
Abstract
Introduction
It has also been suggested that removal of the smear layer may enhance the seal of the root canal filling. 9,10 It is usually difficult to clean the apical portion of the root canal with conventional irrigation methods because of its complicated anatomy. 11 Although the combined use of ethylenediaminetetraacetic acid (EDTA) and sodium hypochlorite (NaClO) solution have been recommended for removal of the smear layer from the surface of the root canal wall, 11 –13 but whether these irrigants can remove the smear layer at the apical one third of the canal has not been confirmed. 14 There are areas in the root canal where instruments cannot reach, and these areas remain untreated. 15 Moreover, excess cutting of canal dentin and extrusion of the irrigant beyond the apex are matters of concern. 16 Extrusion of irrigants such as NaClO often results in severe periapical tissue damage. 17,18
Lasers were recently applied to shaping of the root canal. 19 The Er:YAG laser is highly absorbed by water and hydroxyapatite. When the Er:YAG laser is irradiated, water contained in dental hard tissues is evaporated instantaneously, and the surrounding tissue is thereby ablated. In the root canal, dentin ablation by Er:YAG laser irradiation removes debris and the smear layer from the root canal wall, and opens the dentinal tubules. It leads to ablation of dental tissues without causing fusion, cracks, or carbonization. Er:YAG laser irradiation could be applied to shaping of the root canal. Appropriate parameters of Er:YAG laser irradiation during shaping of the root canal should be used to minimize thermal damage to periodontal tissues. 20 These findings led us to assume that root canals could be prepared by Er:YAG laser irradiation without producing debris, a smear layer, or any thermal side effects on periodontal tissues. 21 It is difficult for the conventional laser tip to deliver the laser beam to the root canal wall, especially at the apex area. If the laser beam is irradiated at the periapical portion, the laser beam might injure the periapical tissue. Irradiation to the side becomes possible by improving the tip, and it can evaporate the root canal wall dentin. Irradiation of the root canal wall with the fine-tipped Er:YAG laser has made it possible to cut root canal wall dentin and enlarge root canals. 22
Er:YAG laser irradiation is expected to have bactericidal effects. Ando et al. suggested that laser irradiation might inhibit bacterial growth or evaporate viable bacteria in the irradiated area by causing explosive ablation. 23 These findings indicated that growth inhibitory zones may be a result of the bactericidal effect of the Er:YAG laser. Schoop et al. found that Er:YAG lasers were capable of eradicating Enterococcus faecalis to a significant extent. 24 Furthermore, it was reported that irradiation to the root canal system efficiently reduced the viability of intracanal bacteria. 25 Noiri et al. reported that anti-biofilm and microbial procedures with an Er:YAG laser were expected to be beneficial. 26 The Er:YAG laser might be suitable for clinical application as a suppressive and removal device of biofilms in endodontic treatments.
However, few reports have studied the cutting degree of horizontal area of the root canal using Er:YAG laser irradiation. The objectives of this study were to evaluate the cutting degree of horizontal area of the root canal; the Er:YAG laser irradiated surfaces were observed using microfocus X-ray computed tomographic photography (micro CT).
Materials and Methods
All experiments in this study complied with the guidelines of the Ethical Review Board of Tokyo Medical and Dental University (No. 518).
Preparation of samples
Six incisors extracted from human mandibles were used. In this study, intact straight roots with similar diameters were selected. After the soft tissues were removed from the root surface, root samples, 7 mm in length, were prepared by removing the crowns with a high-speed hand piece. They were then embedded in epoxy resin blocks (Buehler, Lake Bluff, IL). The root apex was covered with utility wax (GC, Tokyo, Japan). After confirming the patency of the root canals, they were prepared using K-files (Zipperer, München, Germany) in 0.5 mm increments until reaching size #25. Working lengths were set at 6.5 mm. The coronal portion of the root canal was enlarged with Gates-Glidden burs (#3-4; Mani, Tochigi, Japan). After shaping of the root canal, the root canal was irrigated with 5 mL of saline solution.
