
Abstract
Introduction
There have been some reports about carbon dioxide (CO2) laser in spinal surgery for disc herniation and discal cyst. 8 –11 Because CO2 laser can enable the precise dissection and removal of adhesion scar and accompanying rLDH more effectively, we aimed to determine whether CO2 laser is an effective alternative tool to scalpel in revision microdiscectomy of rLDH. In this study, we used CO2 laser instead of blunt scalpel for sharp and precise dissection of adhesion scar. We report 21 cases of rLDH that were treated by revision microdiscectomy using a CO2 laser and discuss the clinical manifestations, radiologic findings, and usefulness of the CO2 laser for rLDH.
Methods
Data collection
We retrospectively reviewed the clinical and radiologic data of 21 patients with rLDH between October 2006 and July 2010. There were 12 men and 9 women, with a mean age of 49.1 (range, 30–73) years. Medical records were reviewed, and patient demographics, clinical symptoms, operative parameters, duration of hospital stay, preoperative radiographic findings, and postoperative clinical results were assessed. To evaluate the severity of preoperative patients' condition, all patients were assessed with the visual analogue scale (VAS) and Oswestry Disability Index (ODI). Same parameters were also assessed to evaluate the postoperative outcomes. All patients underwent preoperative radiographs, lumbar CT scans, and magnetic resonance imaging (MRI) of the lumbar spine. All patients had had relapse of radicular pain or numbness along the dermatome that they had experienced previously. The average duration of symptoms was 28.8 days (range, 3–113 days). A paired student's t test was used to compare the preoperative and postoperative clinical outcomes and p<0.05 was considered to indicate a statistically significant difference.
Surgical technique
Most procedures are the same as in conventional microdiscectomy. A skin incision was made along the previous incision. Paravertebral muscles and adhesion scar were gently dissected, then, the scar was gently removed from the lamina with curettes to confirm the previous laminotomy bone margins, with great care not to make an incidental durotomy. Then an extended partial laminectomy with or without foraminotomy using a high-speed diamond drill was performed under the operating microscope. The adhesion scar and granulation tissue covering the dura and ligamentum flavum were gently dissected by using the CO2 laser (Sharplan 30C, Lumenis, Yokneam, Israel). An adapter was used to attach the laser to the operating microscope, making possible micromanipulations of the laser with a joystick. The spot diameter of the laser was 0.3 mm and the power level was 5 W with single-pulse mode, which allowed safe and precise dissection. The affected disc was exposed by gentle retraction of the thecal sac and traversing nerve root. Epidural veins around the disc were coagulated with a bipolar coagulator, and the nerve root was gently retracted using a root retractor, exposing the adhesion scar over the rLDH (Fig. 1). The adhesion scar was dissected using a CO2 laser and dissector. Next, the surgeon made an annulotomy using CO2 laser and removed the ruptured disc fragments. By extension of this hole using a CO2 laser, surgeons can create enough of an annulotomy to remove the protruded disc under retraction of the traversing nerve root. After confirming the adequate decompression and release of the nerve root using the microprobe, the wound was closed in a conventional way.
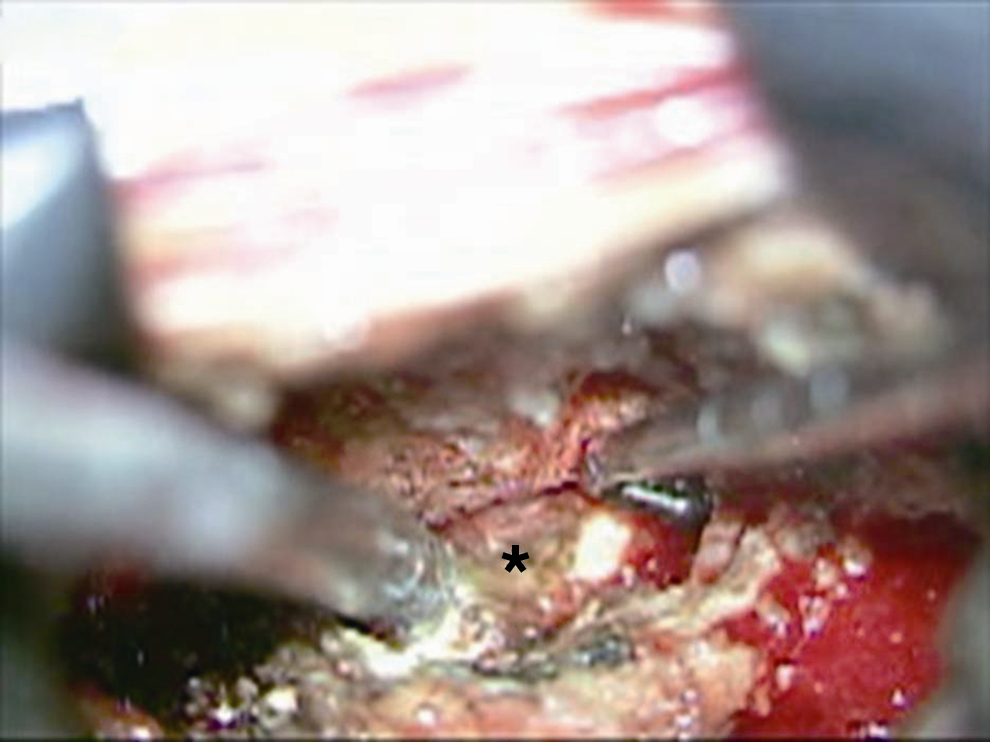
Operative view showing granulation tissue and recurrent lumbar disc herniation located ventromedially to the L5 nerve root (black asterisk).
