
Abstract
Introduction
A cavity prepared with bur has a smooth, enamel, and dentin surface 9 covered by a smear layer 0.5–2 μm thick. 7 This layer is composed of the freshly cut tooth structure. To ensure good adhesion, the dentinal surface is conditioned by acid etching to dissolve this layer, which could occlude dentinal tubules and which is sometimes incorporated into the bonding of the restorations. 10 The acid effect creates a clean dentinal surface without any smear layer, and exposes collagen for adequate bonding. 11 The principle of dentine adhesion is based on micromechanical retention. Penetration of the resin monomers into the exposed collagen network to a depth of 3–10 μm, creates a hybrid layer 12 –15 on the demineralized superficial dentinal surface. This hybrid layer, neither resin nor tooth, also known as resin–dentin interdiffusion zone, appears to be key for the improvement of the bonding between the resin composite and dentin. 16 –18
However, there is always a leakage in the dentin–resin interface, 19 which may be the result of a hydrolytic degradation of the exposed collagen network and a poor infiltration of monomers into this collagen.
Pioch et al. 20 showed that the use of sodium hypochlorite (NaOCl) decreased the leakage levels. NaOCl, a nonspecific proteolytic agent, which is efficient against pathogenic organisms, is widely used in endodontic preparations of root canals. 21 It is used at concentrations varying from 0.5% to 5.25%. At low concentrations, it mainly dissolves necrotic tissue, whereas at higher concentrations, organic dissolution is more significant; however, it also dissolves vital tissue, which is generally an undesirable effect. NaOCl is a strong oxidizing agent that effectively removes organic components, 22 such as collagen fibers. In addition, treatments with NaOCl solution have been evaluated for their effects on dentinal bonding procedures. 12 Other studies have pointed out that the analysis of the resin–dentin interface samples deproteinized with NaOCl showed an absence of the hybrid layer. 12,23
According to the literature, 24,25 the application of Er:YAG laser generates a thermally affected layer on the irradiated dentinal surface. This thermal layer could be composed mainly of denatured collagen fibers, which may decrease the quality of bonding of the irradiated dentin, especially in intertubular dentinal areas. This thermally affected layer might induce the microleakage observed in the scanning electronic microscopy (SEM) studies of irradiated cavities, in contrast to the lack of leaking in the cavities prepared only with bur. Only a few studies discuss the effects of Er:YAG laser on the organic components of dentin, especially collagen fibers, which are instrumental in the bonding process of resin materials.
The aims of this in vitro study were to evaluate: (1) the influence of 5% NaOCl application on Er:YAG irradiated dentin; and (2) its effect on the quality of adaptation of the composite restoration margins.
Materials and Methods
Dentin preparation
Forty-nine caries-free and freshly extracted adult molars were cleaned using a scaler and stored in distilled water at 4°C. In order to expose the dentin, crowns were transversally sectioned at high speed with a diamond disc (943 CH 205 080 GEBR Brasseler, Lemgo, Germany) under running water. Dentinal surfaces were then polished using Soft-Lex discs (3M ESPE, St Paul, MN). Four standardized cavities were prepared in each dentinal surface using a high-speed handpiece (KaVo, Germany) under air/water spray. Cavities were prepared using standard 1.7 mm diameter and 2 mm length diamond burs (Hager & Meisinger GmbH 828G017, Germany). The bur stop system allows control of the drilling depth.
A cylindrical diamond bur was used to set a marking guide on the enamel distal side of each tooth. A second mark was also made on the enamel part in front of the control cavity. All cavities were prepared and treated by the same operator. We randomly selected 43 teeth to be used for microleakage studies and 6 others for SEM analysis.
Dentinal surface treatments
Only two cavities in each tooth were irradiated with the Er:YAG laser system (Fidelis plus III, Fotona, Slovenia) at an approximate irradiation speed of 1 mm/sec and under a spray of air (20 mL/min) /water (20 mL/min).
