
Abstract
Introduction
Currently used canal debridement and shaping techniques produce a smear layer consisting of microorganisms and necrotic debris on canal walls, 7 which might prevent penetration of antimicrobial agents into the dentinal tubules. 8 However, antimicrobial agents might not be able to exert any influence on microorganisms in deep dentinal layers, because of their limited penetration potential. 9
Enterococcus faecalis is commonly isolated from endodontically treated teeth with refractory periradicular disease. 10 The bacteria can produce bacterial biofilm. 11 Biofilm bacteria are 1000 times more resistant to antibacterial agents than planktonic bacteria and are difficult to eliminate. 12
As laser penetration depth can be adjusted, laser provides better access to the canal areas that were previously inaccessible. 13 Nd:YAG laser has gained great popularity in endodontics because of its effective antiseptic properties. 14,15
Previous studies have evaluated the effect of various lasers on E. faecalis. 13 –19 However, the majority of previous studies have evaluated planktonic cells, and the effects of these lasers on the bacteria in the biofilm are less recognized. Given the increased use of lasers, the present study aimed at evaluating the effect of Nd:YAG laser and 1% sodium hypochlorite solution as a new protocol on E. faecalis biofilm in the root canals of infected teeth.
Materials and Methods
Sixty freshly extracted human maxillary central incisors with mature apices and straight roots were selected. The tooth crowns were removed to leave 12 mm of root length. Then the working length was determined using a #20 K-file (Dentsply Maillefer, Ballaigues, Switzerland). Subsequently, #4, #3, #2 and #1 Gates-Glidden drills (Dentsply Maillefer, Switzerland) were used to prepare the canal walls using the crown-down technique. Canal instrumentation was perforomed up to #60 K-file. Physiologic serum was used for canal irrigation. The smear layer was removed using 5.25% sodium hypochlorite solution for 3 min, followed by 17% EDTA (Pulpdent Corp., MA) for 3 min. Transverse sections were prepared from the samples to evaluate the dentinal tubules of teeth before formation of E. faecalis biofilm under a scanning electron microscope (SEM) (VEGAII TESCAN, Cranberry, PA) (Fig. 1A and B).
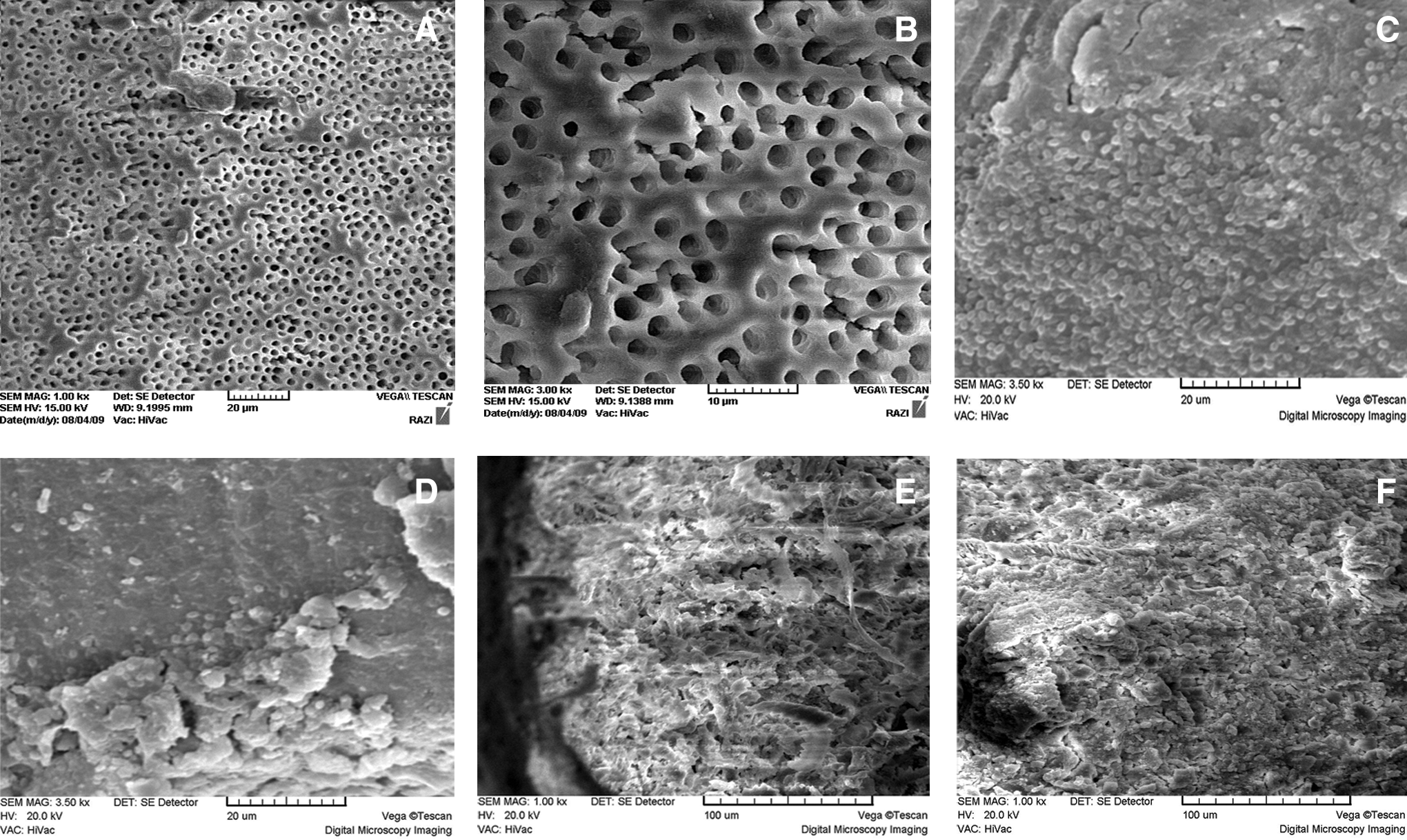
Scanning electron microscopic (SEM) images of dentinal tubules of teeth without Enterococcus faecalis biofilm at ×1000
Formation of biofilm
The teeth were placed in an autoclave at 121°C and a pressure of 15 psi for 20 min in order to eliminate all the existing microorganisms. The teeth were incubated at 37°C for 24 h in brain–heart infusion broth (Merck, Darmstadt, Germany) in order to confirm sterilization. In the next stage, each tooth was placed in a sterile microtube containing 2 mL of a standard suspension of E. faecalis (ATCC 29212). In order to prepare the standard suspension, at first a pure culture of the microorganism was provided by incubating the bacteria at 37°C for 24 h in the presence of 10% CO2. Then the young bacteria were cultured in