
Abstract
Introduction
Modern DO originated in the 1950s with studies by the Russian orthopedist Gabriel Ilizarov, whose “tensile stress law” stated that the tensile stress generated by gradual stretching of live tissue stimulates their active growth and regeneration. 1,3 DO was first used in the mandibular area in a canine study by Snyder et al. 4
Various surgical and nonsurgical strategies have been developed in an attempt to stimulate bone tissue repair. Growth hormones, cytokines, bone morphologic proteins, and electric and electromagnetic stimulation and low-level laser therapy (LLLT) have been and continue to be used to accelerate bone healing. 5 –8
Modification of the inflammation period and acceleration of bone repair through the biological stimulation of tissues using lasers has been a significant treatment modality. LLLT was first used in the treatment of unhealed ulcers, 9 and its role in increasing osteoblastic activity during bone repair to enable rapid bone healing has been reported. 10
Ultrasound therapy has also been used to apply micromechanical vibrations to bone and bone cells in order to accelerate bone healing by mimicking physiological stress, with the therapeutic effect of ultrasound apparently arising from piezoelectric and angiogenetic effects on cell membranes. 11
Increases in bone tissue substance per centimeter can be assessed by measuring bone mineral density (BMD), which is also used to evaluate loading capacity and fracture risk, given the statistical relationship between BMD and both loading capacity and fracture risk. BMD is commonly measured using conventional radiographic techniques; however, with new technological developments in recent years, the use of other minimally invasive procedures such as single- and double-photon absorptiometry, quantitative computed tomography, quantitative ultrasound, radiogrammetry, digital x-ray radiogrammetry and single and double x-ray absorptiometry has also become widespread. Composed of both an x-ray source and detector, dual energy x-ray absorptiometry (DEXA) devices perform photon scans of tissue at two different energy levels (40 and 140 kV) and evaluate BMD results in g/cm2.
A direct comparison of the effects of LLLT and LIPUS on the DO consolidation period in the same subject does not exist in the literature. It has been hypothesized that LIPUS and LLLT may affect BMD value during DO consolidation period. Therefore, this study aimed to evaluate and compare the effects of LLLT and LIPUS on DO consolidation in terms of changes in BMD.
Methods
Approval for this study was obtained from the Animal Testing Ethics Committee of Ankara University (No: 2008-18-71). All procedures were performed with the animals under general anesthesia in accordance with humane methods. Fifteen New Zealand rabbits aged 3–5 months were randomly divided into three groups (n=5) according to treatment, as follows: Group A: DO; Group B: DO+LIPUS (30 mW/cm2 [1 MHz]) for 20 min daily; Group C: DO+LLLT (650 nm wavelength; 25 mW output power; continuous wave; diameter 11 mm [beam area: 0.95 cm2]; 0.026 W/cm2, two times a day each for 300 sec and a total of 600 sec irradiation time; energy density: 16 J/cm2 a day; total energy: 15 J/day and one irradiation area). For all rabbits, the distraction period was 10 days.
Surgical procedures (DO)
Hair was removed from the animal's left mandibular area and the surface washed with antiseptic to provide sterile conditions for surgery. General anesthesia was provided with 10–20 mg/kg ketamin and 3 mg/kg Rompun®, and local anesthesia and hemostasis were achieved with 0.5 cc Ultracaine. A skin incision was made 0.5 cm below and parallel to the inferior margin of the mandible. The inferior margin of the mandible was accessed by blunt dissection, and the mandible itself was accessed through an incision of the periosteum along the inferior margin. The osteotomy incision line was prepared 2 mm from the apical and coronal margins with the aid of round drills beginning 1 cm mesially from the mandibular ramus. Custom-designed distractor plates were adjusted and fixed at both sides of the incision line, and the osteotomy was performed using a thin edged straight saw blade at a rate of 25,000 rpm under intensive saline cooling (Fig. 1). Following DO, a mean 10 mm of bone gain was achieved in the left mandibles of all rabbits, which resulted in cross-bite.