The irradiation parameters used in this in vitro study were as follows: pulse: variable square pulse (VSP) mode (100 μsec), 150 mJ, and 10 Hz. We used a mirror handpiece (R02). The diameter of the laser beam was 0.9 mm at a focal distance of±7 mm. The irradiation distance was standardized using a system allowing fixation of the handpiece in order to maintain an approximate working distance of 7 mm. Only the tooth was allowed to move (Fig. 1). The complete irradiation of the dentinal cavity was done in one passage, with overlaps between irradiated areas that were controlled and appreciated by the operator, with possible human error.

Schematic view of the system allowing irradiation of dentin with an approximate constant irradiation distance. Arrows show the possible movements of the tooth. Tooth can move in all directions except the vertical one.
Two out of the four cavities, one irradiated and one nonirradiated, were treated with a 5% NaOCl solution for 30 sec and rinsed with distilled water for 30 sec.
This solution was prepared the same day as the experiments in order to avoid any loss of chloride activity.
Bonding procedures
All cavities were etched with 35% phosphoric acid (3M ESPE Dental Products, St. Paul, MN) and rinsed with running water for 10 sec. Soft drying was performed with air flow, to keep the dentin slightly moist.
Two applications of bonding agent (Scotchbond: 3M ESPE Dental Products, St. Paul, MN) were done on all cavities for 15 sec using a fully saturated specific brush tip for each coat. The bonding agent was gently air-dried with an air syringe for 5 sec and photocured for 20 sec using a light-emitting diode (LED) (Translux Power Blue: Heraeus-Kulzer, Germany: wavelength : 400–480 nm, 1000 mW/cm2).
A restorative resin composite, (Ceram-X nanoceramic restorative, Dentsply, USA) was placed in every cavity using a transparent matrix strip (Kerr Hawe Stopstrip, Switzerland) and photopolymerized using an LED-curing light source for 20 sec. The light intensity of the LED was periodically measured (it ranged between 800 and 1000 mW/cm2).
Thermocycling
All surfaces of filled cavities were polished by means of Soft-Lex Pop-on discs (medium, 3M ESPE, St Paul, MN) under cold water in order to remove the potential excess of resin composites overhanging the border of cavities. All teeth of all groups were thermocycled for 1000 cycles, for 24 h, from 5°C to 55°C (Willytec Thermocycler V 2.9).
Other treatments
The teeth were covered with two layers of transparent marine varnish, leaving a 1 mm border around the edge of each cavity to protect the rest of the tooth from the dye solution. Then the samples, except the resin composite-filled surfaces, were embedded in acrylic resin (GC Unifast Trad, Japan). Subsequently, all specimens were immersed in an aqueous solution of 0.5% methylene blue for 90 min at 37°C. Finally, these specimens were brushed under tap water for 20 sec.
Cavities filled with resin composite were completely covered by the acrylic resin. Thereafter, all the teeth were sectioned longitudinally in a labial-lingual direction through the center of both cavities using a water-cooled diamond saw (Leica 1600, Leica Microsystems). On average,±3 mm thick slices were collected from each cavity. The penetration of dye was measured in millimeters using the Visilog 5.3 analysis software (Noesis Vision, St. Laurent, PQ, Canada). For each cavity, the deepest penetration of the dye was recorded. The ratio of infiltration (depth of dye penetration from the occlusal surface/total length of interface) into the resin composite–dentin interface was measured. The penetration scores for all slices per specimen were compared. A third party other than the operator, who performed the treatment and the restorations, observed the specimens and recorded the results.
Statistical analysis
The mean values and standard deviations of the microleakage percentage in each group were calculated and analyzed using Kolmogorov and Smirnov for normality test and Tukey–Kramer multiple comparisons test (p<0.05).
SEM study
Six teeth were used for SEM observations. Samples were subjected to the same cavity-preparation method. In the first group, (four teeth) cavities were etched; whereas no etching was performed in the second group (two teeth).
