
Abstract
Introduction
Fluoride is an established therapy for tooth demineralization control and prevention. 7 However, high-risk individuals who receive fluoride treatment can still develop pit and fissure caries. On the occlusal surface, some risk factors, such as the tooth morphology, hygienization difficulties, the eruption period, and patient age, need to be taken into account. 8 Pit and fissure sealant has been developed to overcome this problem. However, studies have demonstrated that complete or partial sealant loss is common, which can result in secondary caries. 9 Therefore, the need for new strategies and preventive measures for caries on occlusal surfaces is observed.
Stern and Soggnaes 10 were the first to demonstrate the increase of enamel acid resistance after exposure to laser irradiation. Other researchers have demonstrated satisfactory results using different types of lasers such as CO2, 11 –14 Er:YAG, 15 –17 and Nd:YAG lasers for the same function. 18 –21 The major theories regarding the effect of lasers focus on the fusion and recrystallization of the irradiated tissue using high energy densities; 5,13,17 –19 however, this treatment can damage the adjacent body tissue, as the heating of dentin and pulp tissues causes inflammation and pulp necrosis.
Recently some studies have tested irradiation in lower energy densities and have shown significant inhibition of enamel demineralization. 22 –24 In this way, other theories have attempted to explain the results obtained by using laser irradiation, for which the chemical changes observed on the irradiated enamel have been considered, such as the carbonate loss of the surface of irradiated enamel, 22,25 which means that the loss of carbonate from the enamel surface would render the undissolved tissue much less soluble in acid. 25 In this way, modification of the tooth mineral in such a way as to reduce destabilizing elements, such as carbonate, has been attempted, thus reducing the resulting solubility product (Ksp) for enamel mineral.
For the reasons stated, it is important to analyze the real effects of different lasers in preventing the formation of caries on occlusal surfaces. Therefore, the purpose of this study was to evaluate the effectiveness of three different types of lasers for caries prevention in pits and fissures.
The present study tested two null hypotheses: (1) There is no difference between the effects in the enamel surface caused by the different lasers tested. (2) The use of the CO2, Nd:YAG, and Er:YAG lasers does not cause any surface alteration that can increase the acid resistance.
Materials and Methods
Volunteers and ethical aspects
This in situ study was approved by the Research and Ethics Committee of the Ribeirão Preto School of Dentistry at the University of São Paulo (Proc. 2006.1.1238.58.0), and all of the volunteers signed informed written consent forms (Resolution No. 196 of the National Health Council, Health Ministry, Brasília, DF,10/03/1996). The study lasted for 14 days. The participants were 13 healthy volunteers (5 females and 8 males, ages 20–35 years) who resided in the same fluoridated area (0.8mg/L) and presented adequate stimulated (1–2 mL/min) and unstimulated salivary flows (0.3 mL/min) with no evidence of active caries or periodontal disease, and who wore the acrylic palatal appliances.
Experimental design
This study was conducted in accordance with a randomized complete block design. The factor under study was the treatment method of pit and fissure surfaces at four levels: (1) no treatment (control); (2) Er:YAG laser; (3) Nd:YAG laser; and (4) CO2 laser. Each group comprised 13 enamel blocks (n=13) randomly assigned to the 13 volunteers, who were considered as experimental blocks. The response variables were the cross-sectional Knoop microhardness of enamel, the enamel demineralization area assessed by polarized light microscopy (PLM) (mm2), and the morphological analysis obtained through scanning electron microscopy (SEM).
Specimen preparation
This study used 52 unerupted human third molars from the Ribeirão Preto Dentistry School Human Tooth Bank that were stored in a 1% formal saline solution. Fifty-two enamel blocks composed of pits and fissures (4×4×2 mm) were cut from the occlusal surface, sterilized, immersed in a saline solution, and then placed in an autoclave for a 30 min cycle. The enamel blocks were then covered with acid-resistant nail varnish, leaving a 7 mm2 (±0.5 mm2) exposed circular area considering the fissure irregularities. The care of fissures selection was attempted for the similarity of morphology of the selected fissures, excluding the deep fissures, so that the bottom of the fissure was in enamel. The type of fissure was determined in an examination in which fissures were characterized by the appearance of a uniform width of the fissure clefts. The cuspal inclines formed an angle narrower than the designated shallow fissures. Usually the base of the fissure appeared to be visible under illumination. 26
Laser irradiation
Control group (G1)
The enamel blocks were not subjected to any type of surface treatment. The samples from experimental groups G2, G3, and G4 were subjected to the laser treatment designated for that particular group.