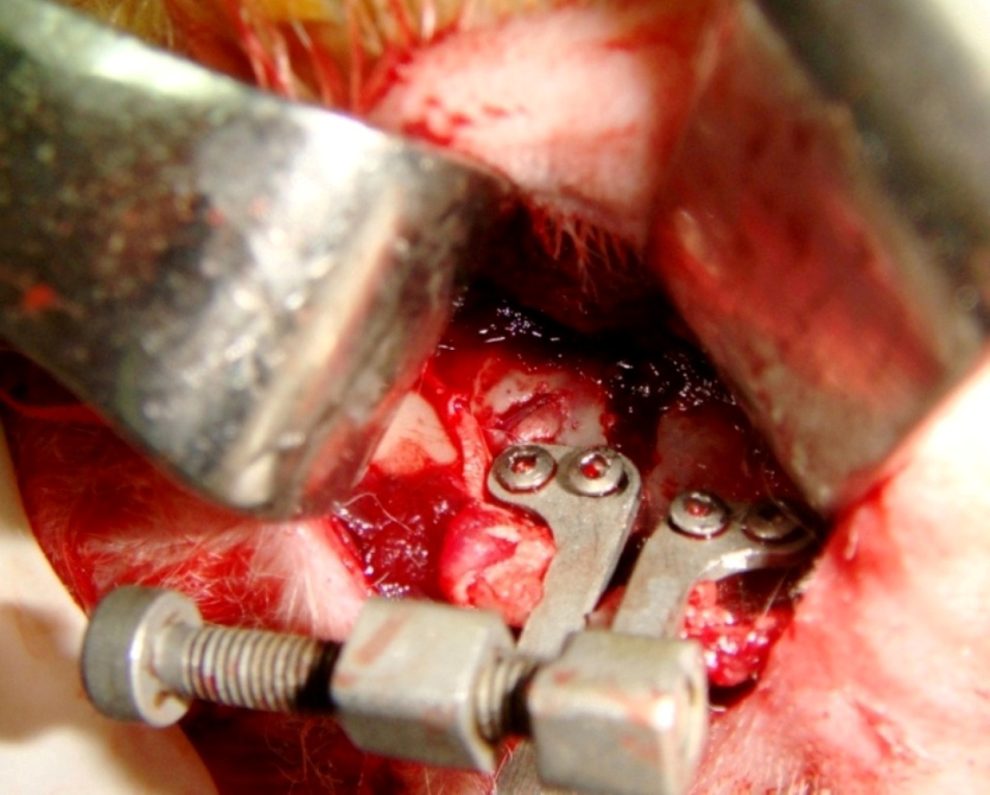
Osteotomy line with the custom-made distractor placed in the posterior mandible.
Radiologic evaluation
DEXA examination of the treatment areas were performed immediately prior to the DO (baseline) and at 30 and 60 days postoperatively. Standard radiographs were also taken as a control (Figs. 2 and 3).
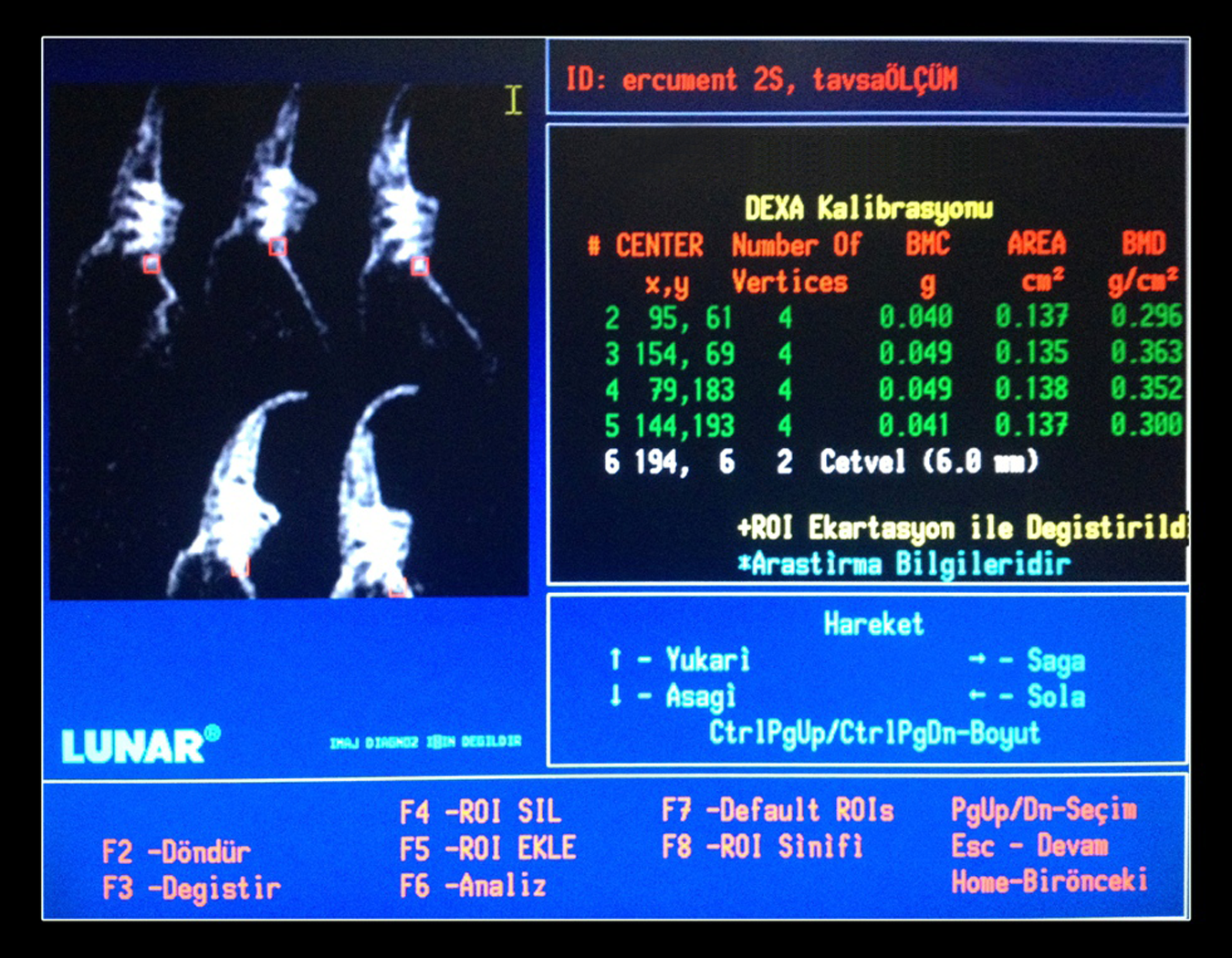
An example of the dual energy x-ray absorptiometry (DEXA) measurement of the #5 (Group A).

Control radiograph of the distractor area.
Statistical analysis
BMD means and standard deviations were calculated for each group. Sample t tests were used to assess changes over time for each group in 95% confidence interval.
Results
In the control group, mean BMD values of all rabbits at 30 days were below baseline. At 60 days, BMD values were above baseline in one rabbit, at baseline in three rabbits, and below baseline in one rabbit (Table 1). Overall, mean BMD values were below baseline at both 30 and 60 days, but the difference was greater at 30 days (Fig. 4). Pairwise comparisons of mean BMD values of rabbits in the control group showed statistically significant differences between baseline and 30 days (p=0.0001), baseline and 60 days (p=0.022), and 30 and 60 days (p=0.0004).