Experimental procedure
Figure 1 shows the procedure of the experiment. Each sample was fixed to a custom-built jig for exclusive use of micro CT (SMX-90CT; Shimadzu, Kyoto, Japan) (Fig. 2). The tips were custom made. They do not have a lot number. The jig was used to scan the samples at the same position in the micro CT device. Before laser irradiation, the samples were scanned by micro CT.
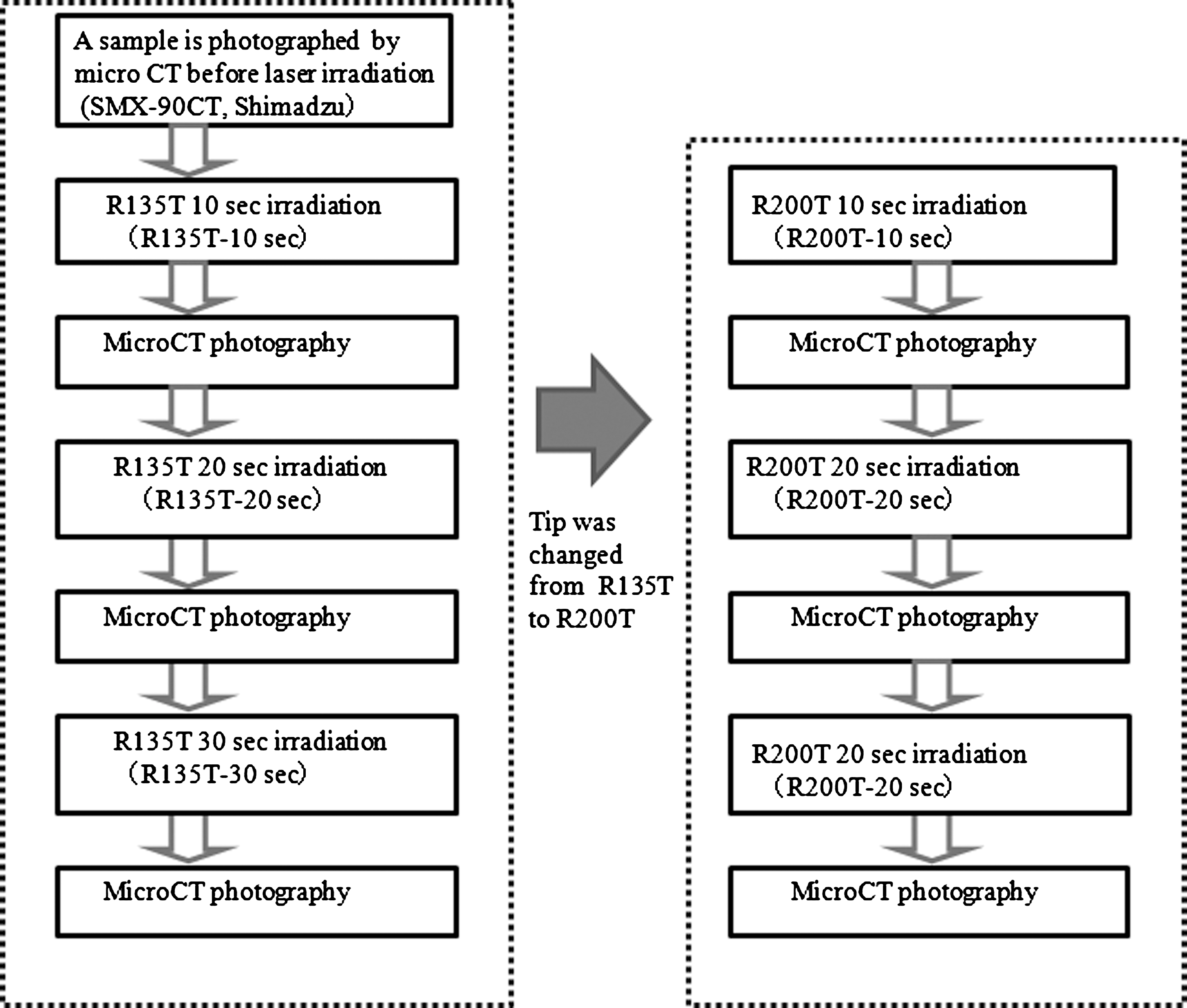
Laser irradiation and computed tomography procedure. Micro CT was performed for every laser irradiation for 10 sec.