the brain–heart infusion broth (Merck) and the microbial concentration was adjusted to the standard 0.5 MacFarland solution (108 cells/mL) using a UV VISIBLE spectrophotometer (Shimadzu, Japan) at an optical density (OD) of 1 at 600 nm. The broth culture medium was renewed every other day to guarantee the stability and nutritional support of the culture medium and elimination of all the additional bacterial cells. The procedure continued for 6 weeks, during which the teeth were incubated at 37°C. After 6 weeks, transverse sections were prepared from the samples to evaluate and confirm formation of biofilms under an SEM (Fig. 1C–F).
Study groups
The teeth were randomly divided into four groups of 15 teeth each:
Group 1: the control group
Group 2: 3 W Nd:YAG laser
Group 3: 3-W Nd:YAG laser plus 1% sodium hypochlorite
Group 4: 1% sodium hypochlorite
Group 1 (the control group): The samples in this group underwent no intervention.
Group 2: A fiber tip with a diameter of 200 μm was used to deliver a 3 W beam of Nd:YAG laser (LAMBDA S.P.A, Brendola, Italy) into the root canals; the laser beam had a wavelength of 1064 nm, an energy of 120 mJ, and a frequency of 25 Hz. The total irradiation time was 10 sec for each canal.
Group 3: The root canals were irrigated with 1% sodium hypochlorite solution using 21 gauge 5 mL syringes. The irrigation procedure was repeated every 5 min, a total of 15 mL of the irrigation solution was used, and the overall contact time of sodium hypochlorite solution with the canal wall was 15 min; sodium thiosulfate was used to prevent the effects of carry-over. Then the samples underwent a laser irradiation procedure in the same manner as described for group 2.
Group 4: The samples underwent only an irrigation procedure in the same manner as described previously.
The disinfection efficacy was evaluated by collecting dentin chips produced by scraping the root canal walls with #6 and #5 Gates-Glidden drills. A total of 10 mg of dentin chips were collected from each root canal. The dentin chips were placed in pre-weighed microtubes, which were weighed again during collection of the chips using a sensitive electronic weighing machine (A&D Co., LTD, Japan).
The samples were transferred into test tubes containing 2 mL of sterile physiologic serum and were mixed using a whirling motion. Then tenfold serial dilutions were prepared up to a concentration of 10−7. Then 10 μL of each concentration was transferred to three Mueller–Hinton agar plates, which were incubated at 37°C for 48 h. After the incubation, colony-forming unit (CFU) counts were determined on each plate. The mean CFU counts were calculated for the three plates with concentrations of 10−2, 10−3, and 10−4. Then the means were converted to the 10−3 concentration, summed up and divided by three to achieve one CFU count for the samples in each group.
Statistical analysis
Kruskal–Wallis and Mann–Whitney U tests were used to evaluate differences between the groups. Data were analyzed with descriptive statistical tests (mean±SD) using SPSS 13 statistical software. Statistical significance was defined at p<0.05.
