
Abstract
Introduction
Studies of laser-induced effects on nerves in animals have provided further insight into the analgesic effects of LI. In these studies, LI selectively blocked conduction in small diameter Aδ and C nociceptors in response to noxious stimuli. 14 –18 Further supporting such neural blockade is a dental clinical trial using low-level pulsed Nd:YAG laser at nonablative doses, which established a direct correlation between conduction block in the pulpodental nerve and analgesia. 19 Moreover the analgesia was equivalent to the topical anesthetic agent, EMLA.
Recently, we demonstrated that both 120 sec of transcutaneous 650 and 808 nm LI, applied transcutaneously and sequentially to four points overlying the course of rat sciatic nerve, blocked both somatosensory evoked potentials (SSEPs) and compound muscle action potentials (CMAPs). 20 In the current study we further dissect the effects of LI on nerve conduction in relation to the distribution of the total energy, at doses used clinically, and compare transcutaneous 650 nm, continuous wave (cw, 35 mW) or 808 nm (cw, 450 mW) LI to a single point with effects at four points. We also discuss the clinical implications of our findings for LLLT and LA.
Materials and Methods
All procedures were conducted in accordance with protocols approved by the Animal Ethics Committee of the University of Sydney, Australia #K00/4-2009/2/5033. Outbred Sprague Dawley (SD) rats, 10–12 weeks of age, were used for all experiments and were anesthetized with 2% isoflurane at each time point for each experimental procedure. Electrophysiological assessment of baseline SSEPs and CMAPs was determined for all rats prior to any experimental procedures, and to detect animals with abnormal conduction. No animals were identified for exclusion.
Experimental design
Forty rats were randomly assigned into 650 or 808 nm LI studies. The rats in each laser group were further assigned for 30 sec (n=10) or 120 sec LI (n=10) and each of these groups further assigned for SSEPs (n=4) or CMAPs (n=6) (Fig. 1).
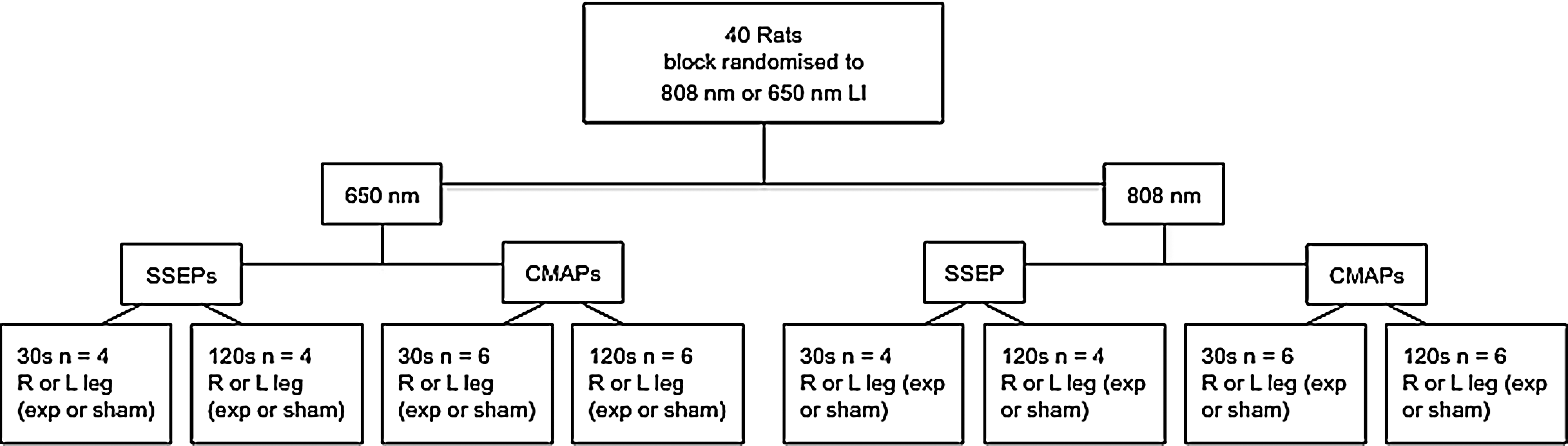
Experimental design.
One hind leg of all rats in all groups was randomly assigned as experimental LI and the contralateral leg assigned as control sham LI, delivered as for the experimental leg but with the laser switched to the “off” position.
