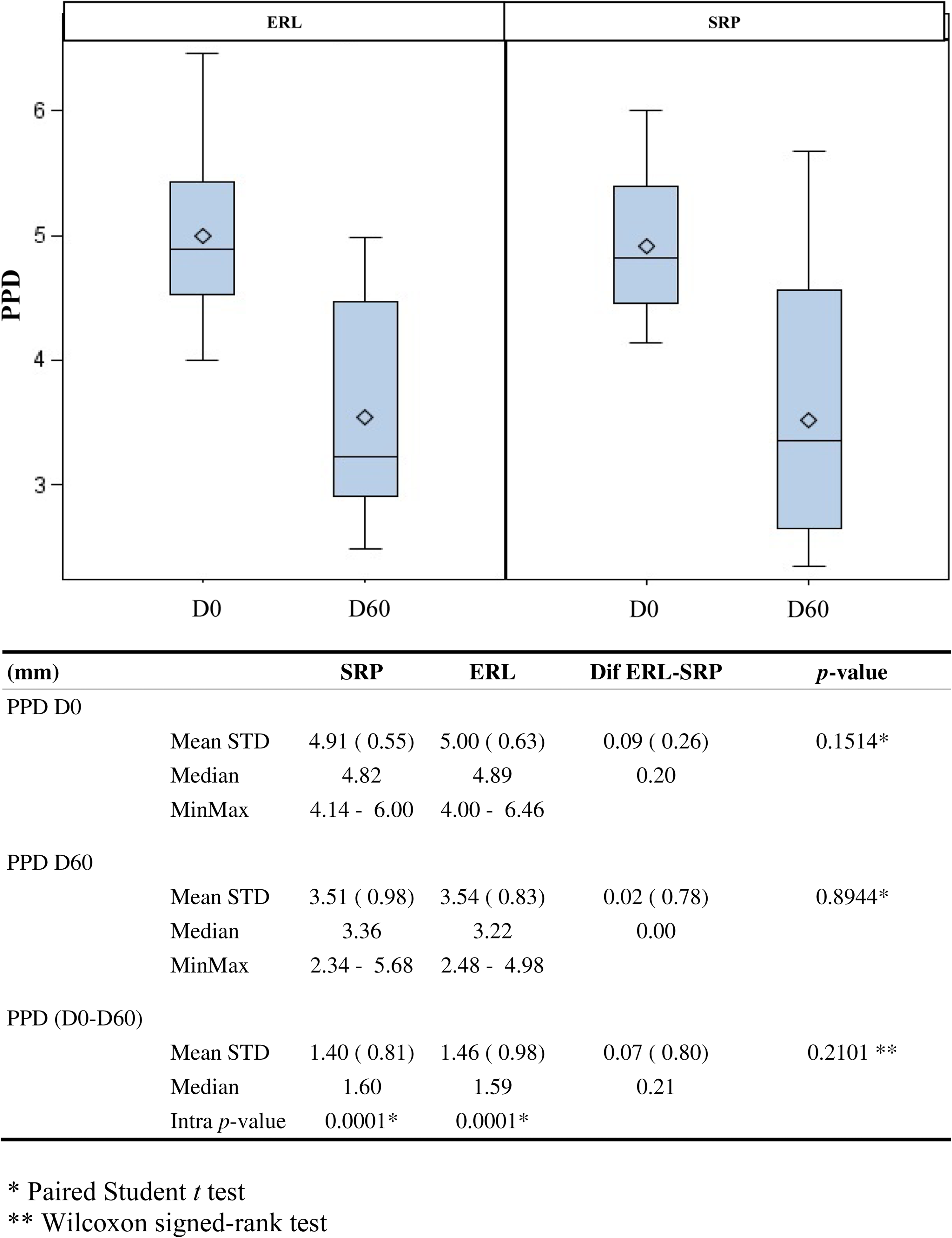
Pocket depth scores at baseline (D0) and reevaluation (D60). PPD, periodontal pocket depth; SRP, scaling and root planing; ERL, Er:YAG laser debridement; STD, standard deviation; dif. difference; intra, intra-group.