Er:YAG laser (G2)
The equipment used for the Er:YAG laser surface treatment was a Kavo Key II device emitting at a wavelength of 2.94 μm (Kavo Dental GmbH & Co. KG, Biberach, Germany). The parameter settings used were 80 mJ of energy and 2 Hz. The pulse duration was 250–500 μs, and the 2051 handpiece with a removable tip attached to a flexible fiber delivery system was used. The laser beam was delivered in the noncontact, unfocused mode. The irradiation distance was 4 mm from the target site. The water flow used was a fine water mist at 5 mL/min (Table 1).
Nd:YAG laser (G3)
The equipment used for the Nd:YAG laser surface treatment was a Twin Light device emitting at a wavelength of 1.064 μm (Fotona Medical Lasers, Ljublijana, Slovenia). The laser beam was delivered in the contact mode perpendicular to the sample via a quartz fiber with a diameter of 300 μm. This laser system has a pulse length of 250 μs and a repetition rate of 5–10 Hz. The parameter settings used were 1 W and 10 Hz (Table 1).
CO2 laser (G4)
The equipment used for the CO2 laser surface treatment was a UM-L30 device emitting at a wavelength of 10.6 μm (Union Medical Engineering Co., Yangju-si, Gyeonggi-Do, Korea). The laser beam was delivered in the noncontact mode. The irradiation distance was 2.5 mm from the target site. The parameter settings used were 0.4W and 20 Hz (Table 1).
Preparation of appliances
Acrylic custom-made palatal devices were made with four sites (6×6×4 mm), and the enamel blocks were positioned and fixed with wax. The group distribution was randomized, and a new randomization scheme was performed for each volunteer. To allow plaque accumulation and to protect it from mechanical disturbance, a plastic mesh was fixed to the acrylic resin, leaving a 1 mm space above the surface of the enamel block (as described by Hara et al.) (Fig. 1). 27
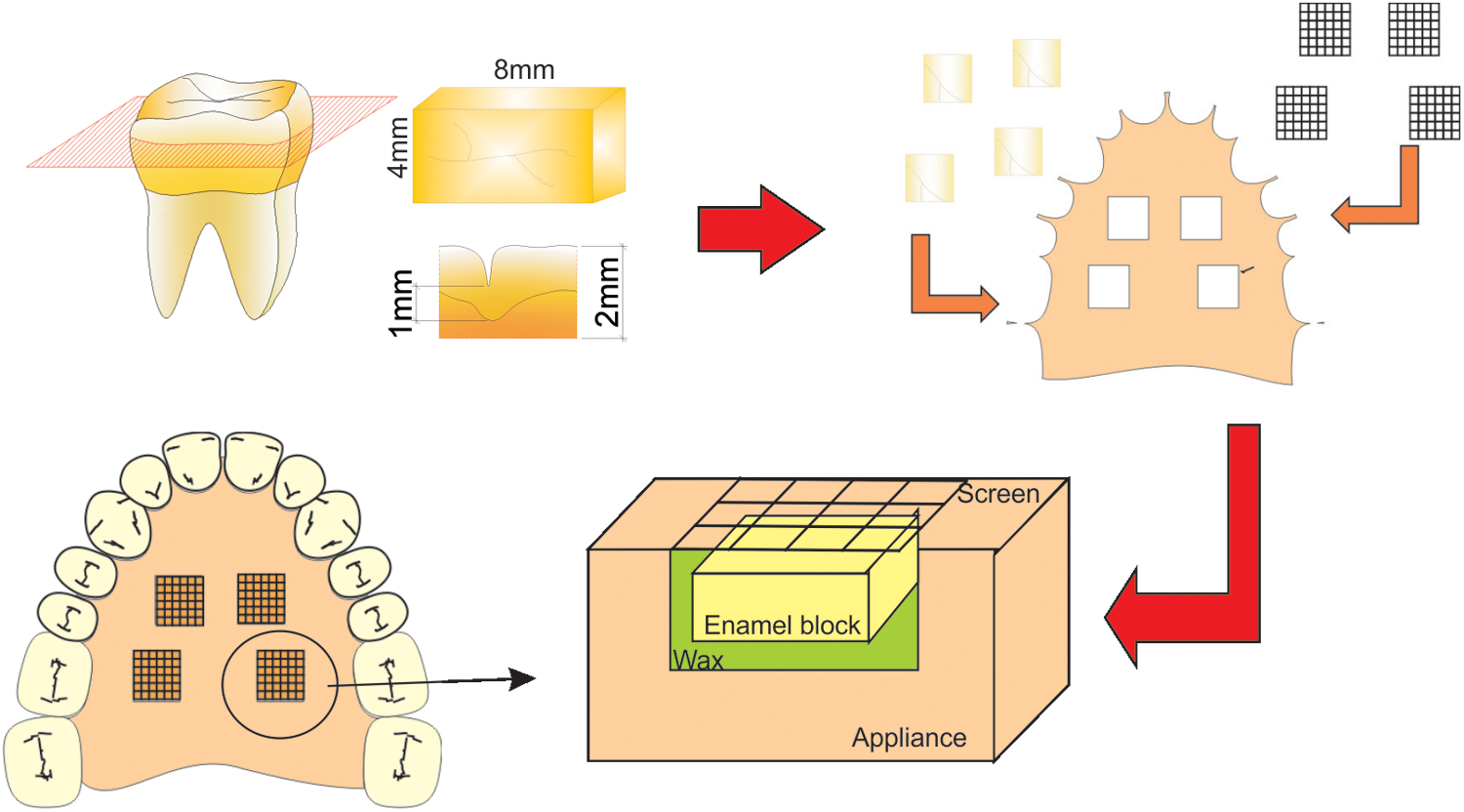
Preparation of appliances.
Intra-oral procedures