Laser parameters and LI delivery
The power outputs of the 650 and 808 nm laser probes (Irradia™, Sweden) were 35 mW (Power Density [PD]=∼600 mW/cm2) and 450 mW (PD=∼7.5W/cm2), respectively, as measured by the Australian National Institute of Measurement. The output power of each laser was again checked before each irradiation via the inbuilt optical power meter (Table 1).
LI (650 or 808 nm) was delivered transcutaneously for 30 or 120 sec per point with the laser probe in firm contact on the skin to a single point over the midpoint of the course of the sciatic nerve based on other studies by our group. The midpoint was selected because it corresponds to an acupuncture point on the bladder meridian and its location in comparison with the four points in our previous study is shown (Fig. 2).

Location of laser irradiation (LI) application over sciatic nerve at
Electrophysiological recordings
All studies were performed at room temperature using a Neuromax (XLTEK, Ontario, Canada). All stimuli in all experiments were supramaximal and the responses recorded at 10 min, 20 min, 24 h, and 48 h post-LI or sham LI. Amplitude was measured from baseline to the peak of the waveform. Latency was defined as the time from stimulation to the initiation of the waveform and, as a general rule, is inversely proportional to conduction velocity.
SSEPs
The stimulating needle electrode was inserted at the ankle with the recording electrode placed between the spinous processes of T13 and L1 (Fig. 2a). Two averaged traces, of at least 20 responses, were recorded from each leg of all rats in all groups.
CMAPs
Paired stimulating needle electrodes were inserted at the sciatic notch (hip; proximal to LI) and the ankle (distal to LI delivery) (Fig. 2b) and electrophysiological responses recorded from the dorsal foot muscles. The difference between the proximal and distal (P-D) latencies in LI and sham LI groups was compared, a standard measurement of nerve conduction. Amplitude was measured from both proximal and distal peaks and expressed as a ratio (H/A).
Statistical analysis
Data are expressed as means±SEM. Changes in latency and amplitude of SSEPs and H/A ratios of CMAPs were analyzed by Student's t test. All data were analyzed with GraphPad Prism (Version 5) and significance was set at a p value of <0.05.
Results
Effects of 808 nm LI
LI (120 sec) to a single point increased SSEP amplitude by 17.5% at 10 min, returned to baseline by 20 min, and remained unchanged at 24 and 48 h (Fig. 3). LI (808 nm) for 30 sec did not alter latencies or amplitudes of SSEPS or CMAPs, (data not shown), from baseline at any time point. All sham LI conduction remained at baseline values.
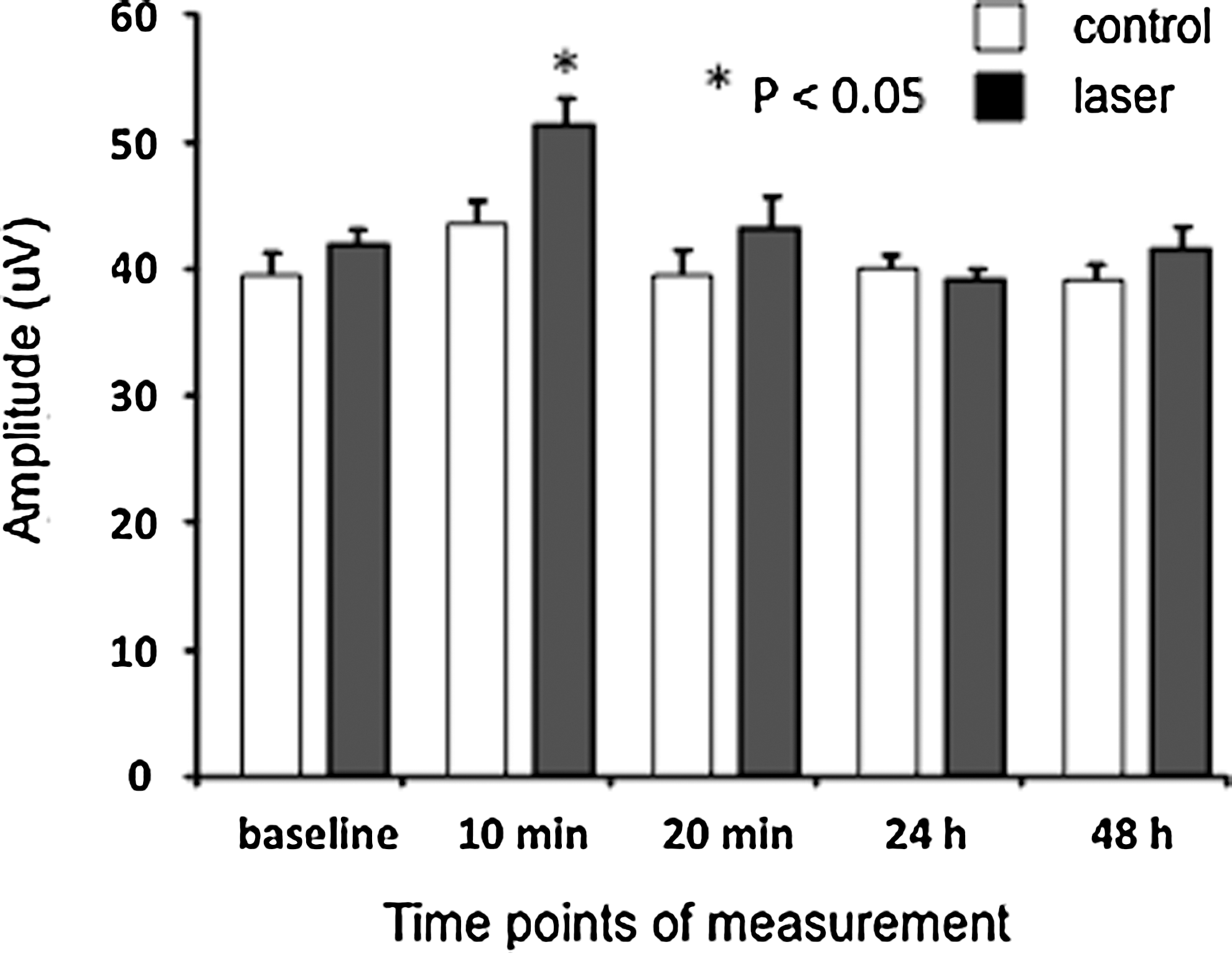
Amplitude of somatosensory evoked potentials (SSEPs) following 120 sec 808 nm laser irradiation (LI) to a single point overlying rat sciatic nerve.
Effects of 650 nm LI
LI (650 nm) for 30 or 120 sec to a single point did not alter latency or amplitudes of SSEPs or CMAPs (data not shown).
Discussion
