
Abstract
Introduction
Postoperative care of surgical wounds requires patient information centered on the healing process and early signs of complications. Usually, analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), and long-term anesthetics are prescribed to control these complications. 5,6 However, these drugs can sometimes induce side effects. Therefore, the development of alternative or complementary therapies free of adverse side effects and that concurrently enhance the wound healing process are required. 7
The application of innovative methods such as a low-power laser or low-level laser therapy (LLLT) have demonstrated many benefits in controlling the inflammatory process, helping bone regeneration and wound healing, and decreasing pain and swelling. 8 –10
The most accepted explanation for the enhancement of tissue reparation after the application of therapeutic lasers is that these devices offer energy that the target cell can utilize to stimulate its membrane or organelles. Laser radiation is absorbed through cytochromes in the mitochondria and converted into energy by the cell adenosine-5′-triphosphate (ATP), which acts in the synthesis of protein and the acceleration or stimulation of cell proliferation. However, the benefits of continuous diode lasers in wound healing are controversial. Some studies have attested to the positive effects of continuous diode laser delivery on the cutaneous wound-healing process. 11,12 In contrast, several authors have found no improvement in these processes using this technology. 13,14 Based on these contrasting results, the effects of LLLT on wound healing remain unclear.
Similar problems exist in relation to the analgesic effect of LLLT. Studies suggest that the application of low-lever lasers produces neuropharmacological effects such as the synthesis, release, and metabolism of a series of biochemical substances, including endogenous endorphins (β-endorphin); decreasing the activity of C fibers and bradykinin; and altering the pain threshold. 8 –10,15,16
In dentistry, LLLT has been used for the prevention of inflammation after surgical procedures 17,18 and periodontal surgery, 19 and to reduce pain after orthodontic treatment settings, 20 as well as for the treatment of craniomandibular disorders 21 and dentin hypersensitivity. 22 Although numerous applications exist for therapeutic lasers, their efficacy for the prevention of pain and enhancing the wound healing process is controversial. 23
The main purpose of this study was to evaluate the analgesic effect of an 830 nm diode laser applied after surgical removal of premolars, and to evaluate the effects on the wound healing process.
Methods
The study was approved by the Research Ethics Committee of the Araraquara School of Dentistry, and all patients and their respective guardians signed an informed consent to undergo the surgical treatment.
Patient selection
This randomized double-blind clinical trial study included 14 patients (8 females and 6 males) who attended the Orthodontic Clinic of Araraquara School of Dentistry between September 2010 and August 2011 for surgical removal of both contralateral maxillary and/or mandibular premolars. The subjects matched the following inclusion criteria: male or female gender, between 12 and 18 years of age, healthy, and in need of surgical removal of both first maxillary and/or first mandibular premolars, totaling two or four teeth in the same subject. Exclusion criteria included contraindications to laser therapy, systemic illness, acute local infection, risk of infective endocarditis, pregnancy, lactation, and allergy to local anesthetics or to the medication prescribed in the study.
A split-mouth model was conducted with patients acting as their own controls. A total of 20 pairs of premolars were included, totaling 40 surgical procedures. The treatment used was allocated randomly by coin flip to determine the laser therapy treatment group (n=20); the contralateral side was used as the placebo group (n=20). The operator maintained this information in confidence until the end of the analysis.
Surgical technique
The surgical procedures were performed by only one surgeon who followed the same standardized surgical technique in two sessions separated by at least 1 week because of the systemic effects of LLLT. 24 Surgery was performed with the subject under infiltrative local anesthesia, with a maximum of 1.5 cartridges of 1.8 mL of mepivacaine HCl 2% plus epinephrine 1:100,000 (Nova DFL, Jacarepaguá-RJ, Brazil). All patients required the same surgical procedure on both occasions as for all teeth, surgery involved a similar degree of difficulty, and patients were their own controls.
The medication prescribed after surgery was 600 mg of ibuprofen (Glaxo SmithKline Brasil Ltda, Rio de Janeiro-RJ, Brazil) used orally every 8 h for 4 days and 750 mg of paracetamol (Glaxo SmithKline Brasil Ltda, Rio de Janeiro-RJ, Brazil) as a rescue medication. In cases in which patients required this medication, they recorded the time of intake.