The volunteers followed a 1-week lead-in period before inserting the palatal devices. During this period and throughout the experimental phase, they brushed their teeth with a dentifrice containing fluoride (Colgate Máxima Proteção Anti-cáries, Colgate-Palmolive, São Paulo, Brasil). The cariogenic challenge to the specimens was provided by dripping a 20% sucrose solution onto all of the blocks; the blocks were kept in contact with the solution for 5 min before replacing the appliance in the mouth. 21 This procedure was performed six times per day during the 14 day study period with 120 min intervals between the applications. 28 Tooth brushing with the fluoride dentifrice was performed three times a day (after the main mealtimes). The volunteers were instructed to wear the intra-oral devices for the entire intra-oral phase, except while brushing and during meals. During the removal times, the devices were kept moist in boxes (provided to each volunteer).
Cross-sectional microhardness test
After intra oral procedures, the enamel blocks were removed from the appliances and cleaned in an ultrasound (3L, Dabi Atlante, Ribeirão Preto, SP, Brazil) for 15 min before being embedded in a polyester resin. They were then sectioned longitudinally through the center and polished with 600 and 1200 grit silicon carbide paper in a polishing machine (Buehler, Lake Bluff, IL) under water cooling and then with 0.3 and 0.05 μm alumina paste on the cloth. Next, the resin cylinders containing the blocks were ultrasonically cleaned and the cross-sectional Knoop microhardness was measured using a microdurometer (HMV-2000; Shimadzu Corporation, Kyoto, Japan) employing a 25 g load for 10 sec. Three rows of six indentations each were made: one in the central region of the dental enamel exposed and two 100 μm to either side of the central row. The indentations were made at 20, 30, 40, 50, 100, and 200 μm increments from the outer enamel surface at the bottom of the fissure. The three depth measurements were averaged.