Root samples were embedded in epoxy resin blocks fixed to a custom-built jig for exclusive use of micro CT.
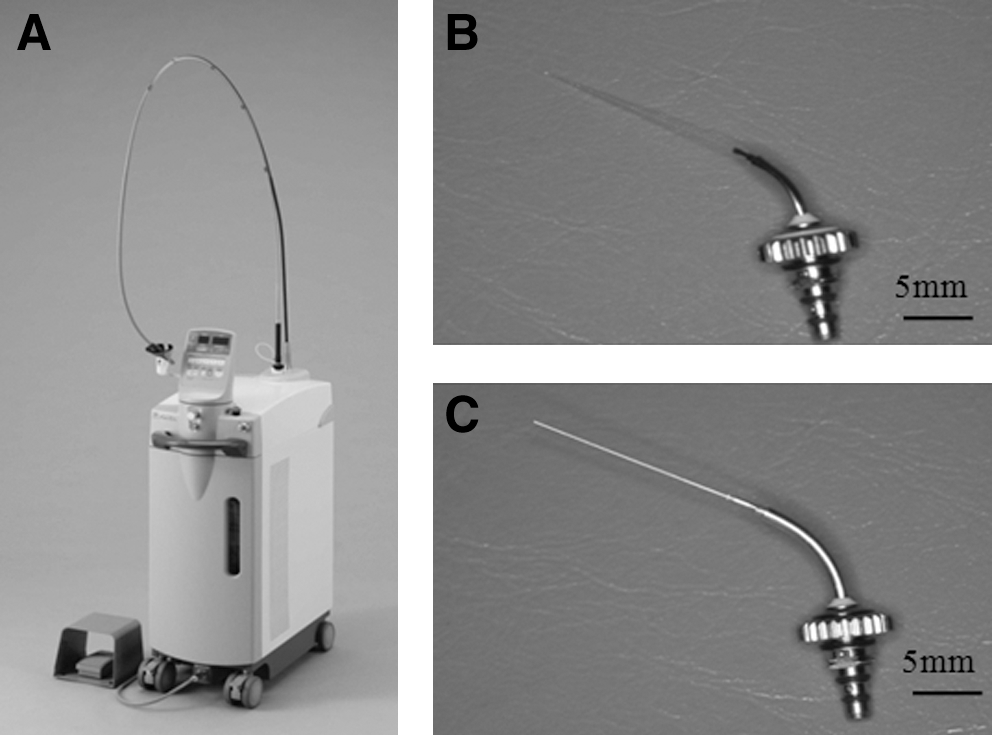
Er:YAG laser equipment (Erwin AdvErL; Morita, Kyoto, Japan) (Fig. 3A) and cone-shaped irradiation tips (R135T, φ=185 μm and R200T, φ=280 μm) (Fig. 3B, C) attached to the hand piece were used for this study. The irradiation tip point was positioned at 1 mm from the apical foramen within the root canal. The outer diameter of tip of R135T was 185 μm, and the root canal at 1 mm from the apical foramen was estimated to be 270 μm. The irradiation conditions of the Er:YAG laser were 30 mJ and 20 pps, and water was sprayed from the tip at 5 mL/min. An Er:YAG laser was then irradiated. First, the root canal was irradiated for 10 sec with the R135T tip (R135T-10 sec) (Fig. 4A). The sample was then placed back into the micro CT device using the jig, and an image was obtained. Further laser irradiation was performed for an additional 10 sec in the same fixed position with the R135T tip (R135T 20 sec), and another micro CT image was obtained. Final irradiation was performed for 10 sec, and a micro CT image was obtained (R135T 30 sec) again. Next, the tip was changed to R200T (Fig. 4B), and the same process tip was repeated (R200T 10 sec, R200T 20 sec, and R200T 30 sec). In total, seven micro CT images were obtained before and after each irradiation for each sample. The new tip was used for each sample. A total of six R135T, and six R200T tips were used.