Illustrative case
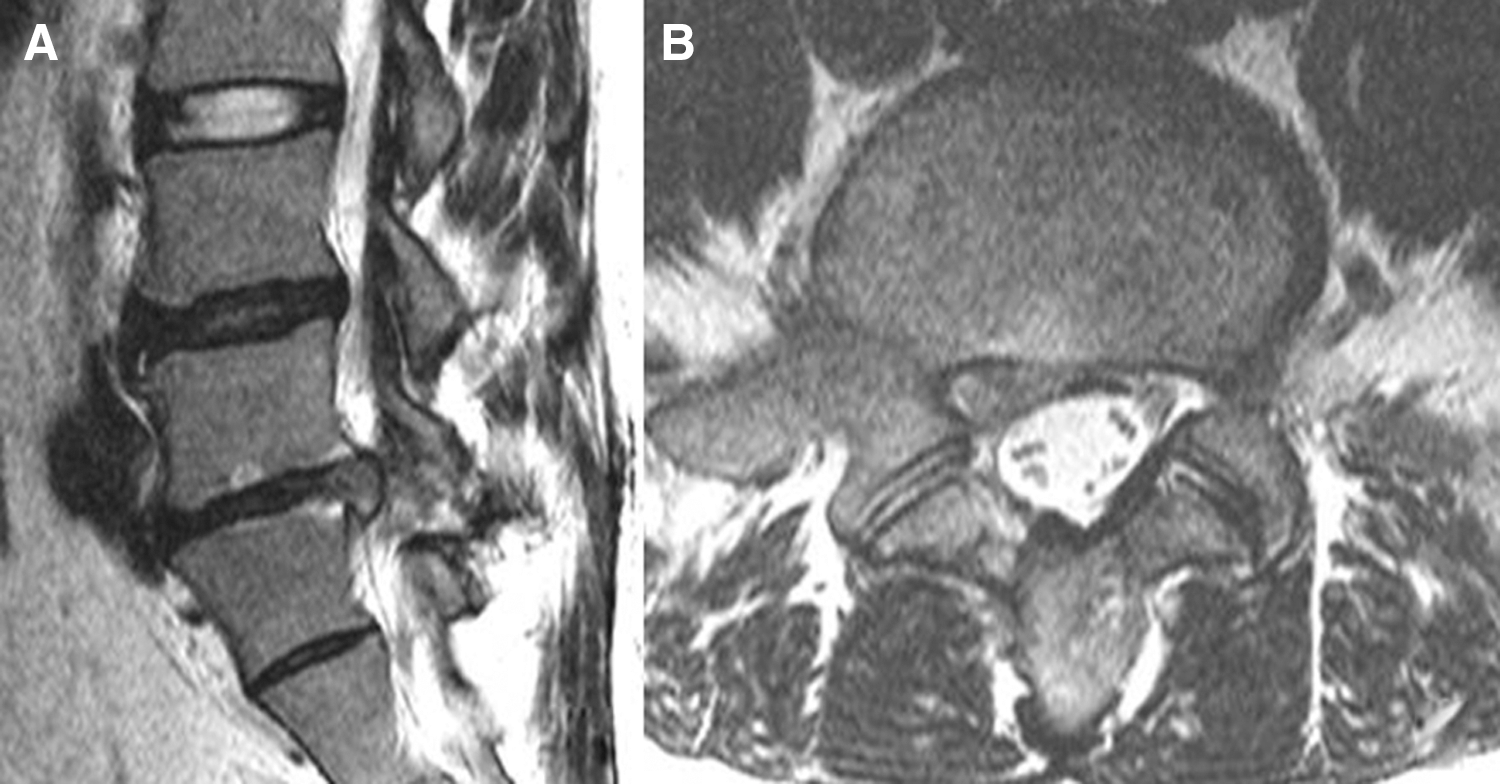
A 35-year-old man who had undegone microdisectomy 2 years ago visited the clinic because of a 2 month course of radicular leg pain along his S1 dermatome. MRI scans revealed degenerative discs at L5-S1 as well as a large rLDH causing S1 nerve root compromise (Fig. 2A and B). The patient underwent revision microdisectomy using CO2 laser for rLDH. During surgery, moderate to severe epidural granulation tissue was found to be located dorsolaterally to the nerve root with severe adhesion to the dura. After gentle dissection of epidural scar using CO2 laser, rLDH was identified and removed successfully without nerve root injury. The patient's lower extremity pain improved remarkably after the operation.
