
Abstract
Introduction
Patients with candidiasis often report burning, an unpleasant taste that is bitter or salty, taste alteration, and, sometimes, pain and discomfort, dysphagia, nausea, vomiting, and diarrhea. Such symptoms can disrupt feeding and lead to a change in quality of life of the patient. 2
Treatment with topical or oral antifungal agents, such as nystatin, amphotericin B, or fluconazole is able to achieve only transient response during treatment, in general for 15 days. Recurrences are very common, considering the multifactorial etiology of candidiasis, and widespread use of fungicides has resulted in the development of resistant species, especially Candida albicans. 3 In addition, antifungal agents can reduce the effectiveness of antiretroviral drugs, worsening the general health of the patient. 4
Antimicrobial photodynamic therapy (aPDT) has been shown to be an effective alternative to the use of antifungal agents. 5,6 It consists of the use of a photosensitizer, activated by a light source, which reacts with oxygen causing cell death. This effect occurs when the photosensitizer absorbs light energy and produces reactive substances that lead to cell damage, mainly by oxidation. This technique has shown to be effective against micro-organisms, including those resistant to antifungals, 6 and there are no side effects related to the topical modality of this therapy if it is used with the appropriate parameters. 7
Reports from the literature show that methylene blue combined with a red laser is an effective photosensitizer to be used in aPDT in animal models of oral candidiasis. 8,9 Despite considerable research evaluating the effects of aPDT in animal models, there is a scarcity of data regarding the treatment of patients. In this work, we report a preliminary study that investigated the feasibility of the use of aPDT as an antifungal therapy for oral candidiasis in HIV-infected patients, and compare the results with those of fluconazole, a well-established antimycotic.
Materials and Methods
Twenty-one patients of either gender (16 males and 5 females, mean age 30±8 years) with HIV-antibody seropositive infection of 5–7 years' duration; and clinical features of oral candidiasis (characterized by complaints of burning sensation on the mucosa, loss of filiform papillae, and varying degrees of erythema) distributed on cheek mucosa, dorsum of the tongue, and hard palate who were followed by the Customer Service Specialist at the City of Ponta Grossa (PR, Brazil) were enrolled in this study. Smokers, pregnant women, and patients who used removable partial or total dentures and those who were under radiotherapy or chemotherapy were excluded. All selected patients were informed about procedures to be conducted and agreed to participate in the research as a volunteer. They signed a written statement of informed consent prior to receiving treatment. The clinical study protocol was approved by the Ethics Committee on Human Research of State University of Ponta Grossa.
Patients were randomly divided into three groups of n=7 individuals with at least one female per group, and on initial visit, oral swabs were taken from mucosa to confirm the diagnosis of candidiasis by culture on Sabouraud agar.
Control group (CG) was subjected to treatment with oral antifungal fluconazole, 100 mg/day during 14 days, 10 Laser group (LG) received a single session of low-level laser irradiation (Twin Laser, MM Optics, São Carlos, Brazil), λ=660 nm, P=30 mW, beam area of 0.04 cm2, and fluence of 7.5 J/cm2 in contact with the mucosa for 10 sec per point. Nine points of the affected area were selected. APDT group (aPDTG) received methylene blue (450 μg/mL) during 1 min (pre-irradiation time) applied with sterile cotton swab on the affected area followed by laser irradiation using the same parameters described previoiusly. 8
Clinical efficacy response was evaluated by (1) changing signs and symptoms from the baseline, that is, before treatment, and by (2) semiquantification of colony forming units of Candida spp. cultures from swabs taken at the same sites used before treatment. 11 For the first approach, the evaluation was rated as better (minimal signs and symptoms with no residual visible candidiasis), unchanged, and worse. Following the initial visit, patients were clinically examined every 2 days. At the end of the treatment phase, the clinical response rate was evaluated.
For the second approach, samples were collected from mucosa on days 7, 15, and 30 after the procedure (all groups) using oral sterile swabs on the affected area and immediately seeded on Sabouraud agar plus antibiotic (Micobiotic agar, Laborclin, Paraná, Brazil). The tubes were stored at room temperature for assessment of cultures. Results were then scored as (1) low, (2) moderate, and (3) abundant growth of the fungus in the cultures, according to the medium turbidity: clear, mild, and intense, respectively (Fig. 1).

Medium turbidity of Candida spp.
Results
A total of 21 patients were evaluated. Before beginning the treatment, all patients had oral candidiasis and showed abundant growth of Candida spp.