Dentinal surfaces were prepared for SEM examination using the following procedure: ∂ Rinsing in two concentrations of ethanol (70% and 100%) ∂ Air-drying and mounting on stubs with Tempfix resin ∂ Coating with Pt by sputtering in a Balzers SCD-030 sputtering unit for 2 min on 30 mm thick samples at 30 mA ∂ Examining with a scanning electron microscope (JSM 840A electron microscope, JEOL, Japan) at an accelerating voltage of 20 kV
Samples were observed under a scanning electron microscope (JSM-840, JEOL, Japan) at 1000× and 5000× magnifications.
Results
Microleakage tests
Mean values and standard deviations of dye penetration (%) in the different groups were as follows: 46.43±8.571 for group B (cavities prepared with a bur), 58.33±6.821 for group BCl (cavities prepared with a bur and pretreated with a 5% NaOCl before acid etching), 39.09±5.871 for group LCl (cavities irradiated with Er:YAG laser and pretreated with a 5% NaOCl before acid etching), and 47.27±5.017 for group L (cavities irradiated with Er:YAG laser).
Every group showed microleakage, irrespective of the conditioning method applied (Fig. 2).
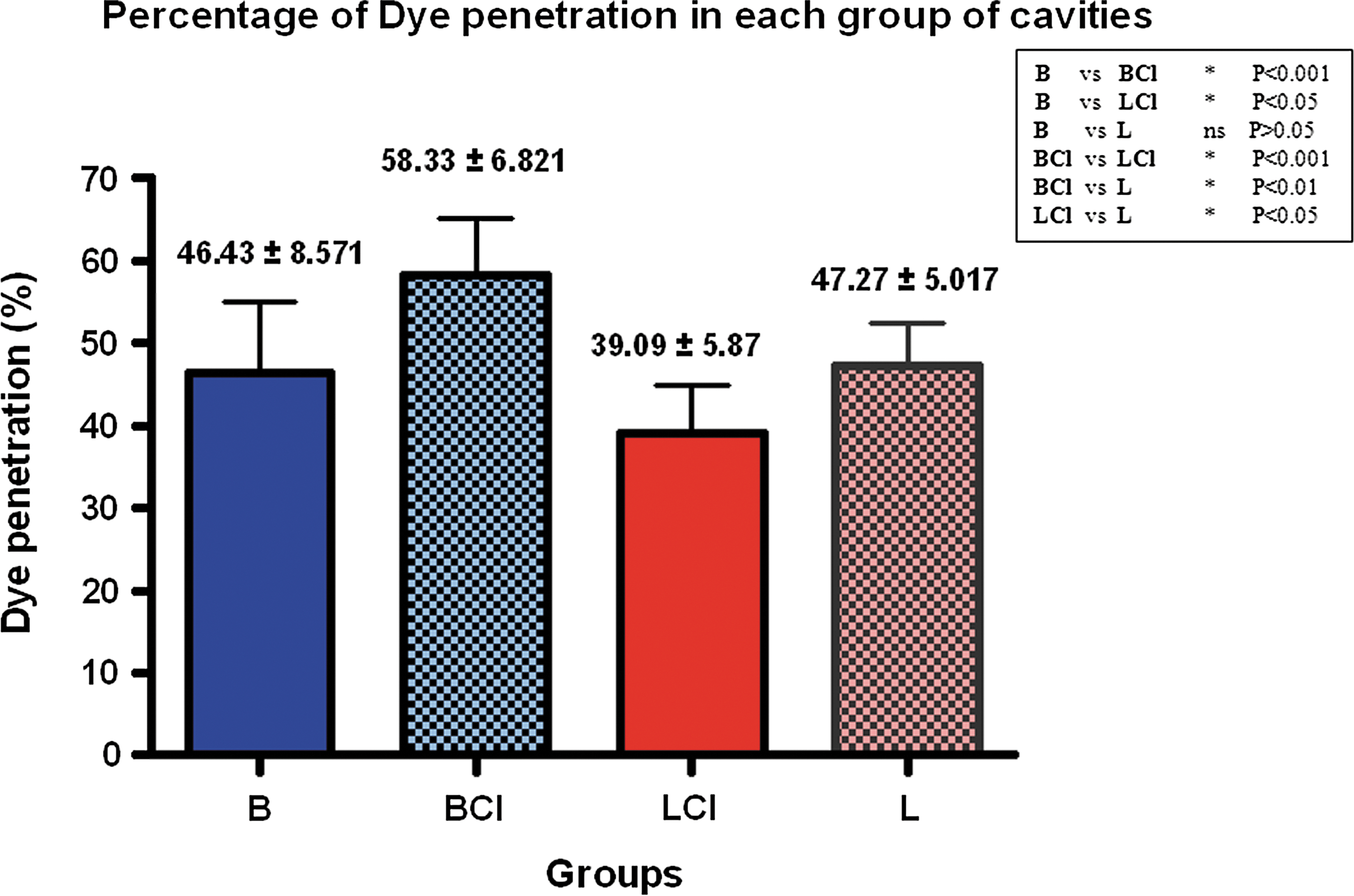
Graph representing the mean values and standard deviations of dye penetration (%) in the dentinal cavities subjected to different treatments. A 0.5% methylene blue solution was used for the microleakage test.