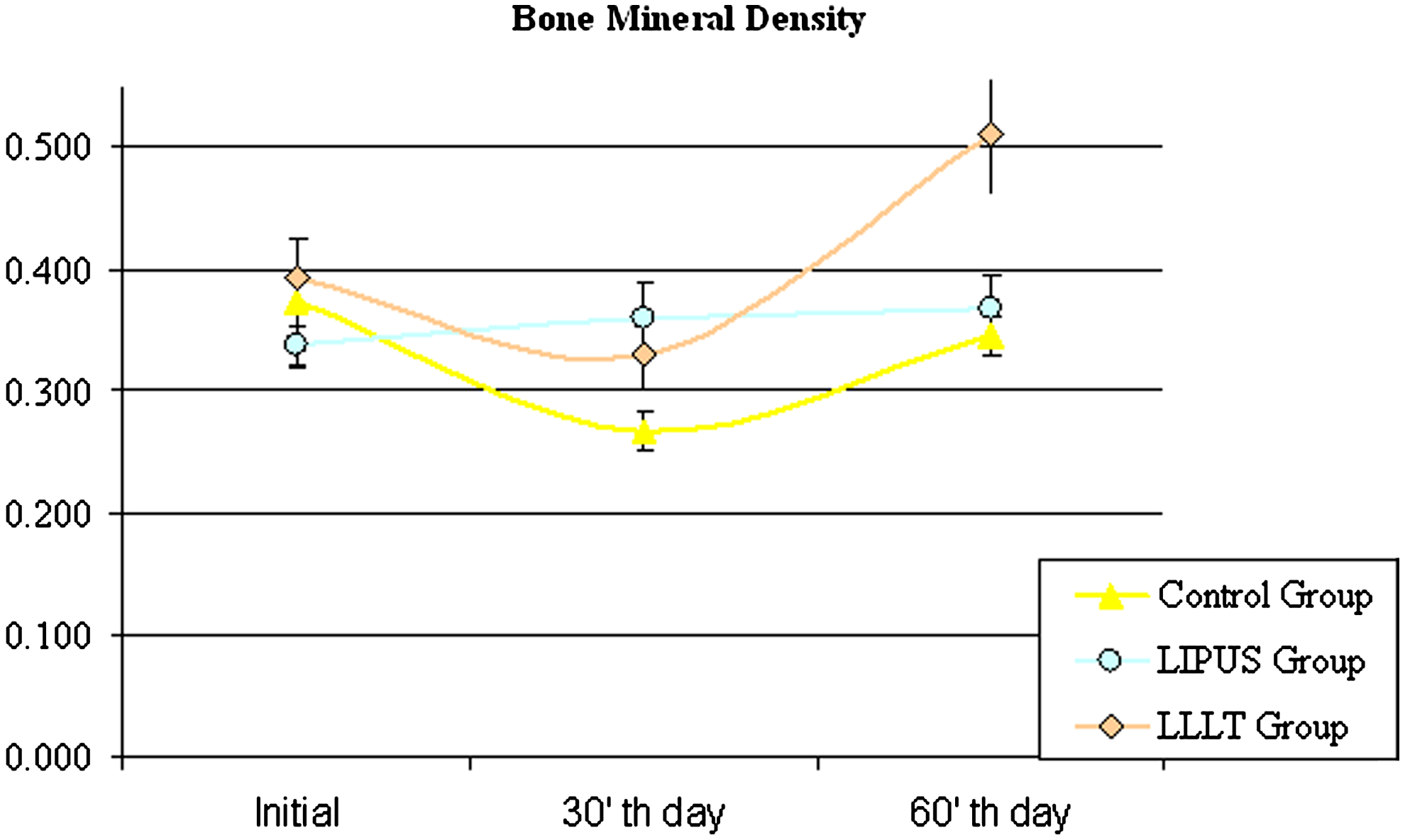
Changes in bone mineral density values over time, by groups.
In the LIPUS group, mean BMD values increased from baseline to 30 days and increased further from 30 to 60 days (Table 1 and Fig. 4). However, pairwise comparisons of mean BMD values in the LIPUS group did not show statistically significant increase between baseline and 30 days (p=0,153), baseline and 60 days (p=0.059), and 30 and 60 days (p=0.552).
In the LLLT group, BMD values were below baseline at 30 days, but increased to above baseline at 60 days (Table 1). Pairwise comparisons of mean BMD values in the LLLT group showed statistically significant differences between baseline and 30 days (p=0.01), baseline and 60 days (p=0.005), and 30 and 60 days (p=0.001).
At postoperative 60 days, the increase in BMD value over baseline was found to be significantly greater in the LLLT group than in the LIPUS group (Fig. 4).
Discussion
Over the past 20 years, DO has come into more common use in maxillofacial surgery for the correction of congenital and acquired deformities, as well as for treatment of bone loss. The success of DO is dependent upon a number of technical parameters, including latency period, distraction rate and rhythm, and consolidation time. Reducing the latency and consolidation phases minimizes the risk of infection and treatment failure. The literature describes numerous methods that aim to shorten therapy time by accelerating bone regeneration.