PLM analysis
Thirteen samples from the remaining sections of each group were cut longitudinally using a diamond disc (Buehler Lake Bluff, IL) to obtain a ∼600 μm thick section. These sections were manually reduced with #1200 sandpaper under cooling conditions until an 80–100 μm thickness (per section) was obtained; each section was analyzed using PLM. The thickness for each section was measured with a 1 μm resolution micrometer (Mitotoyo, Tokyo, Japan). The cuts were soaked in 0.5 mL of deionized water and mounted on glass slides. The microscopic analysis was performed with a PLM and a crossed polarizer using an appropriate filter (Leica DMLB, Leica Microsystems, Nussloch GmbH, Germany). The images were captured at a 10× magnification and transferred to a computer through an integrated digital camera (Leica DC 300F, Leica Microsystems) with 100× final magnification.
For the lesion area measurements, the AxioVision LE 4.3 software was used (Carl Zeiss, Berlin, Germany). Because of differences in the depths of the fissures, the measurements were standardized considering a distance of 500 μm from the lower part of the fissure to the occlusal portion (Fig. 2). The assessment was done by previous calibrated evaluators and the examiners of the images were blinded.
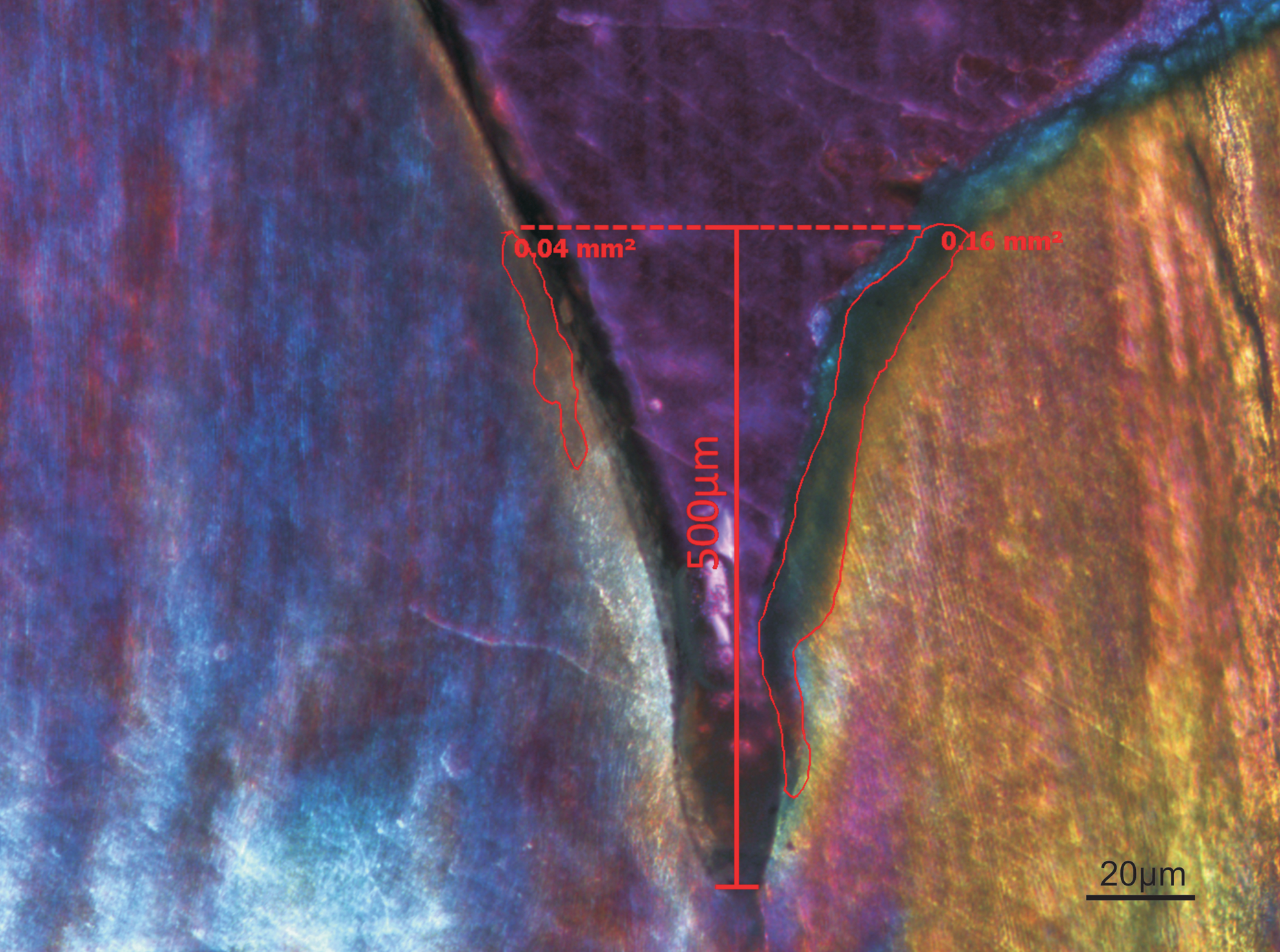
Standardization method for measurement of the demineralized area. A distance of 500 μm from the lower part of the fissure to the occlusal portion was considered (100×).