All groups passed the normality test, using the Kolmogorov and Smirnov method. Statistically, Tukey–Kramer Honestly Significant Difference (HSD) test showed that there was a significant difference in the dye infiltration rate between the cavities of groups LCl and L (without NaOCl treatment), the cavities of groups LCl and BCl
SEM results
Dentinal surface prepared with bur and treated with NaOCl (5%) and phosphoric acid (35%) showed a clean and smooth surface with fully opened tubules; the smear layer was totally eliminated. Acid etching mostly removed the peritubular inorganic material and greatly enlarged the tubules (Figs. 3A and 4A).
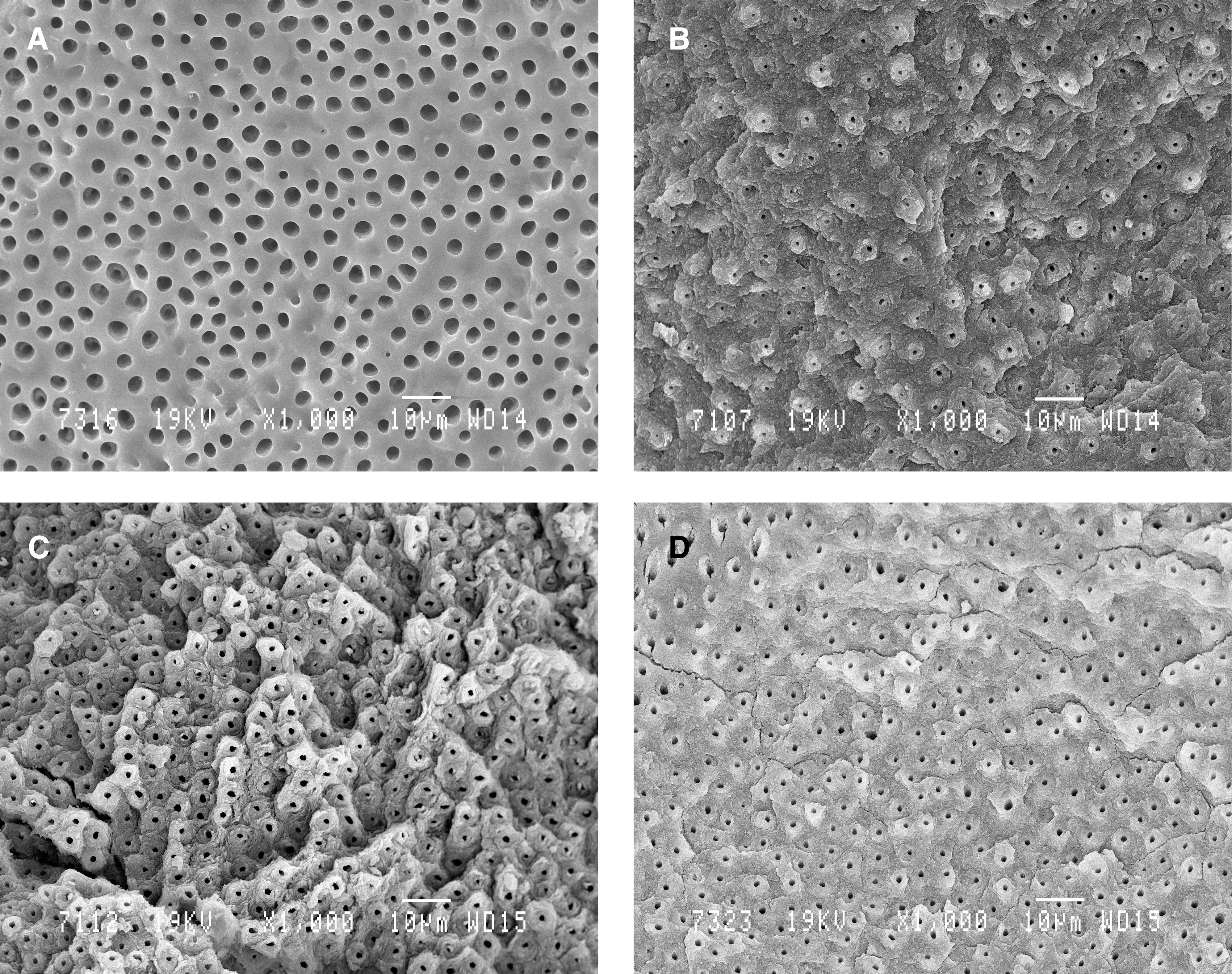
Representative scanning electron microphotography (SEM) images of dentinal surfaces (original magnification ×1000).
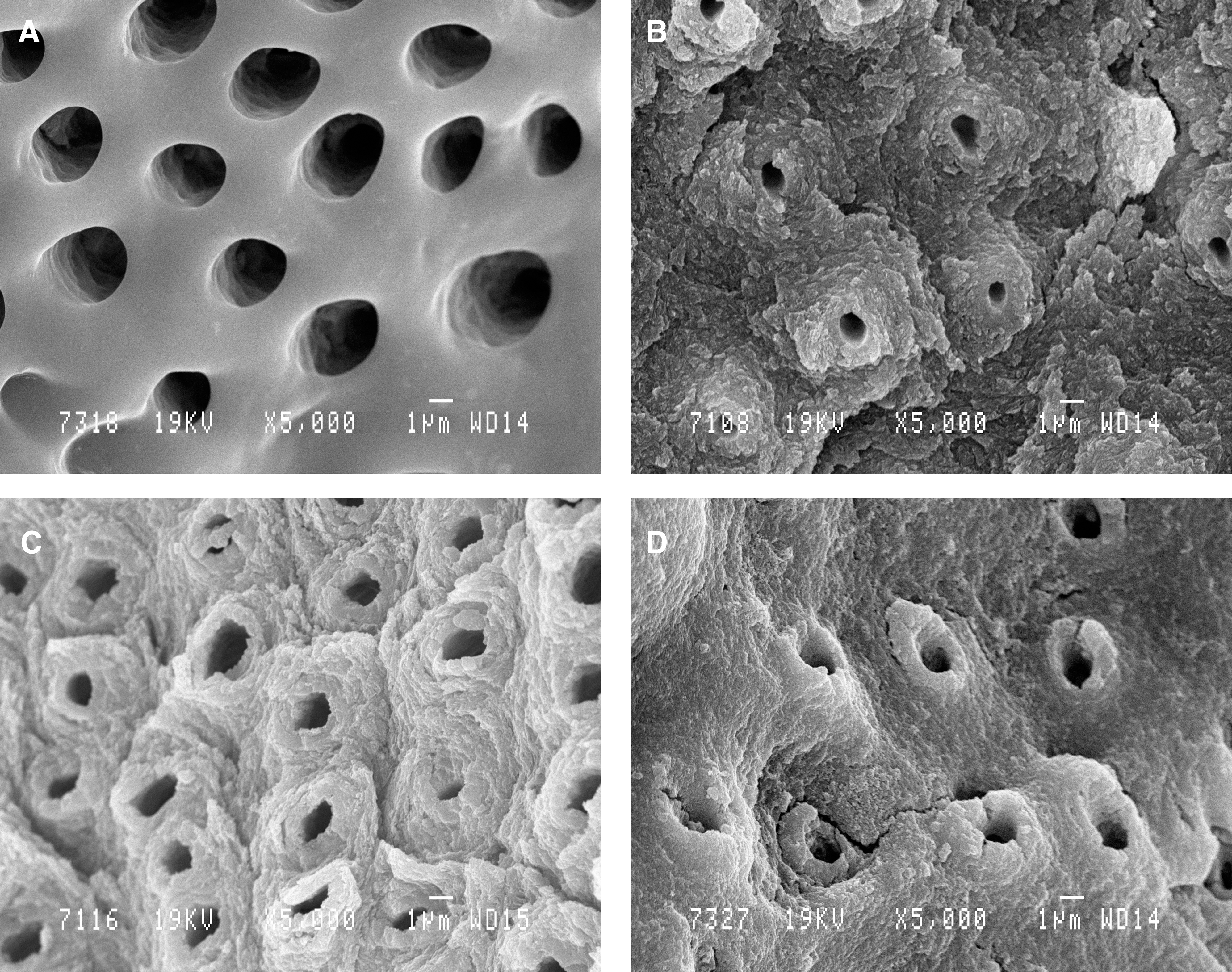
Representative scanning electron microphotography (SEM) images of dentinal surfaces (original magnification ×5000).
In contrast, the dentinal surfaces irradiated by Er:YAG laser showed a highly irregular and flaky surface, free of the smear layer. The dentinal tubules were open. Intertubular dentin, richer in water than the peritubular dentin, was easily eliminated (Figs. 3B and 4B). These microscopic observations corroborated previous studies' findings.
The SEM microphotographs of irradiated dentin surfaces pretreated with 5% NaOCl showed more obvious peritubular areas that were intact and more circular tubule orifices. The mineral components of the dentinal surfaces were exposed (Figs. 3C and 4C).