LLLT protocol
After premolar surgical removal, both the patient and the professional wore appropriate glasses according to standard safety rules to apply the LLLT protocol. The laser unit used was a gallium-aluminum-arsenide (GaAlAs) diode low-level laser with a wavelength of 830 nm (invisible red light) (Thera Lase, DMC São Carlos-SP, Brazil). This device emitted a constant wave with a mean output of 100 mW (0.1 W) in continuous mode with a spot size of 1 mm. Before the application, the surface exposed to the laser was air dried, and the laser probe was placed 1 cm from the target area at three different points. 25 –28
Each point was exposed to laser therapy for 17 sec (0.1 W×17 sec=1.7 J per site; 5.1 J at three points) and the energy density was 60 J/cm2, 28,29
On the control side, the laser unit hand piece was positioned into the mouth at the same points, but the laser was not activated. This protocol was instituted immediately and at 48 and 72 h after the surgical procedure. Hence, the participants were blinded to which treatment they received. After this procedure, the wound was sutured with 3-0 silk.
Assessments
The variables studied were degree of pain and wound healing. A horizontal 10 cm visual analogue scale (VAS) was given to each patient to assess the level of pain at the first hour, at 2, 4, 8, and 12 h after completion of the surgery, and for the next 2 days; the level ranged from 0 (without pain) to 10 (the worst pain imaginable). The quality of wound healing was recorded by clinical visual inspection and digital photographs (Canon Rebel XS, Tokyo, Japan) and analyzed by a calibrated independent examiner (K=0.76) at baseline and 2, 7, and 15 days postoperatively and was classified according validated criteria. These criteria were used to create scores and are summarized in Table 1.
An independent examiner assessed the parameters for wound healing and analyzed the VAS of all patients. This researcher, who classified the degree of tissue repair, was unaware of the type of treatment received, consistent with the design of a double-blind study.
Statistical analysis
A descriptive analysis was conducted for demographic variables. Pain and degree of wound healing were analyzed by Kruskal–Wallis and Dunn tests for a repeated measures test. The significance level was set at p<0.05 with a confidence interval of 95%. All data were analyzed using Statistical Package for the Social Sciences for Windows v14.0 (SPSS, SPSS Inc., Chicago IL) licensed from the Araraquara Dental School – UNESP. Additionally, a power analysis was performed using the program Power and Precision V4 (Biostat Inc., Englewood, NJ).
Results
Fourteen patients were enrolled in the study after satisfying inclusion criteria. Table 2 summarizes patients' genders and mean age distribution as well as the region of intervention. None of the patients showed any adverse reactions to the treatment used.
There was no statistically significant difference in analgesic effect between the groups for any evaluated periods (p>0.05). Moreover, no patients required rescue medication until the end of the analysis (Fig. 1).
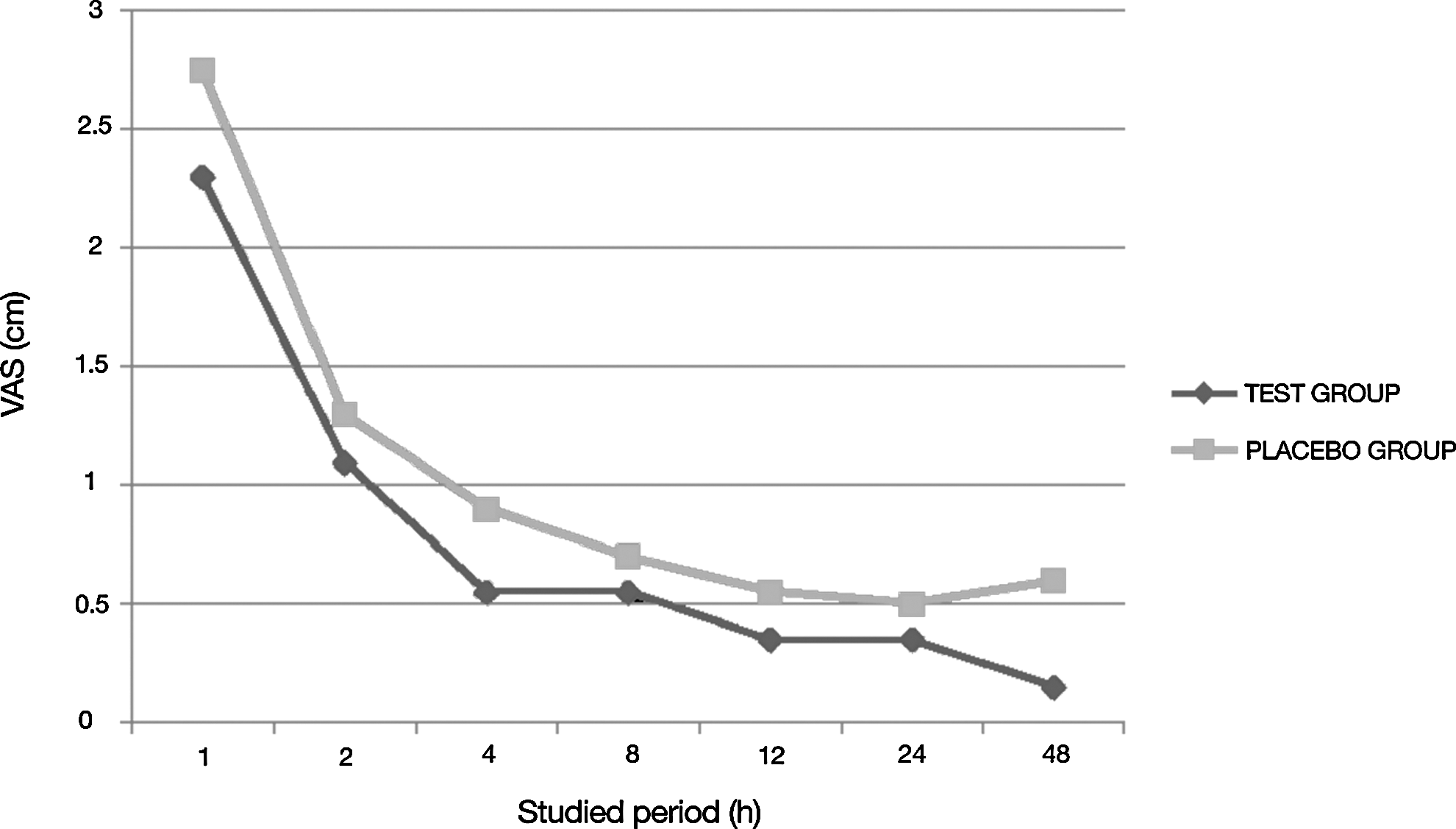