Various studies have reported on DO latency phases and distraction rates. A 1989 study by Ilizarov reported that a minimum of 7 days was required for the latency phase in adults, although this period could be shorter in children. 1 Aida et al. 12 compared latency periods of 0, 2, 5, and 10 days in the use of DO to treat rabbit mandibles, and suggested 5 days as the optimal latency period; the authors reported no bone trabecula development with latency periods of 0 and 2 days, but found the distraction space to be rich with immature bone trabecula at 5 days. Today, a latency period of up to 7 days and a distraction rate of 1 mm/day is generally accepted as standard in the DO treatment of long bones. A web-based study reported that most clinicians applied a 3- to 7-day latency phase (82–88%) and a distraction velocity of 1 mm/day (88–92%). 13 Taking rabbit weight, height, and mandible size into consideration, the present study found the optimal latency phase to be 7 days, and the optimal distraction rate to be 1 mm/day.
One of the greatest disadvantages of DO is the lengthy consolidation period, with mean ossification time reported to be between 28 and 36 days. 14,15 An early study on rabbit mandibles reported 1–2 months to be appropriate as a consolidation period, with mature callus containing mature lamellar bone visible after 4 weeks. 16 Based on these earlier DO studies performed on the same species, the overall period of this study was set at 60 days, with a consolidation period of 43 days and BMD measurements recorded at 30 days postoperatively (day 13 of consolidation) and 60 days postoperatively (day 43 of consolidation) for comparison.
The present study found BMD values at 30 days (day 13 of the consolidation phase) to vary significantly between the LIPUS and control groups. These values were in line with those obtained at the second week in similar studies (Fig. 4). 17,18 BMD values in the LLLT group were also consistent with those obtained histopathologically in a similar study (Fig. 4). 19 Although there has been no clear explanation of how this mechanism operates, laser therapy has been shown to prevent cell apoptosis and increase cell proliferation, migration, and adhesion. 20 –22 LLLT has been shown to be effective in treating various acute and chronic conditions in different animals by accelerating wound healing through neovascularization, angiogenesis, and collagen synthesis. 23,24 A study examining the use of LLLT in bone healing found that LLLT stimulated osteoblastic activity. 10 Other studies have shown LLLT to accelerate mineralization and increase osteoblasts and osteointegration by increasing mitochondrial activity. 25 –27 With regard to the present study, the greater increases in mean BMD values at 30 and 60 days over controls can be attributed to the increasing osteoblastic activity mentioned in the literature.
Not only has LLLT been reported to be effective in the distraction phase, it has also been reported to be effective in the consolidation phase because of improved blood circulation. 19,26,28
LLLT effectiveness may vary according to laser dose, in terms of both power output and application time. Whereas some studies have recommended high doses varying between 10 and 112.5 J/cm2, 26,27,29 other studies have indicated levels of 0.03–3 J/cm2 to be effective. 25,30,31 In addition to dose, target tissue represents another important criterion, as mucosa and fat tissue penetration is more easily achieved than muscle tissue penetration. The dose-dependent effects of LLLT are frequently explained using the Arndt–Schulz law, 32 which states that while smaller amounts result in biostimulation, as the amount increases, the effect is reversed, and bioinhibition occurs. 33 Some studies have stated that high doses can be destructive and have advocated the use of 3–5 J/cm2 rather than 50–100 J/cm2. 34 The LLLT apparatus used in the present study has an output of 25 mW, and a daily dose of 16 J/cm2 was applied to each rabbit. The laser dose used in the present study is consistent with the literature, and the changes in BMD values measured in the laser group were found to be significant (Fig. 4). Laser wavelength and dose has also been reported to have an effect on live healing. 35 The present study found that bone healing improved with a twice-daily application of LLLT at a wavelength of 650 nm and a maximum of 16 J/cm2.