Root canal irradiation with R135T.
Evaluation
To evaluate the cutting degree of horizontal area of the root canal, Er:YAG laser irradiated surfaces were observed using micro CT. The micro CT exposure conditions were as follows: normal scan mode, tube voltage of 90 kV, tube current of 100 μA, and digital flat panel detector of 52.5×52.5 mm (1 pixel=30×30 μm). The data obtained from all samples were saved as 8-bit JPEG files and 512×512 matrix data. Pictures of horizontal sections 1 mm from the apical foramen within the root canal were reconstructed. With imaging software (Photoshop CS, ver. 7.0; Adobe, San Jose, CA), micro CT pictures taken from each aforementioned sample were measured in terms of the amount of cutting change of root canal wall dentin 1 mm from the apical foramen within the root canal in the horizontal section. First, color-gamut specification of the white part (dentin) of pictures was carried out in the selection range. The number of pixels at the root canal area was then counted using a histogram. The amount of change after each laser irradiation was displayed in pixels. The numbers of pixels in each image were counted and averaged for each sample. The root canal area before and after each irradiation was compared (Fig. 5).
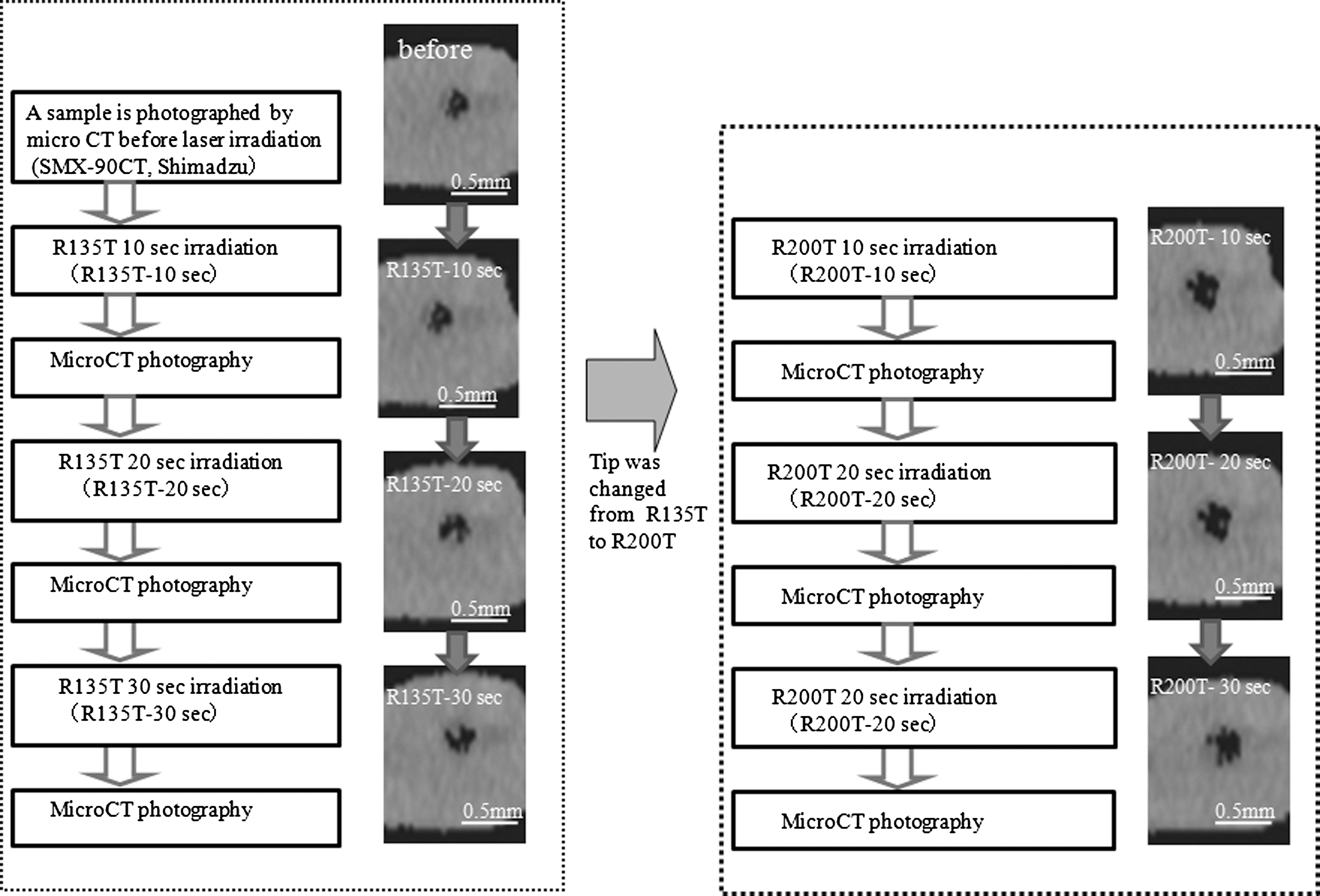
Representative micro CT image in each group.