Our study demonstrated that transcutaneous 808 nm LI delivered to a single point for 120 sec (54 J, 18 J/cm2) increased SSEP amplitudes at 10 min with return to baseline by 20 min. There was no change in SSEPs or CMAPs with 30 sec or 120 sec 808 nm LI at any time point other than 10 min. This finding contrasts with our previous study in which the same total energy, delivered sequentially to four separate points for 30 sec per point caused statistically significant conduction block of SSEP and CMAP amplitudes and latencies. 20 LI (650 nm) for 30 or 120 sec caused no change in SSEPs or CMAPs at any time point, whereas we reported significant conduction block in our four point LI study. Our two studies are the first to compare how the same total laser energy affects nerve conduction when delivered at single or multiple points.
Although our recent review shows that LI is largely inhibitory, 21 two earlier studies have reported increased CAP amplitudes following transcutaneous 632.8 nm (HeNe), 8 mW, cw, LI to a single point overlying rat sciatic nerve. These studies applied LI continuously for 30 min. 22,23 The increase in CAP amplitudes occurred 7 min after delivery of ∼7 J, which gradually returned to baseline and then decreased to below normal at 30 min. In contrast, the visible wavelength 650 nm (InGaAlP) 35 mW, cw in our study, for 30 sec (1.1 J) or 120 sec (13.5 J), caused no change in CAP, although the total energy delivered in 2 min is greater than that reported by Rochkind and Nissan over the same time. 22,23 The difference between our study and theirs may be the result of the longer duration of LI or different wavelength characteristics, such as greater coherence with HeNe resulting in greater photon penetration, 24 or other laser parameters as yet undefined for InGaAlP diode. The increased amplitude with our IR 808 nm LI, could, in contrast, be the result of the higher total energy delivered of 54 J. These considerations are important, as our review highlighted the inconsistent and patchy reporting of laser parameters in the majority of studies. 21
Increased CAP amplitudes have also been reported after LI to exposed nerves in vitro. HeNe (632.8 nm), 5.5 mW, 350 mW/cm2 to cervical sympathetic ganglia increased intracellular axonal amplitudes and caused hyperpolarization, increasing the resting membrane potential. 25 Paradoxically, when Shimoyama et al. recorded CAP amplitudes extracellularly they were reduced. They explained this paradox as being the result of hyperpolarization of some axons, so that fewer axons were responsive to the supramaximal stimulus. Therefore, the overall effect was reduced amplitude. As these nerves are autonomic, it is difficult to compare with our findings with the sciatic nerve composed of both sensory and motor fibers. However, it is possible that our increased SSEP amplitudes after 120 sec LI could be the result of synchronization, that is, some fibers become hyperpolarized with an increased activation threshold, which when activated summate to cause increased amplitudes. 26,27
Although beyond the scope of our electrophysiological experiments, we found that 808 nm LI in cultured neurons significantly reduced ATP via decreased mitochondrial membrane potentials. 28 which would downregulate Na+K+ATPase activity, the major Na+/K+ channel for maintaining the resting potential of the axon. 29 Kudoh et al. found that Na+K+ATPase activity increased following “low” dose 830 nm, 60 mW, 0.36–0.9J, cw LI to rat saphenous nerve, whereas “high” dose, 1.8–7.2J, decreased activity. These findings are consistent with the biphasic effect of hyperpolarization followed by depolarization, which we propose underpins the findings of our electrophysiological studies.