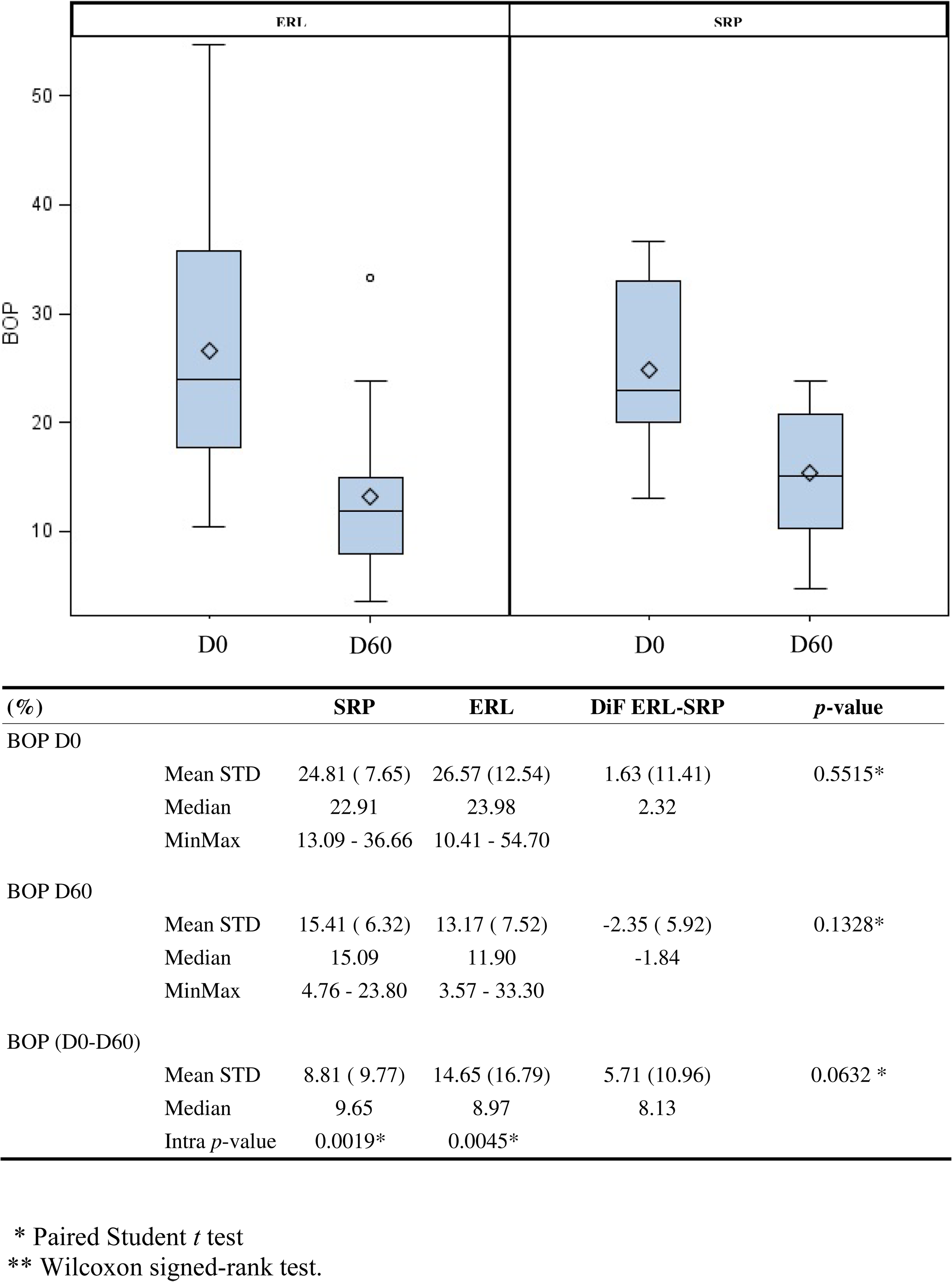
Bleeding on probing scores at at baseline (D0) and reevaluation (D60). BOP, bleeding on probing; SRP, scaling and root planing; ERL, Er:YAG laser debridement; STD, standard deviation; dif, difference; intra, intra-group.