Statistical analysis
The obtained data were statistically analyzed with one-way analysis of variance and the Tukey–Kramer test; the significance level was set at p=0.05.
Scanning electron microscope (SEM) observation
All samples were observed with an SEM (S-4500; Hitachi High-Technologies Co., Tokyo, Japan) to investigate morphological changes on root canal wall dentin surfaces.
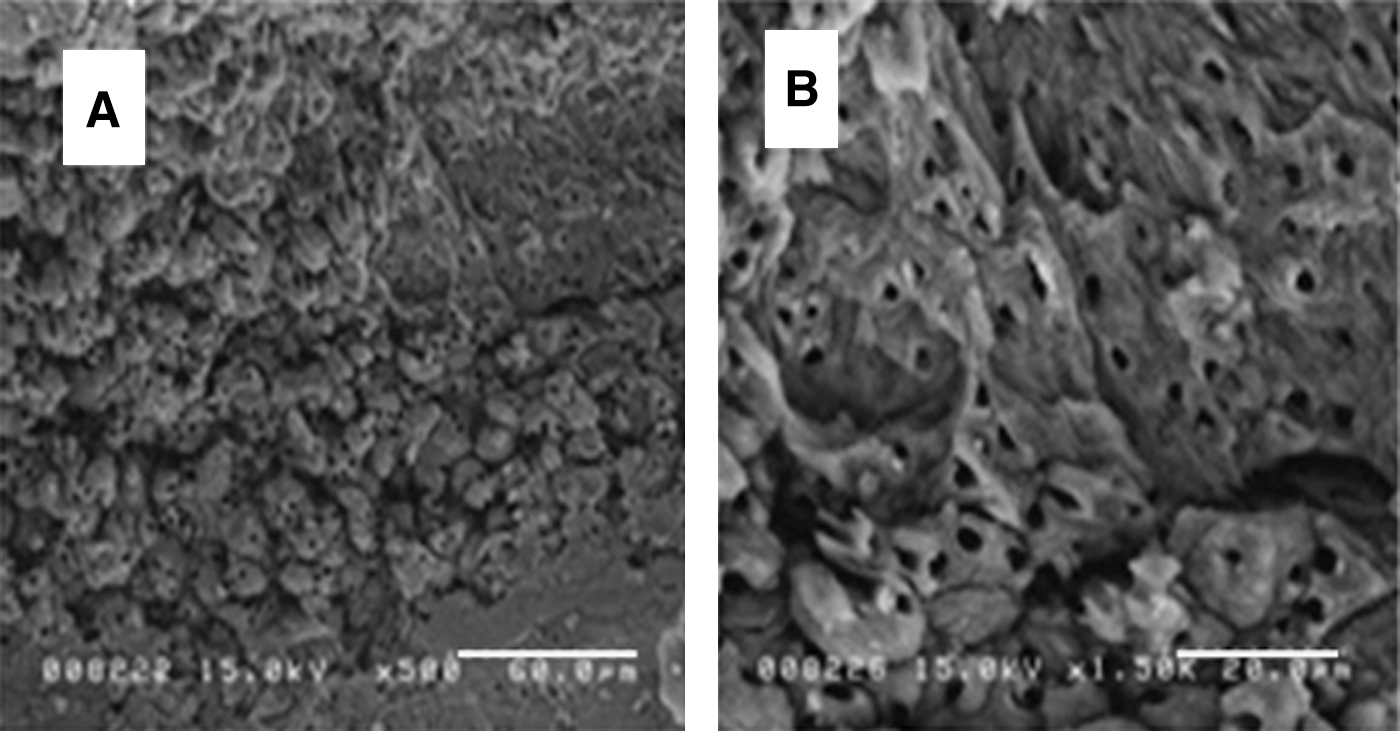
The root was sectioned and then split longitudinally into two halves at its buccolingual aspect for SEM observation. The specimens were dehydrated in a graded series of ethanol solutions, coated with platinum, and observed under the SEM at 15 kV. Areas 1 mm from the apical foramen within the root canal were photographed at 500× and 1500× magnification.