The SEM microphotographs of dentinal surfaces irradiated by Er:YAG laser, treated with 5% NaOCl for 30 sec, and then etched with 35% phosphoric acid for 15 sec, showed a smoother and less rough surface (Fig. 3D). The tubules remained open and were prominent (Fig. 4D).
Discussion
The quality of bond strength in Er:YAG laser-irradiated dentin has been extensively investigated. 24,26,27 Previous studies have reported that cavities prepared by Er:YAG laser, non-etched, and filled with resin composite, show a lower dentin bond strength 28 –30 than do cavities prepared conventionally and filled with the same material. The Er:YAG laser creates a laser-modified layer that adversely affects the dentin; consequently, it does not constitute an alternative bonding strategy to conventional acid etching. The formation of a hybrid layer and resin tags seems to be essential to the establishment of a strong resin–dentin bond. In order to achieve this, the complete removal of the smear layer and the demineralization of intertubular and peritubular dentin are necessary. This results in an exposed collagen matrix, which is subsequently infiltrated by resin that polymerizes in situ. Bertrand et al. 7 showed that the acid etching application prior to the bonding process allowed hybrid layer formation. In our study, we used acid etching in order to obtain this hybrid layer.
At present, the effect of Er:YAG laser on organic components, such as collagen fibers, remains unclear. Nevertheless, Soares et al. 10 have shown, using spectroscopy, that the laser treatment affected the organic substance. Furthermore, Ceballos et al. 24 have shown a 3–5 μm thick laser-modified layer, an alteration of the dentin subsurface, beneath which collagen fibrils appear to have lost cross-banding and are fused together, thereby eliminating interfibrillar spaces. At present, no treatment can eliminate this affected layer. However, according to the literature, 31,32 the application of NaOCl solution, used as a deproteinizer on the dentinal surface, eliminates organic material and part of the smear layer, but it does not entirely open the tubules. NaOCl disrupts the pyridinoline cross-links that occur in collagen I and II, 33 with the formation of chloramines and protein-derived radical intermediates. 34 Nevertheless, it appears that NaOCl does not affect inorganic substances. On the contrary, other studies have shown that NaOCl treatment at different concentrations and reaction times can achieve complete removal of collagen fibers. 35 –37 NaOCl, at a concentration of 5%, was used in some studies 38,39 in which the authors obtained elimination of the organic substance, without alteration of mechanical properties; in contrast, high concentrations such as 10% 40,41 were used in studies, which reported an increase in microleakage. For all these reasons, a concentration of 5% NaOCl was chosen, the concentration mainly used in endodontic treatment. NaOCl solution was applied for 30 sec to assure a high degree of elimination of the denatured and thermally affected layer created by laser irradiation.