SEM analysis
Three sections from each group were analyzed by SEM. The sections were washed, immersed in water, and placed in an ultrasound using two 5-min cycles. Dehydration was performed using a series of ethanol solutions of 25%, 50%, and 75% potency for 20 min each, 95% potency for 30 min, and 100% potency for 60 min. The samples for each group were fixed on stubs using gold-plated metalized adhesive tape (SDC 050) with the treated surface turned upward for analysis. The SEM was used and operated at 20 kV (Phillips, XL30 FEGm Eindhoven, Holland). The specimens were observed at a 50× and 500× magnification, and the entire surface was scanned to observe the changes to the dental tissue.
Statistical analysis
All the data were verified by the Shapiro Wilk's test for the normality and Levene's test for the homogeneity; The data obtained from the analysis of the cross-sectional microhardness test were normal and homogeneous, a group comparison was performed using an analysis of variance. The sample mean differences were calculated using Fisher's least significant difference (LSD) test at a significance level of 5%. The lesion area measurement mean obtained through the PLM for each group was analyzed with the Wilcoxon nonparametric test at the 5% significance level to detect differences between the means. The analyses were performed with the ORING Pro 8 software (Origin Lab Corporation, Northampton, MA). The observation data from the SEM were not analyzed statistically, because the aim of the analysis was the qualitative comparison of the different experimental conditions proposed in the study.
Results
Table 2 shows the means of the cross-sectional microhardness test from each group. The specimens irradiated by the Nd:YAG (G3) and the CO2 (G4) lasers were statistically similar, and presented higher microhardness values than the control group (p<0.05). The group irradiated by the Er:YAG laser (G2) did not differ significantly from the control group (p>0.05).
Statistically significant differences were observed in the depth of the microhardness values for outer surface distances up to 50 μm. The lowest values were observed in measurements closer to the surface (20 μm<30 μm<40 μm<50 μm ∼100 μm ∼200 μm) (Fig. 3).