Results
Figure 6 shows the increase of root canal area evaluated by cross section in each experimental procedure. R200T 10 sec significantly enlarged the root canal area (0.12±1.07 mm2) compared with the other procedures (p<0.05). The increasing rate of root canal area decreased with exposure time.
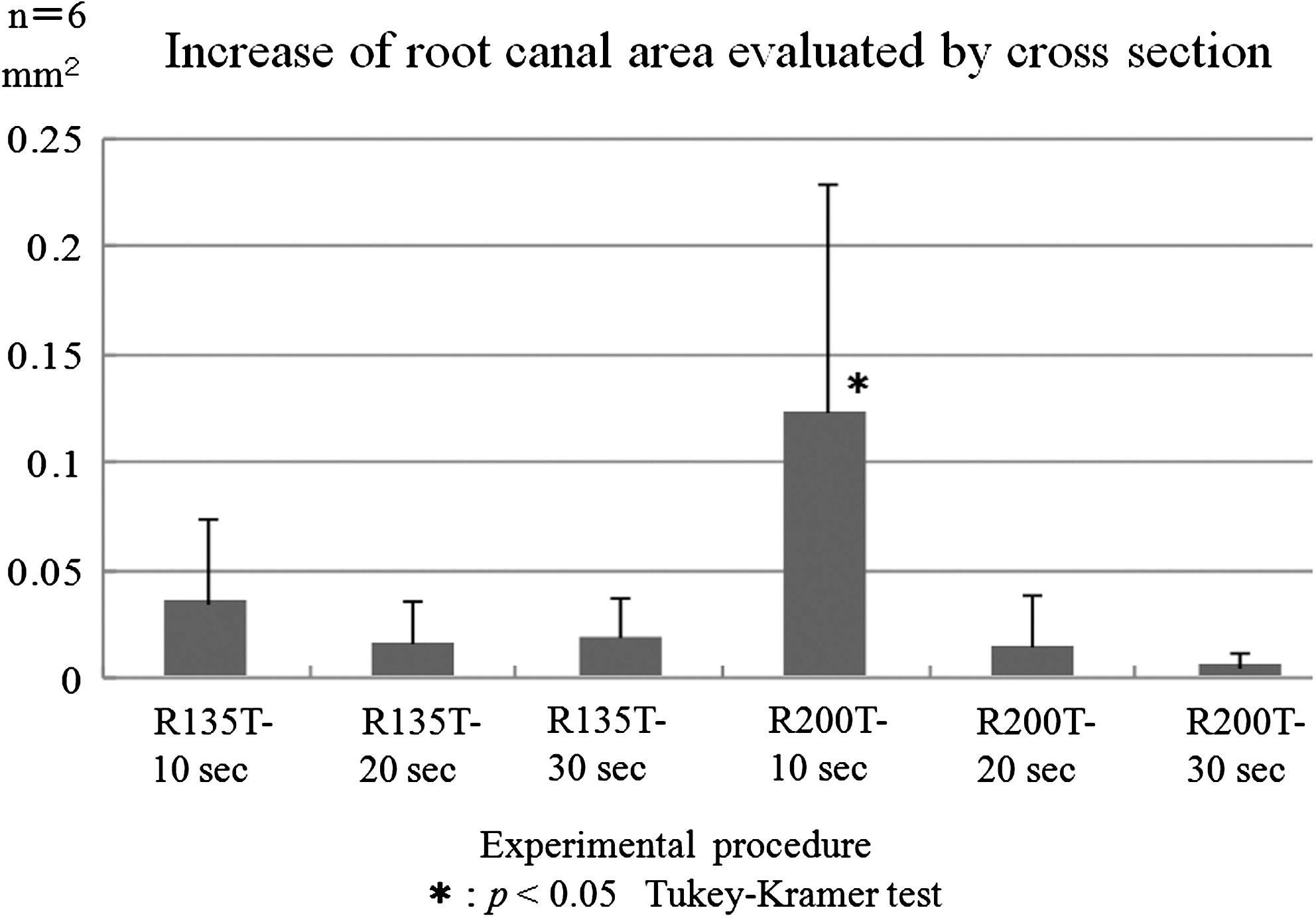
Increase of root canal space evaluated by cross section. The amount of change in the sectional area following each experimental procedure is shown. R200T-10sec most significantly enlarged the root canal area compared with the other procedures (p<0.05).The increasing rate of root canal area decreased with exposure time.