CAL
A significant reduction in CAL was found in both groups, when compared to baseline scores (p<0.001). At reevaluation, a significant reduction in CAL was found within the ERL group, when compared with SRP (p<0.05) (Fig. 1).
PPD
The results demonstrated a significant reduction in PPD in the ERL (p<0.001) and SRP (p<0.001) groups, when compared with baseline scores. Comparison of the two treatment modalities showed a slight but not statistically significant reduction in PPD (p=0.07) in the ERL group, compared with the SRP group (Fig. 2).
BOP
A significant reduction in BOP was found in both groups, when compared with baseline scores (p<0.001). At reevaluation, BOP reduction in the ERL group was higher than in the SRP group, although the difference was not statistically significant (p=0.06) (Fig. 3).
VAS scores
VAS scores in the ERL group were higher than those in the SRP group (Fig. 4), although the difference was not statistically significant.
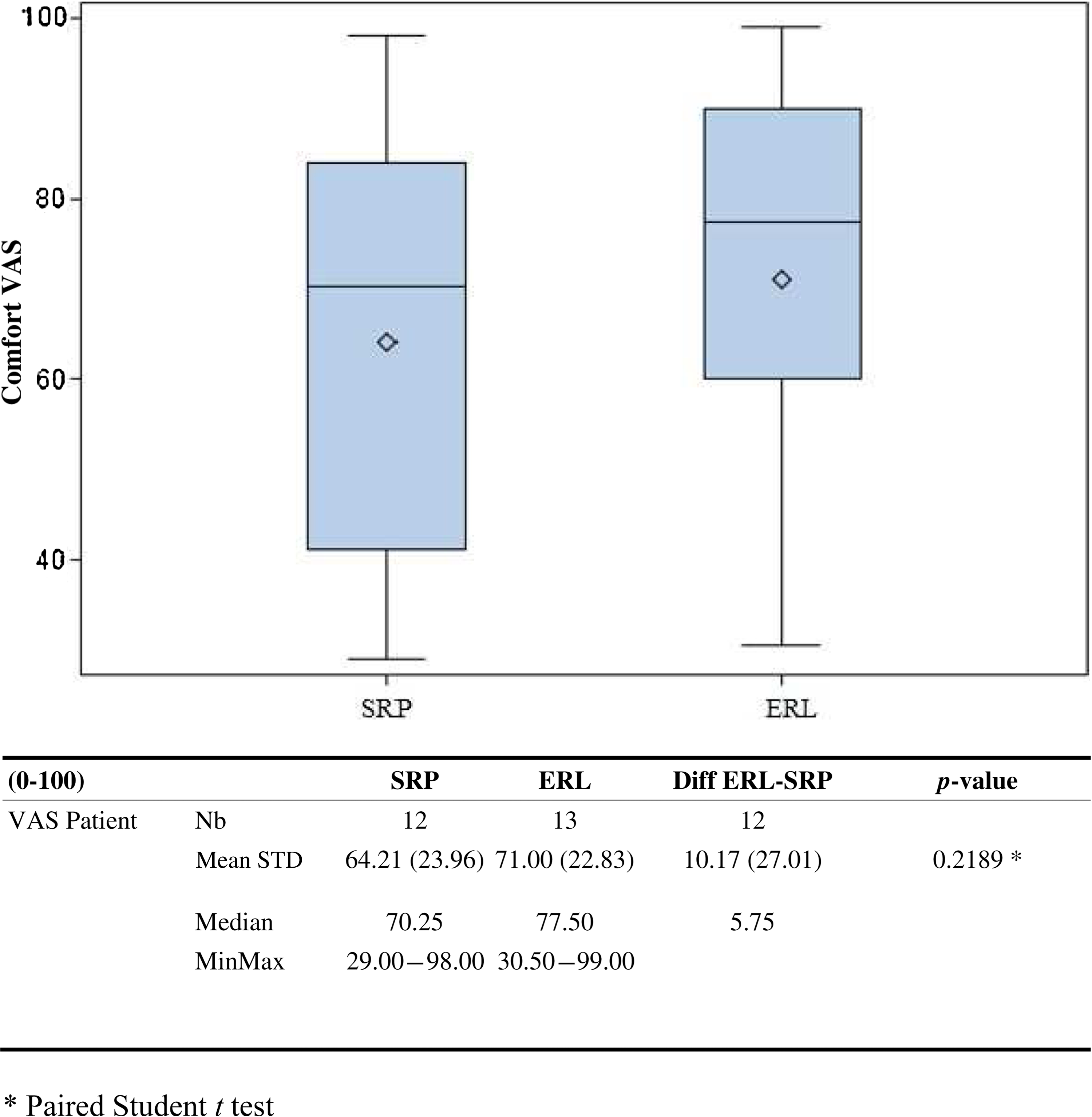
Patients comfort using a visual analogue scale (0–100 range). VAS, visual analogue scale; SRP, scaling and root planing; ERL, Er:YAG laser debridement; STD, standard deviation; dif, difference; Nb, number.