Our study also has direct relevance to the different clinical applications of LLLT and LA. 12,30,31 In LA many acupuncture points (APs) overlie peripheral nerves such as pericardium 6 (PC 6) overlying the median nerve, used for treating carpal tunnel syndrome. 32 Other acupuncture points overlie nerves emerging from foramina, for example, stomach 2 (ST 2) over the infraorbital nerve or where nerves emerge between fascial planes, for example gallbladder 20 (GB 20) or bladder 10 (BL 10) overlying the occipital nerve at the base of the skull, and used to treat headache and neck pain. 11 The increase in SSEP amplitude following 120 sec, 808 nm is consistent with acupuncture puncture point “stimulation,” which would also occur in the epidermal peripheral nerve endings of Aδ and C fibers in the dermis, which also mediate needle acupuncture effects. 33
In contrast to LA, in LLLT laser irradiation is applied to multiple tender points at sites of pathology, such as around joint lines directed to synovium, or at entheses or muscle bellies such as in treatment of knee osteoarthritis. 34 LLLT for chronic musculoskeletal pain does not specifically target the course of an underlying nerve, however, the dense epidermal neural network of unmyelinated and thinly myelinated Aδ and C fibers 35,36 will receive the maximum number of photons. We therefore propose that conduction block would occur a priori in these nerve endings as well as in the underlying nerve trunk, which receives only 3–10% of transmitted photons. 23 This clearly demonstrates the relevance of multiple point LI for pain relief as demonstrated in clinical trials of, for example, neck pain, 37 knee osteoarthritis, 38 and lateral epicondylitis. 39
Our findings are also relevant for the treatment of neuralgias including carpal tunnel syndrome, for which LLLT reduces symptoms when applied at several points over the wrist. 5 Other neuropathic pain conditions such as trigeminal neuralgia, 10 which has been successfully treated by LLLT (830 nm) applied to the face, 10 and post-herpetic neuralgia, in which the affected dermatome is treated. 6 –8
We suggest that for the maximum inhibitory effect on pain fibers, LI should be applied over an area of pathology, treating tender points in the related dermatome, myotome and sclerotome. This method would support the use of laser cluster heads for LLLT, rather than single laser diodes, to achieve more efficient coverage of an area of pathology. For laser acupuncture, application at a single acupuncture point can result in the generation of an action potential in the epidermal neural network and in underlying nerves, initiating a pain-modulating response in cortical centers. 40
Conclusions
The important finding from this and our previous study is that the area over which LI is delivered is a variable with significantly different electrophysiological effects, which we consider is a critical parameter in neural response. Our finding of increased sensory nerve amplitudes with localized high dose LI to a single point in contrast to conduction block with multiple point LI supports a neural hypothesis for laser acupuncture and the clinical use of LI to multiple points in LLLT for maximum analgesia. Further research to define optimal laser parameters for neural inhibition and stimulation would strengthen current evidence-based protocols for relief of pain, a worldwide and enormously costly burden.
Footnotes
Acknowledgments
This work is funded by the National Health and Medical Research Council of Australia, Grant #512678.
Author Disclosure Statement
No competing financial interests exist.