A representative SEM micrograph taken at low magnification (500×) is shown in Fig. 7A. No smear layer was observed, and the dentinal tubules were open. Observation of the same sample at higher magnification (1500×) revealed that there was no obvious carbonization or fusion (Fig. 7B). The same results were observed in the other samples.
Discussion
In the conventional method, hand files and Gates-Glidden drills are mainly used to prepare root canals in the clinic. Adorno et al. found that shaping of the root canal alone, regardless of the technique used, can potentially generate cracks in the apical root canal wall as well as on the apical root surface, 27 which might lead to root fracture. Dang et al. suggested that small, blind fractures were produced and stored by root canal treatment, and that with additional stresses applied through restoration or mastication, these fractures might manifest as complete fractures. 28 Root fracture could result from the conventional root canal treatment. Moreover, it is thought that dentin strain caused by mechanical shaping of the root canal may induce root fracture. Nalla et al. found that human dentin fractures might be caused by strain. 29 The mean maximum dentin strain under water cooling caused by Er:YAG laser is significantly smaller than that by Nd:YAG laser. 30 Also, water cooling greatly reduced the dentin strain in both lasers. Therefore, shaping of the root canal with Er:YAG laser irradiation, might reduce the risk of root canal dentin crack formation especially at the apical portion. No crack formation was observed in the apical root canal wall or on the root surface in this experiment.
Er:YAG laser irradiation might reduce the risk of root canal dentin crack formation especially at the apical portion. No crack formation was observed in the apical root canal wall or on the root surface in this experiment.
Er:YAG laser irradiation causes evaporation of water from the most superficial layer of the tissue because its wavelength 2.94 μm is very close to the high absorption band of water. When it is irradiated, water contained in dental hard tissues evaporates instantaneously and thereby ablates the surrounding tissue. Therefore, among the several laser systems, the Er:YAG laser ablates dental hard tissues most effectively and efficiently. The lasing tips used in this experiment were R135T and R200T. They were made of quartz glass with a top angle of 84°. It delivers ∼80% of its energy laterally and only 20% forward. These tips may expand the possibility of shaping of the root canal with the Er:YAG laser. In general, mechanical shaping of the root canal is performed with the use of hand and/or rotary files. However, they do not touch all of the root canal walls, and at the untouched area, the dental pulp remnants and infected dentin may remain. Wu et al. reported that in 25% of the cases, the instrument did not touch the wall at the working length, whereas in the remaining 75%, the instrument was found to bind at one part of the wall. In addition, the smear layer is formed on the canal wall surfaces when the root canal is prepared with hand and/or rotary files. It is evident that the smear layer contains numerous bacteria. 31 A combined use of EDTA and NaClO solutions has been recommended for removal of the smear layer from the root canal walls. 11 –13 However, the effect of these irrigants on the apical one third of the canal is often questionable. O'Connell et al. reported that insufficient irrigation might leave bacteria and result in failed root canal treatment. 14 In our study, adequate removal of the smear layer and achievement of open dental tubules were observed. In addition, because Er:YAG laser irradiation vaporizes moisture, a bactericidal effect on the biofilm is expected. The laser can be irradiated to clean the area that mechanical and chemical cleaning does not affect, 6 which would improve the possibility of successful root canal treatment.