Evaluation of pain in the period studied.
The score distribution (%) of wound healing quality in each group for each analyzed period is summarized in Table 3. The experienced examiner performed his clinical analysis at the time of each visit with support from digital photographs reaching a κ index of 0.76. Moreover, the power test analysis revealed a power of 81%.
Discussion
Nowadays, access to laser devices is easier than it was decades ago, and the costs of laser therapy have become increasingly affordable. However, several studies on the use of LLLT have shown questionable outcomes. 13,24,30,31
The use of LLLT depends upon the adjustment of variables such as the type of laser, wavelength, output power, time and mode of application, and distance of source from irradiated tissue; this makes it difficult to draw meaningful comparisons. 14,18,24,30,31
In the present investigation, the use of LLLT with the intention of decreasing postoperative pain and accelerating tissue repair after premolar extraction achieved no statistically significant differences between the laser application and the control groups. The study was designed to investigate a specific group of teeth (premolars) and a specific age group of individuals (adolescents), which is a new approach. Therefore, comparison with other studies is a difficult task; however, our results, regarding the lack of benefit for healing postoperative symptoms, are in agreement with those of previous investigations. 14,18,24,30 –32
A study 30 used a sample of 17 patients to investigate the effects of soft laser (He-Ne) on postoperative swelling and pain after lower third molar (LTM) extraction. In this study, the tested side was treated for 2 min with a power output of 8 mW in pulsed mode (50 pulses per second). No statistically significant differences were found in pain levels and swelling between the two sides. In a clinical trial (double-blind crossover study), 24 the authors used a laser (830 nm; 6 J at 40 mW of power) to verify postoperative swelling, trismus, and pain after LTM extraction surgery. These authors concluded that in reference to the parameters investigated, there was no evidence that the application of soft laser had any beneficial effects. Another approach used 14 a laser with the same wavelength (830 nm); however, these authors used a different power output (30 mW), time of irradiation (132 sec), and dose (4 J). They reported pain and swelling levels at 24 and 72 h and on the 7th day, in addition to information on wound healing; they found no differences between groups at 72 h with respect to wound healing. Additionally, a statistically significant reduction was not found in postoperative pain at all evaluated periods (24, 48, and 72 h) using a He-Ne laser. 33 In all of these studies, the use of LLLT did not result in positive effects on postoperative symptoms. In addition, the lack of uniform reporting of physical and biological variables hampers the standardization of results. Furthermore, studies on the use of LLLT in the management of postoperative symptoms have used different methodologies, and some variables are not fully described in the texts.