Discussion
In this study, no adverse reactions were noted after ERL or SRP. The study showed significant intra-group improvement in all parameters. Its results were in accordance with those of previous studies that have shown that both treatment modalities can successfully and significantly enhance periodontal clinical parameters. 13 –16 Comparing the outcomes of the two treatment modalities, ERL resulted in greater improvements in PPD and BOP, although the results were not statistically significant. Statistically significant superiority was found only in CAL scores (p<0.05). The results confirmed the assumption that ERL induces less GR at 2 months than does SRP. However, this hypothesis seems inadequate to explain our results, because this finding is inconsistent with previously published data showing that the effects of both therapies on GR are equivalent. Previous studies comparing ERL to mechanical (manual or ultrasonic) debridement have shown a tendency for ERL to be more or less superior 1 month after treatment, although, after 3 months, the difference in clinical parameters tends to be non-significant. 13,17 In our study, clinical outcomes were measured 2 months after therapy, which was an intermediate end point, compared with the intervals set in previous studies. Therefore, we can suppose that the short-term superiority of ERL was diminishing at that time, and this could explain the slight superiority found for ERL (significant only for CAL).
Systematic reviews and meta-analyses have shown heterogeneity in the treatment outcomes of ERL in published clinical studies. 7,12,18 This is because of differences in clinical protocols and laser settings, as well as the relatively small numbers of patients included in previous studies. From our point of view, the data consistently support the idea that ERL can be successfully applied as an alternative to the conventional mechanical treatment of chronic periodontitis. On the other hand, it remains to be seen whether the slight superiority of ERL (regardless of statistical significance) in improving clinical parameters implies clinical relevance in terms of mid- and long-term prognosis.
One of the major advantages of ERL noted by this study is that it is less painful and less invasive than mechanical treatment. Pain felt during ERL was easily managed by applying Oraqix gel. Systematically applying periodontal anesthetic gel before ERL enhanced patient comfort by averting the use of conventional injection anesthetics.
Another issue for further discussion is use of the calculus detection system (feedback system). Previous studies with continuous laser beams have not generated better results than studies that have used the feedback system. Our results showed that this system yielded significant clinical improvements in all clinical parameters. The detection system reduced operating time and prevented unnecessary elimination of sound cementum. It also permitted practitioners to determine an objective debridement end point, which is preferable to the subjective assessments that operators must perform (using a probe) when performing mechanical treatment.
Conclusions
Within the limits of this pilot study, ERL appears to be an alternative to mechanical treatment in the management of chronic periodontitis in nonsmoking patients. ERL may also be performed without injectable anesthetics. Future studies, with larger samples, are needed to determine the long-term clinical outcomes of ERL.
Footnotes
Acknowledgments
This study was supported by the CHU of Nantes (Appel d'offre interne). The authors thank Véronique Le Gac for assistance as clinical research assistant, and Lucie Planche for assistance in statistical analysis of data. We also thank Kavo France and Pierre Fabre Oval Care for supporting our work.
Author Disclosure Statement
No conflicting financial interests exist.