When the tip was exchanged to R200T, distance between tip and root dentin were compared with other conditions. Thus, the greatly cut degree of root dentin was observed. The laser energy is attenuated in an inverse proportion to the square of the distance. Therefore, it is thought that as the distance between the lasing tip and the root canal wall grows by laser irradiation, the cutting degree decreases. Therefore, the cutting degree could increase by using a tip suited to each stage. However, it is considered that the distance between the tip and the root canal wall is not accurately controlled, because the ledging and curvature of the root canal give limited information in terms of the position of the tip. Therefore, it is necessary to perform the flaring in the upper portion of the root canal beforehand. Such coronal flaring would enable the tip to reach the root canal wall more easily. The outer diameters of R135T and R200T tips are 185 and 280 μm, respectively. Therefore, the root canal was enlarged up to file size #25 (diameter, 250 μm) before the lasing tip was inserted, in this experiment. The tip for the root canal irradiation disperses the irradiation energy because of the shape of the tip point.
To avoid abrasion of the tip during root canal irradiation, 30 mJ (the lowest output of the equipment) is recommended, although it is thought that raising the output energy could improve the cutting degree. Moreover, an adequate amount of water must be delivered to cool the dentin surface and radiate the thermal energy that concentrates on the tip. Eriksson et al. reported that the threshold level of temperature increase for bone survival is ∼10 °C for 1 min. 32 In our experiment, laser irradiation was performed near the contact position at 1 mm from the apical portion of the root to prevent excessive heat generation, and the irradiation time was limited to 10 sec. It is thought that the temperature elevation of the surrounding tissue of the root is cooled by the blood flow, surrounding periodontal membrane, and alveolar bone conduction.
Root canal filling after laser irradiation should be reconsidered. Er:YAG laser irradiation could remove the smear layer and clean the canal, but it creates irregular dentin surfaces on the root canal wall. Wave patterns would be observed on the root canal wall surface if and when the lasing tip is scanned. These patterns are caused by the pulsed irradiation of the Er:YAG laser. The moving speed of the tip must be calibrated to prevent the creation of such patterns. 22
One of the keys to successful root canal therapy is to adequately obturate the prepared root canal space. Root canal obturation aims to provide complete filling of the canal in all dimensions to create a fluid-tight seal to prevent ingress of bacteria and their toxins into the periapical tissues. 33,34 After shaping of the root canal by Er:YAG laser irradiation, vertical condensation may be more suitable than lateral condensation for root canal filling because bellows and irregular ruggedness of the wall are usually formed by Er:YAG laser irradiation. Kimura et al. filled root canals with a vertical pressurizing method and compared the amount of dye leakage in the root canal prepared by the laser with that by the conventional method, and found that the degree of apical leakage from the teeth prepared by the laser was not significantly different from control teeth (p>0.01). 35 These results show that shaping of the root canal by laser does not affect apical leakage after root canal filling compared with the conventional method.
In this study, the possibility of shaping of the root canal using Er:YAG laser was indicated. When the tip and root dentin were compared with other conditions, the greatly cut degree of root dentin was observed. Shaping by Er:YAG laser might prevent root fracture, and remove the smear layer efficiently compared with the traditional method. The removal of the smear layer at the apical portion using Er:YAG laser also might be effective and does not affect the surrounding tissues compared with irrigation method.
In this study, Er:YAG laser was irradiated at the only apical area. Irradiation to all areas in root canal dentin is necessary. Therefore, the scanning motion should be considered in further studies. We need to observe smear removal efficiency at the time of moving the tip in dentine, and a cutting situation. Furthermore, we will experiment to investigate influence on the periapical tissue by animal studies or other methods.
Conclusions
When the distance between the tip and root dentin was adjacent, the shaping of root dentin by Er:YAG laser irradiation was definitely observed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.