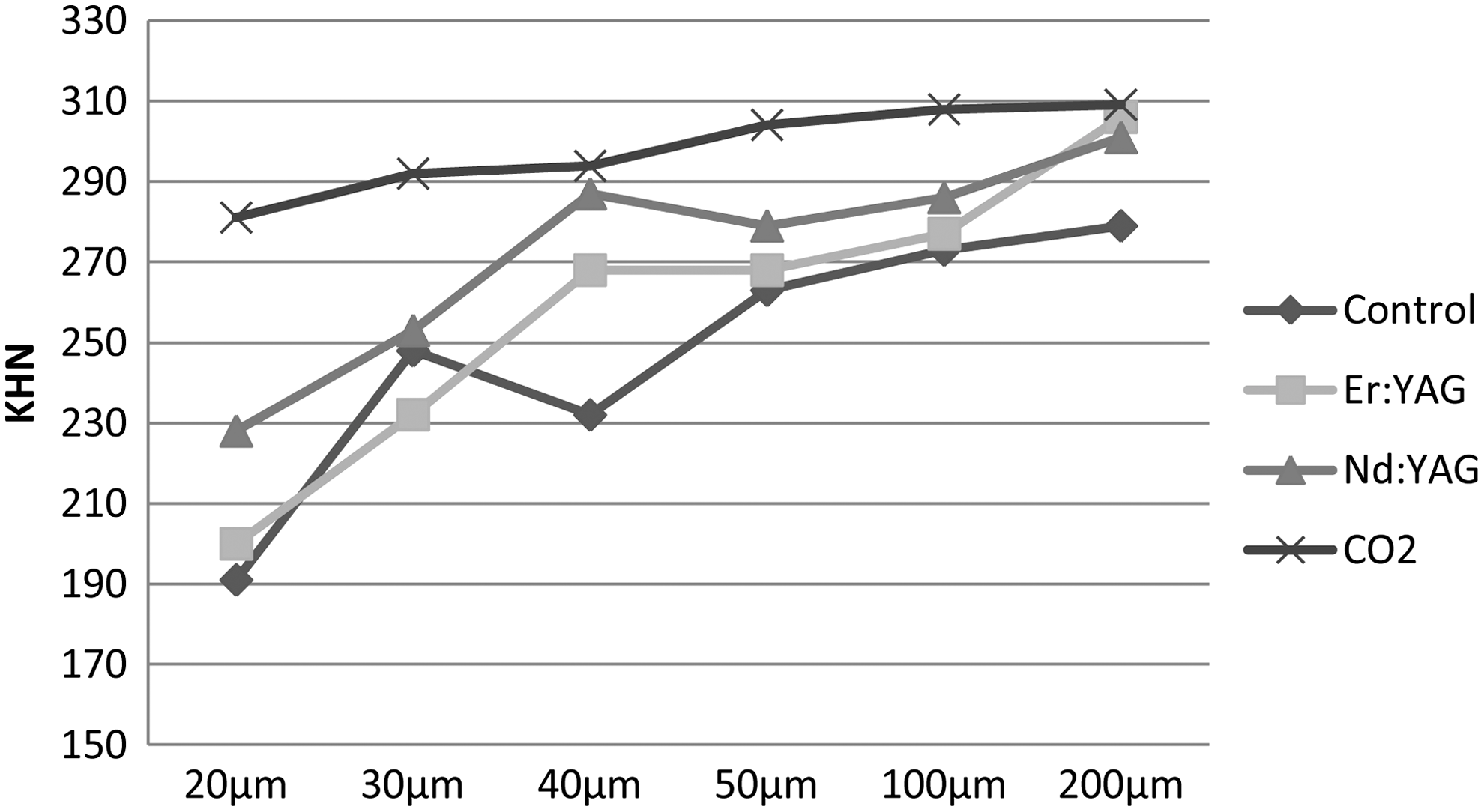
Means of cross-sectional microhardness test from each depth analyzed at each group (Knoop hardness number [KHN]).
In the lesion area analysis, statistically significant similarities were observed among all of the groups (p<0.05) (Table 3). Under PLM, the demineralized tissue appeared dark, whereas the healthy enamel had a yellowish or bluish color. Figure 3 shows representative PLM from each studied group. The control group showed a well-defined lesion area showing intense demineralization that swept through the deep fissure area. It was also possible to observe a surface layer that was more mineralized than the body of the lesion, which characterizes subsurface demineralization (Fig. 4A). The groups irradiated by the Nd:YAG and CO2 lasers did not present significantly demineralized areas (Fig. 4C and D).