In the present study, the application of 5% NaOCl solution for 30 sec to the irradiated group (LCl) before acid etching showed a statistically significant reduction in the percentage of microleakage compared with the irradiated group without NaOCl pretreatment (L) (Fig. 2). In parallel, SEM analysis showed that the irradiated surface pretreated with 5% NaOCl induced a dentinal surface with obvious tubules (Figs. 3C and 4C). An affected layer was described by Soares et al., 10 who noticed it after using the same energy density used in this study. Therefore, organic components, such as collagen fibers, could also be eliminated by NaOCl treatment. This suggestion may be logical because 90% of the organic component in dentin is collagen, which is almost exclusively Type I. 42 Therefore, application of 5% NaOCl, followed by treatment with 35% phosphoric acid, induced a superficial removal of organic and mineral tissues, leaving a polished dentinal surface (Fig. 3C) with largely open tubules (Fig. 4C).
In addition, when we pretreated bur-prepared cavities with NaOCl solution and then etched them with phosphoric acid, the SEM observations showed a very clean and smooth surface with more completely opened tubules (Fig. 4A). At this same concentration, Mountouris et al. 43 have also observed the removal of the smear layer, opening of dentinal tubules, and appearance of a smooth intertubular surface without any alteration of carbonates and phosphates.
Moreover, a significant increase in microleakage was observed when we used NaOCl pretreatment in bur-prepared cavities (BCl group) (Fig. 2). This effect may be the result of the proteolytic effect of NaOCl, which disrupts the quality of the exposed collagen fibers. This observation has been confirmed by Perdigao et al. 37 It is important to note that deproteinization alone does not open the tubules, 44 because NaOCl does not affect the mineral component. Acid etching alone does not completely open the tubules because they remain filled with organic components. Marshall et al. 35 found out that the association of dentinal etching and deproteinization led to the appearance of porous microstructures, because of the removal of minerals and organic components. Therefore, the irradiated cavities were rinsed with distilled water before the bonding protocol. Only a part of the cavities received the application of NaOCl solution. In this study, we ruled out a simple water rinsing effect. We did not observe a difference in microleakage percentage between the groups of cavities prepared conventionally (B) and treated by laser (L). Bertrand et al. 45 reported similar results.
In summary, organic contents, such as thermally affected collagen, are eliminated from irradiated dentinal surfaces by treating them with NaOCl solution. The dissolution of mineral components by the acid etching process may increase the appearance of a smooth surface. The possibility of using NaOCl as pretreatment to improve the bonding quality would be an interesting approach. The capacity of deproteinization should be optimized to allow the introduction of a new treatment for irradiated dentin surface.
The application of 5% NaOCl solution before etching promoted a reduction of microleakage, because our protocol is different from other studies.
Further investigations and studies should be undertaken in the future in order to improve our knowledge about the effect of NaOCl on Er:YAG laser-irradiated dentin by transmission electron microscopy (TEM) analysis. Further studies could evaluate the influence of NaOCl application on lased and acid-etched dentin prior to bonding procedure.
Conclusions
The results show that the application of a 5% NaOCl solution significantly decreases the microleakage of resin–composite fillings in Er:YAG laser-prepared dentinal cavities. Our study also shows that the proteolytic effect of NaOCl on the irradiated surface improves the quality of dentinal bonding.
Footnotes
Author Disclosure Statement
No competing financial interests exist.