From the control group, on the 15th day (after 14 days of fluconazole administered) five out of seven patients (72%) showed clinical improvement and in 28% the clinical picture was unchanged. On day 30, a recurrence of signs and symptoms was seen in 72% of patients (Fig. 2). Regarding Candida spp. growth, 7 days after fluconazole and at the end of treatment (15 days) two patients still presented moderate growth of the fungus (mean score 0.6). Thirty days after the beginning of the treatment, five out of seven patients showed abundant growth of Candida spp., corroborating the relapse observed in clinical response (mean score 2.3) (Fig. 3).
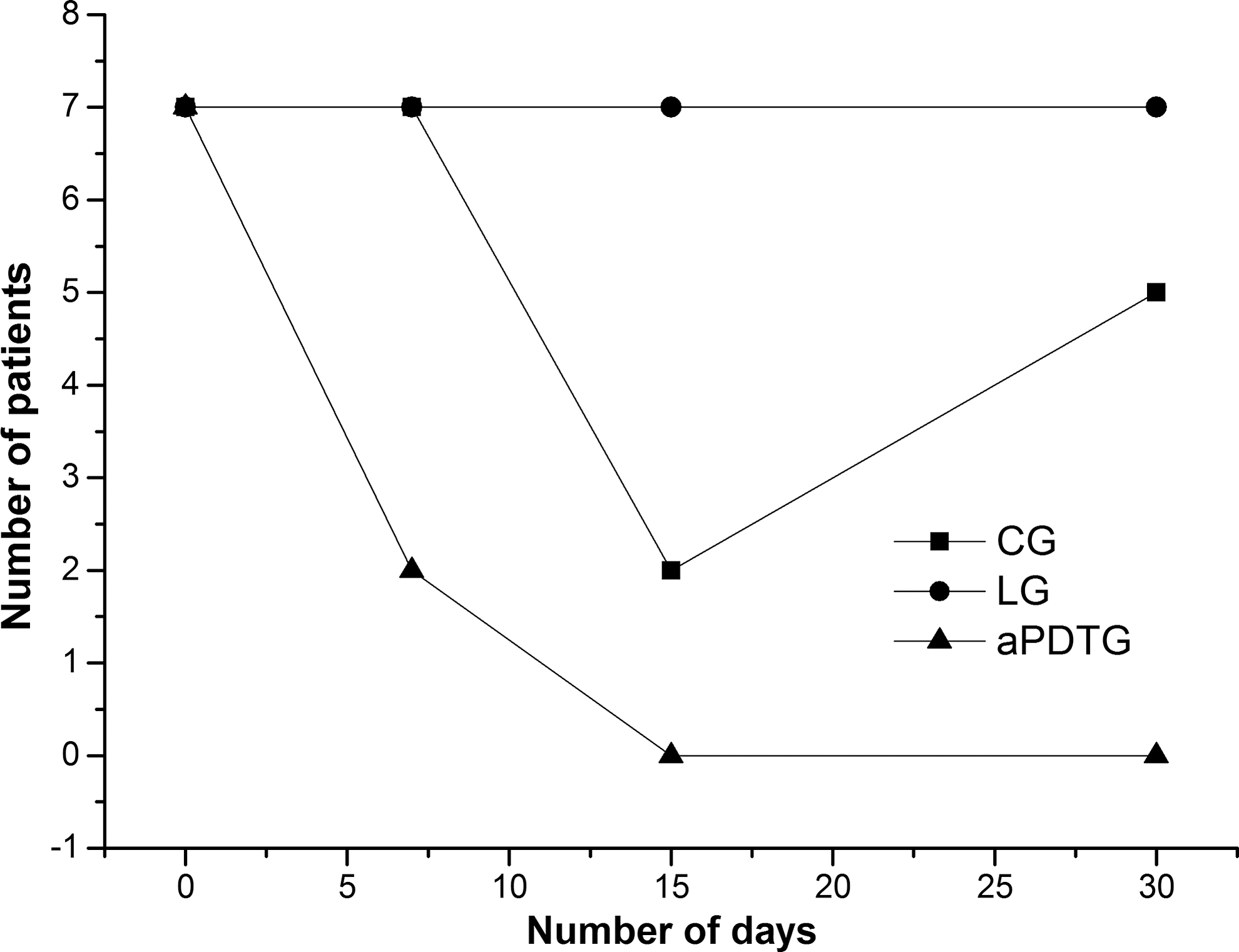
Comparison of disease severity for control (fluconazole), laser, and antimicrobial photodynamic therapy (aPDT) groups during study follow-up.