Results
The clinical results are summarized in Table 1. The series comprised 12 men and 9 women whose mean age was 49.1 years (range, 30–73 years). The mean symptom duration was 28.8 days (range, 3–113 days) and there was a mean follow-up duration of 30 months (range, 9–63 months). The rLDHs were located at the L4-5 level in 14, at the L5-S1 level in 6, and at the L3-4 level in 1 of the 21 patients. There were no complications related to the procedures.
VAS, visual analogue scale; ODI, Oswestry Disability Index; SNRB, selective nerve root block.
The mean preoperative VAS for leg pain was 7.6, which improved to 3.0 (p<0.001) and the patients' mean score on the Korean version of the ODI had improved from 57.4% to 22.2% (p<0.001) by the last follow-up. At 4 weeks after the surgery, 8 out of 21 patients showed a marked improvement of radiating leg pain. Four out of 21 patients had improved, but still had residual leg discomfort. Therefore, these four patients underwent fluoroscopy-guided selective nerve root block (SNRB) one more time and showed a marked improvement of leg discomfort. Six patients who had moderate degree of discogenic back pain (VAS 4∼7) had taken medication for a few months.
Discussion
Surgical treatments of rLDH, including revision microdiscectomy and lumbar fusion with or without instrumentation have been reported, and the clinical outcomes of these treatments have been considered to be favorable. 12 –14 Recently, with the aid of specialized instruments such as endoscopes with video equipment and others, some kinds of minimal invasive methods have been introduced for the treatment of rLDH. 1,15 –24 Some authors reported a patient with rLDH who was treated using the METRx™ (Medtronic Sofamor Danek, Inc., Memphis, TN) system 22 –24 and others 6,24 –26 attempted to remove rLDH using a percutaneous endoscopic lumbar discectomy (PELD) and other systems. 1,15 They noted that favorable pain relief was achieved for most patients through this procedure. However, because PELD and other systems usually have a steep learning curve, 27 they are not commonly accepted for the treatment of rLDH.
For the above reasons, revision microdiscectomy is still more popular and has been considered the treatment of choice rather than lumbar fusion or minimally invasive surgeries such as tubular discectomy, PELD, and others.
In the authors' hospital, there have been operating microscopes attached with CO2 laser, 11,12 and surgeons have used these during lumbar microdiscectomy including revision surgery. During revision microdiscectomy, surgeons can focus the laser beam exactly on the targeted adhesion scar for adhesiolysis and vaporization, so quick and easy dissection of the adhesion scar tissue is possible.
Because epidural or perineural scar tissue may hinder the dissection in revision microdiscectomy, increasing the risk of incidental durotomy or iatrogenic neural injury, CO2 laser could help surgeons perform more precise and safe dissection of the scar tissue than with a blunt scalpel. Calcifications around the recurrent disc fragments are often seen, which may also hinder the surgeons' ability to dissect safely. But with the aid of a CO2 laser, surgeons could evaporate the calcified portion of the disc without excessive retraction of the nerve root via a narrow operative corridor. 8 Moreover, with a slight gentle retraction of the nerve root, surgeons could easily access the narrow ventral part of nerve root using CO2 laser, where a blunt scalpel could not access (Fig. 3).

Operative view presenting easily accessible narrow ventral part of nerve root using CO2 laser where blunt scalpel could not access, with a slight gentle retraction of the nerve root.
According to the literature, the risk of incidental durotomy has been reported in up to 20% of the patients who underwent revision microdiscectomy. 14 Dural tear during lumbar disc surgery is associated with long-term clinical sequelae and poorer clinical outcomes. 3 In our series, no approach-related or CO2 laser-related complications developed. The authors believe the reason that there was no incidental durotomy in our series may be the precise and gentle dissection of theCO2 laser.
Since Choy et al. 28 reported the first trial of neodymium yttrium-aluminum-garnet (Nd: YAG) during lumbar disc surgery in 1986, many studies about the usefulness of lasers for disc surgery have been reported. 8 –11 However, no studies about the usefulness of the CO2 laser for removal of rLDH have been reported. This study suggests that CO2 laser could be a useful surgical tool for conventional microdiscectomy techniques for revision microdiscectomy in rLDH, because the CO2 laser enabled effective delicate and precise dissection of adhesion tissue without excessive violation of the facet joint, while preserving spinal stability. Studies about the pathologic effect of the CO2 laser on the intervertral disc are very rare. However, according to some reports, there was a serial proliferation of cells, increased production, and reorganization of collagen resembling the normal architecture of fibrocartilage after CO2 lasering. 29,30
Considering the surgical usefulness of the CO2 laser during revision surgery and the pathologic aspect of CO2 laser, we suggest that the introduction of the CO2 laser in microdiscectomy for rLDH could be recommended. The results of the present study suggest that CO2 laser-assisted microdiscectomy could be an effective alternative to conventional microdiscectomy techniques.
Conclusions
In this study, 21 cases of rLDH, which caused the same symptoms and signs as those of virgin lumbar disc herniations, were excised successfully with revision microdisectomy using a CO2 laser. Our results demonstrate that the CO2 laser could be a useful surgical tool during revision microdisectomy of an rLDH.
Footnotes
Acknowledgment
This study was supported by a grant from the Wooridul Spine Hospital.
Author Disclosure Statement
No conflicting financial interests exist.