A clinical study 32 used two groups who underwent extraction of an LTM, one of which was a test group who received treatment with a laser diode with 810 nm of wavelength and 11 J/cm2 of energy density at the surgical site. Analysis of the level and duration of pain showed a statistically significant difference between the experimental and control groups, in contrast to the findings of the present study. Similar results were obtained by a previous report 17 which used a diode laser (gallium-aluminum-arsenic) with a wavelength of 637 nm (visible red light), 50 mW with 4 J/cm2 of energy density for 10 min at the surgical site in 30 patients after LTM extraction. This group was compared with another two groups (the second group received diclofenac 100 mg preoperatively, and the third group received regular postoperative recommendations). The results showed that the use of low-power laser irradiation provided the best postoperative analgesic effect and the most comfortable postoperative course after the surgical procedure. In a randomized double-blind study 31 a He:Ne laser (633 nm) was used at a dose of 10 J/cm2 and the results showed that the amount of trismus was significantly less in the laser group than in the placebo group up to 7 days after surgery.
It is important to note that the results of these studies are varied and inconclusive because of the difference in sample sizes or applied protocols (for example, the type of laser and time of irradiation); therefore, it is impractical to define an optimum therapeutic dose or evaluate the procedure's clinical effectiveness.
Classification of pain intensity is a difficult task, as this variable is a subjective quality and can vary among patients. Therefore, the split-mouth design of our study was able to avoid, in part, a bias in information collection. It is important to point out that the pain evaluation was only performed during the first 48 h after the surgical procedure, as the patients reported no painful sensation after this period. Therefore, the third laser application at the 72nd hour after the premolar extraction did not contribute to pain relief. Our study was conducted on premolars with a similar degree of surgical difficulty, so that patients were their own controls following a split mouth model. It is an interesting approach used by current studies concerning this analysis. This approach provides the best possible control group, because both treatments were given to the same patient, with the same surgical procedure, in identical microbiologic conditions, and by the same surgeon. 28,34 Gender distribution between groups was monitored because the pain thresholds differ between both genders (Table 2). Furthermore, a single surgeon and one experienced clinician performed this investigation in order to avoid differences among different surgeons' skills and to conform to the requirements of a clinical trial study.
The sample size is an important feature in clinical studies. In our investigation 14 patients of both genders were enrolled (40 surgical procedures), who were allocated randomly to each group. It can be supposed that the number of participants in this study may be insufficient to show any statistical differences. Despite the fact that the number of patients seems to be relatively inappropriate for making a clinical decision, the number of procedures allocated in the studied groups is in agreement of previous clinical studies. 25,26,28,34,35 Table 4 summarizes the current results in the literature concerning laser therapy application as well as the sample size used, and some important parameters.
RCT, randomized clinical trial; LTM, lower third molar.
In relation to laser parameters, success in obtaining good results is dependent upon many variables. In the present investigation, the LLLT application protocol resulted in no beneficial effects. Therefore, studies with different laser application parameters must be performed to clarify the applicability of LLLT following surgical procedures.
Conclusions
These findings show that the application of intraoral LLLT with an 830 nm diode laser with the specific parameters used in this study does not reduce pain or accelerate the wound healing process after surgical removal of premolars in adolescents.
Footnotes
Author Disclosure Statement
No competing financial interests exist.