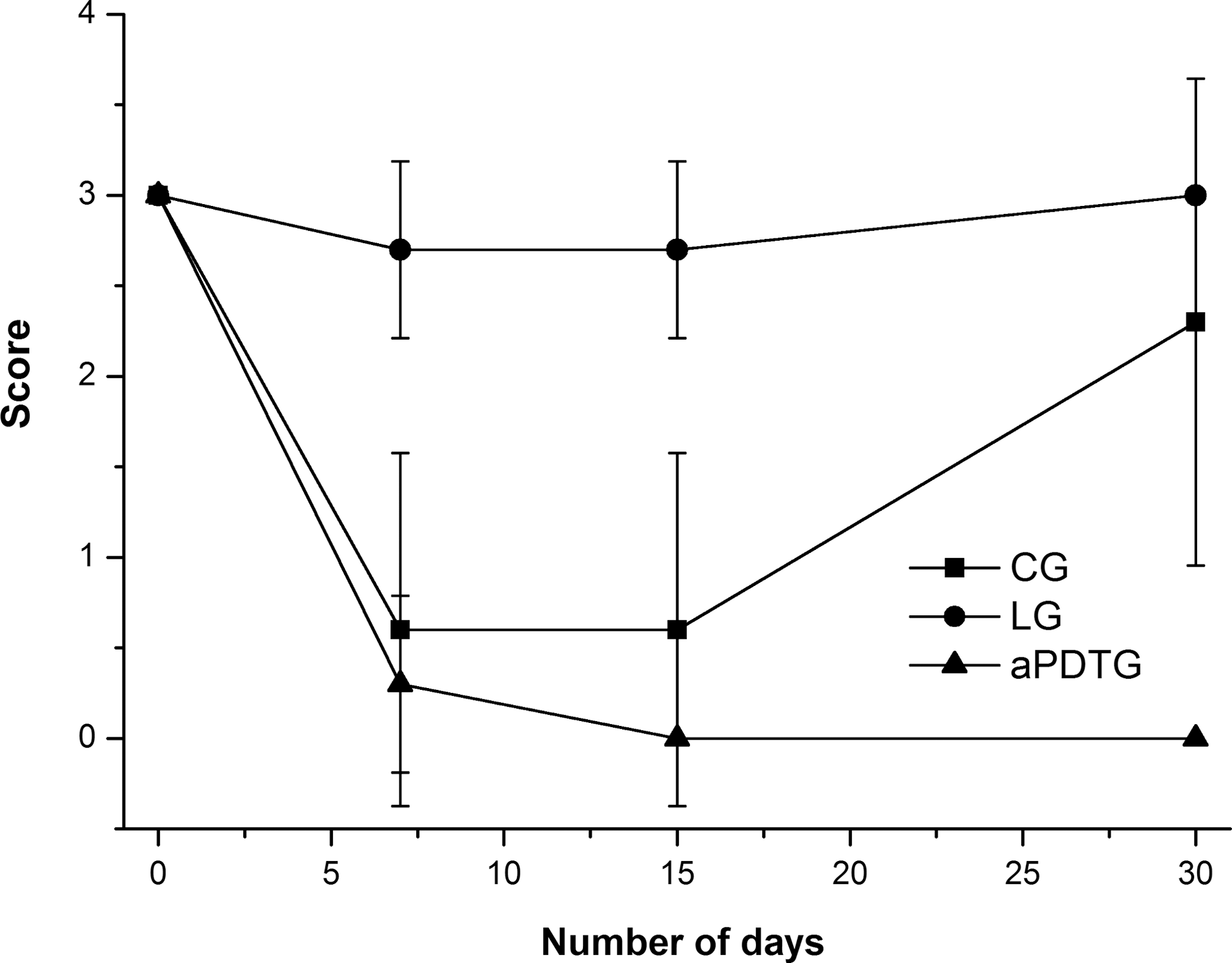
Comparative microbiological semiquantitative analysis for oral swabs collected from control (fluconazole), laser, and antimicrobial photodynamic therapy (aPDT) groups during experimental period.
Low-level laser therapy (LLLT) did not show any efficacy during the experimental period. All patients (7/7) exhibited unchanged clinical signs of candidiasis up to 30 days after start of care. Moderate (two out of seven patients) to abundant growth of Candida spp. (five out of seven) was observed on the 7th and 15th days (mean score 2.7). Thirty days post-treatment, the percentage of subjects with abundant yeast colonies was 100% (Figs. 2 and 3).