Results
The bacterial counts before and after laser application and irrigation with sodium hypochlorite solution are presented in Table 1. Kuruskal–Wallis test revealed significant differences between the groups under study, with statistically significant differences between groups 1 and 3 (p<0.001, χ2=49.3). Mann–Whitney U test was used for the two-by-two comparison of the groups. The results showed more bacterial counts in group 1 than in groups 3 and 4 (p<0.001). Although laser irradiation had decreased bacterial counts, there were no significant differences between the control and laser groups (p>0.05). A combination of laser irradiation and sodium hypochlorite solution had resulted in a 100% decrease in bacterial counts.
CFU, colony-forming units.
Discussion
A combination of laser beam and 1% sodium hypochlorite resulted in complete inhibition of growth of bacteria present in the biofilm in this study; however, the application of only Nd:YAG laser beams did not eliminate the bacterial biofilm. E. faecalis is isolated in most cases of root canal treatment failures. 20 –22 This microorganism is resistant to intracanal medications, such as calcium hydroxide, 23,24 and might colonize the root canal space without being supported by other intracanal microorganisms. 25 It has been reported that E. faecalis can contaminate the entire length of dentinal tubules in 48 h. 26 It can penetrate into the dentinal tubules up to 300 μm and survive. 8,27 However, a period of 48 h is too short for the formation of biofilms within the dentinal tubules. According to Kishen et al., 28 bacterial biofilms, particularly those of E. faecalis, can form a calcified layer on the root canal dentin and extraradicular areas; an increase in the number of phosphate and carbonate bonds is observed in 4–8 weeks, and biofilm structure exhibits signs of mineralization after 6 weeks, which might reflect a factor associated with the persistence of this microorganism after root canal therapy. Therefore, in the present study, the samples were incubated for 6 weeks to simulate in vivo conditions. After 6 weeks, SEM photomicrographs revealed biofilm formation with the adhesion of bacteria to the dentin, consistent with the results of a study by Chivatxaranukul et al., and Ozdemir et al. 29,30
Nd:YAG is probably the best laser for the disinfection of root canals based on the reports available. 31,32 Bergmans et al. 33 reported a significant decrease (99.7%) in E. faecalis counts within the root canals by Nd:YAG laser, whereas in this study, Nd:YAG laser alone did not significantly decrease bacterial counts in comparison with the control group, which is attributed to the presence of biofilms. The number of the cells forming the biofilm, presence of an extracellular polymer material, the amount of growth, the composition of the cell wall, metabolic activity, and expression of genes in the planktonic cells are different in biofilms, and elimination of bacteria is difficult in the presence of a biofilm. 22 Therefore, in the present study, a new protocol was used to eliminate biofilms, in which subsequent to irrigation of the canals with 1% sodium hypochlorite solution, a beam of Nd:YAG laser was delivered. The results showed that the combination of the two techniques was more effective than Nd:YAG laser and 1% sodium hypochlorite separately in eliminating biofilm.
Folwaczny et al. 34 and Piccolomini et al. 35 reported that Nd:YAG laser decreases bacterial counts; however, they reported a better performance for sodium hypochlorite solution, consistent with the results of the present study in which Nd:YAG laser decreased bacterial counts less than that by sodium hypochlorite solution.
In a recent study by Meire et al., 36 the effect of various lasers, including Nd:YAG and Er:YAG, 2.5% sodium hypochlorite solution, and photodynamic therapy on E. faecalis biofilm was evaluated and the results showed that NaOCl was the most effective in eliminating biofilms and Nd:YAG laser was the least effective, which is consistent with the results of this study in which the use of Nd:YAG laser alone was not effective against E. faecalis biofilm.
The inability of Nd:YAG laser to completely eliminate bacteria might be attributed to the deep penetration of bacteria into the dentinal tubules so that they are immune to laser irradiation. In addition, E. faecalis bacterial cells might exhibit more resistance in unfavorable environmental conditions because of the presence of biofilm. 37 Another factor that might be involved in the persistence of bacteria in the root canals despite laser irradiation is the heterogeneous irradiation of laser on all the canal walls and the presence of areas without any laser effect. Because of the difficulty of eliminating biofilms after the common antiseptic procedures, use of adjunctive techniques, such as the use of lasers, might be useful during endodontic treatment. Further studies are necessary to determine the penetration depth of Nd:YAG laser and bacteria into the dentinal tubules and irradiation of surfaces with Nd:YAG laser in order to confirm the antimicrobial effects of this laser in endodontic treatment.
Conclusions
Based on the results of this study, the effect of Nd:YAG laser on E. faecalis is less than that of sodium hypochlorite solution. A combination of laser irradiation and sodium hypochlorite solution results in complete elimination of E. faecalis biofilms.
Footnotes
Acknowledgments
The authors thank the Dental and Periodontal Research Center and of Tabriz University of Medical Sciences for their technical and financial support of this research project.
Author Disclosure Statement
No competing financial interests exist.