Low intensity ultrasound has also been shown to accelerate fracture healing in experimental and clinical studies. Duarte 36 first reported on the positive effects of low intensity ultrasound applications on bone healing in 1983, and a number of subsequent studies reported that LIPUS treatment accelerated healing of long bone fractures. 37,38 Fëdotov et al. 39 were the first to report on the use of ultrasound applications in maxillofacial surgery in their study of mandible fractures in rabbits. This study was followed by one by Harris et al. 40 in which ultrasound was used to treat mandible osteoradionecrosis in humans. A healing ratio of 88% was reported by another study of 1317 fracture cases in humans in which ultrasound was used with conventional therapy methods; delayed or no ossification was observed during a 9 month period. 41 Another study showed that LIPUS application for 20 min/day for 10 days following a DO to lengthen a right rabbit tibia had significant positive effects on bone mineral density at the callus phase as well as stiffness and fracture strength after 3 weeks. 17 LIPUS application of 20–50 mW/cm2 was reported to raise tissue temperature <1°C, but this temperature increase and the absorption of energy by tissues and cells was reported to cause significant changes in bone formation. 42 According to another study, LIPUS was also shown to generate changes in the amounts of enzymes such as matrix metalloproteinase 1 (collagenase 1), despite minimal increases in temperature. 43 Ultrasound has also been reported to decrease edema by stimulating mast cell secretions in rats. 44 Furthermore, ultrasound stimulation was reported to increase leukocyte adhesion to endothelium in the inflammation period of fracture healing; to stimulate collagen synthesis from fibroblasts; and to increase the release of macrophages, fibroblasts, and vascular endothelial growth factor. 45 –47
Ultrasound has been found to be especially effective in the early periods of fracture, according to a study in which rats with bilateral fibular fractures were treated with 500 mW/cm2 ultrasound. 48 A study in which dogs received 40 mW/cm2 LIPUS for 20 min/day during the distraction period found higher BMD values at 2, 4, 6, 8, and 12 weeks, when compared with controls that received no LIPUS. 18 Ultrasound application in the early period of fracture is considered to reduce the inflammation period and speed the onset of repair. 18,48
A study with rats found that the mechanical properties of newly developed bone were better when ultrasound was applied at 50 mW/cm2 when compared with 100 mW/cm2 and with no ultrasound treatment. 49 Considering that similar animal studies found appropriate doses to range from 20 to 100 mW/cm2 and from 1 to 1.5 Mhz, the dose of 30 mW/cm2 at 1 MHz LIPUS was applied in this study.
In addition to DEXA, quantitative tomography has also been reported among the most appropriate techniques for measuring BMD. 50 However, although it is capable of providing a complete three-dimensional analysis of bone, it has the disadvantages of both high effective doses and high costs. DEXA provides high resolution imaging that enables near-real estimation with low doses of radiation. 51 However, because DEXA provides two-dimensional rather than three-dimensional measurements, it may not be sufficient for the measurement of superimposed areas.
In the present study, BMD in the distraction area in the control group showed an initial decrease at 30 days following DO, but was similar to baseline at 60 days postoperatively. In contrast, BMD values in the LLLT group at 30 days were similar to those at baseline, and at 60 days exceeded baseline, and BMD in the LIPUS group exceeded baseline values at both 30 and 60 days postoperatively. The present study demonstrated that LIPUS and LLLT applied during the distraction period had positive effects in terms of accelerating healing and ossification. Despite the small cohort of this study, it may be suggested that LIPUS and LLLT may have clinical application in enabling early termination of fixation in fracture therapy, reducing postoperative edema in minor surgical procedures and accelerating healing. LIPUS and LLLT may also be helpful in accelerating osteointegration of intraosseous implants, and treating temporomandibular irregularities. LLLT has been shown to stimulate bone marrow cell production; 52 however, it has also been suggested that LLLT has a negative effect on the physical properties of new bone when applied in the early period of healing. 26 In order to identify therapy options and benefits to humans, additional experimental studies need to examine various criteria, including application time, dose, duration, and frequency for LIPUS, and wavelength for lasers in terms of their effects on hard and soft tissue. 19
Conclusions
LLLT and LIPUS are both safe, noninvasive procedures that may improve the outcome of DO treatment, which is both difficult and costly. However, given the limited number of clinical and experimental reports in the literature, further comparative research is necessary. Studies should include an examination of the effectiveness of LIPUS and LLLT when used in the consolidation period, in comparison with the distraction period.
Footnotes
Author Disclosure Statement
No competing financial interests exist.