When patients were treated with aPDT, there was a remarkable decrease in the clinical signs of candidiasis. Fifteen and even 30 days following treatment, seven out of seven patients showed an improved clinical picture and improved general health (Fig. 2). The microbiological analysis showed that 7 days post-treatment, two patients (28%) exhibited low growth of Candida spp. (mean score 0.3). Fifteen and 30 days after treatment, aPDT was effective to completely eradicate yeast cells in 100% of patients (Fig. 3).
After the 30 day experimental period, patients from the control and laser groups received aPDT and were followed up with preventive strategies under the regular guidelines of the institution.
Discussion
Oral candidiasis caused by Candida spp., mainly C. albicans, is recognized as one of the most frequent opportunistic infections in HIV-infected individuals. Our preliminary clinical trial demonstrated that a single session of aPDT was significantly effective in reducing the viability of C. albicans and in improving clinical signs and symptoms of oral candidiasis, in addition to preventing recurrence even 30 days after the start of care.
Topical azole antifungal drugs are usually used to treat oral candidiasis. Systemic fluconazole is the protocol approved by the Public Health Service in Brazil to care for immunocompromised patients. In this study, 100 mg tablets of fluconazole were administered daily during 14 days. Despite clinical improvement in the first 15 days of medication, our data showed that no significant reduction of the fungus was observed, allowing Candida spp. recolonization after 30 days, and, consequently, disease relapse and worsening of the general health status of the HIV-infected patients. Patients reported the unpleasant taste of the medication as well as diarrhea and abdominal pain. One major concern regarding antifungals is that drug becomes less effective as new dosages are administered. In this situation, patients are instructed to take higher dosages to obtain pain relief, which is considered one of the adverse reactions of combination antiretroviral and antifungal medications. 12
LLLT has been reported as an alternative to antimycotics in denture stomatitis. 13,14 In the present investigation, a group of patients received only red laser irradiation (single session) on the affected mucosa. Our findings revealed that LLLT was not able to reduce yeast colonies at any moment of evaluation (7, 14, and 30 days after irradiation). Interestingly, two patients from this group had Candida spp. growth that increased after 30 days of treatment.
Our data disagree with the study of Maver-Biscanin et al. 13 in which reduction of yeast colonies on agar was observed following red and infrared laser treatment of patients with denture stomatitis. Two hypotheses could explain these conflicting results. The first one involves light parameters and irradiation protocol. We used a 30 mW red laser in a single session, 7.5 J/cm2/point during 10 sec on nine points of the affected mucosa. Those authors also used a 30 mW-red laser, however, the fluence was 3 J/cm2 during 10 min scanning palatal mucosa for 5 consecutive days.
The second plausible explanation could be related to the virulence factors of the pathogen C. albicans. The overall severity and chronicity of oral candidiasis has been attributed to the HIV-induced immune deficiency of the affected individuals. 15 On the other hand, both plaque accumulated on the denture and poor oral hygiene contribute to the virulence of Candida, offering the clinical picture of Candida-associated denture stomatitis. 16 Although we do not have data to support our premise, recent work reports the increase in the quantitative expression of four virulence factors in C. albicans isolates from HIV positive compared with isolates from HIV negative individuals. 17
We decided to assay the effects of aPDT on immunosuppressed HIV-infected individuals, as the literature has demonstrated satisfactory results in immunocompromised mice. 8 We used the more effective methylene blue concentration reported by those authors. We observed that individuals from the aPDT group showed reduction of clinical signs and eradication of the fungus at colonies. Furthermore, patients reported pain relief immediately after irradiation and even up to 1 month after no relapse was verified.
aPDT generates reactive oxygen species (ROS) that react with membranes and other organelles to kill microbial cells by oxidative stress. In vitro studies demonstrate selective killing of micro-organisms under conditions in which mammalian cells were unaffected, 18,19 Clinical trials in dentistry have demonstrated that this therapy could be a new adjuvant approach in root canal disinfection and periodontal disease. 20,21 One other attractive characteristic particular to aPDT is the possibility that the ROS produced from photosensitizer may chemically destroy some virulence factors (especially those that are proteins). 22
Conclusions
Putting together our results and the advantages of aPDT such as being devoid of mutagenicity, low cost, and the ability to destroy virulence factors make aPDT a potential alternative for immunocompromised patients with HIV infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.