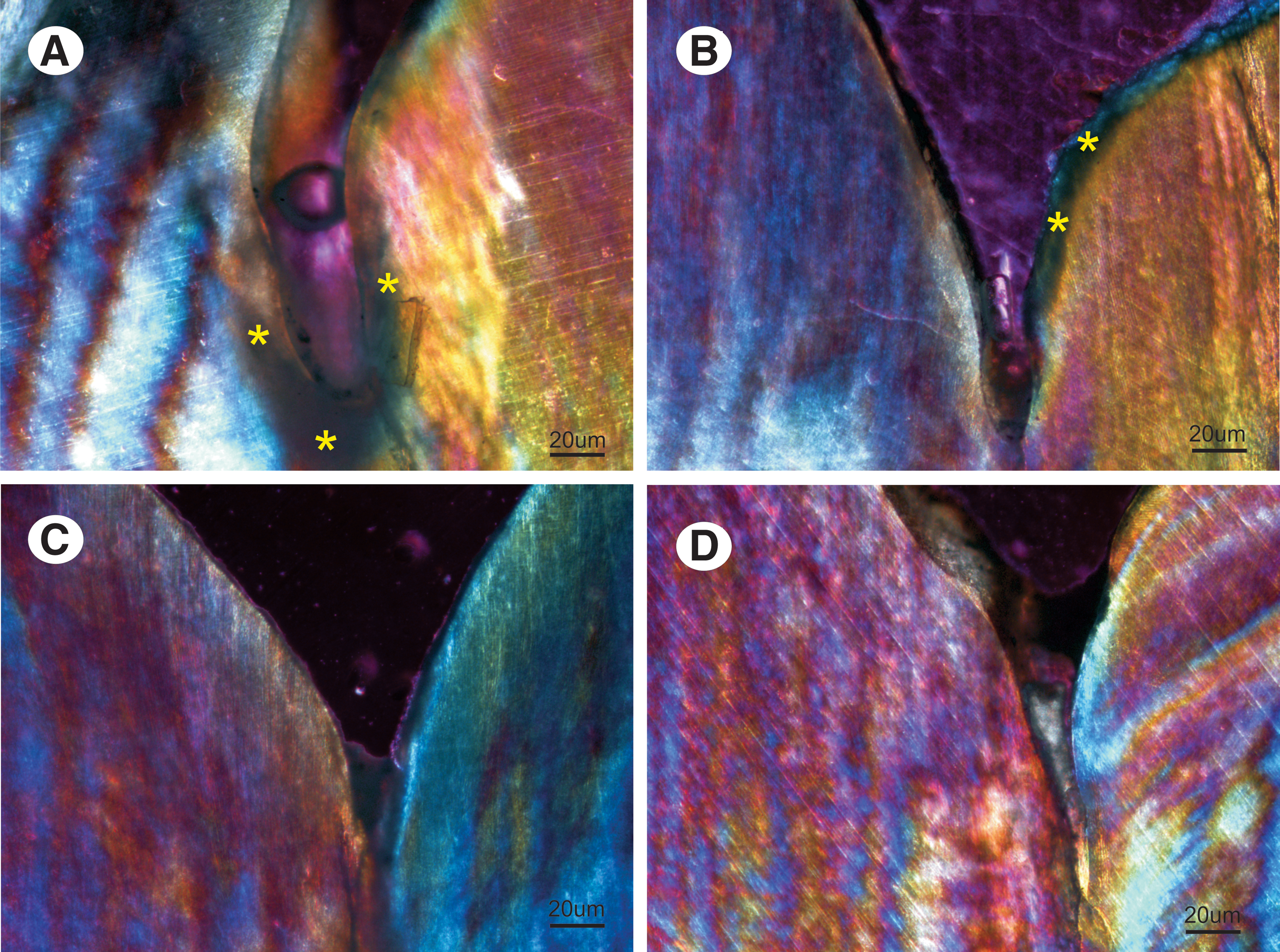
Photomicrograph representative of polarized light microscopy (PLM) analysis (100×).
Same letters indicate statistical similarity.
In the SEM analysis of the cross-sectional enamel, the control group showed demineralization through the length of the fissure, and a great disruption in the subsurface enamel (Fig. 5A and B). The group irradiated by the Er:YAG laser also showed demineralized areas through the length of the fissure, but some areas were intact. Moreover, when analyzed with a higher magnification, the tissue was characterized by demineralization (Fig. 5C and D). Groups 3 and 4 did not show any demineralization through the length of the fissure, and discrete disorganization was observed when a higher magnitude was used for the analysis (Fig. 5E–H).
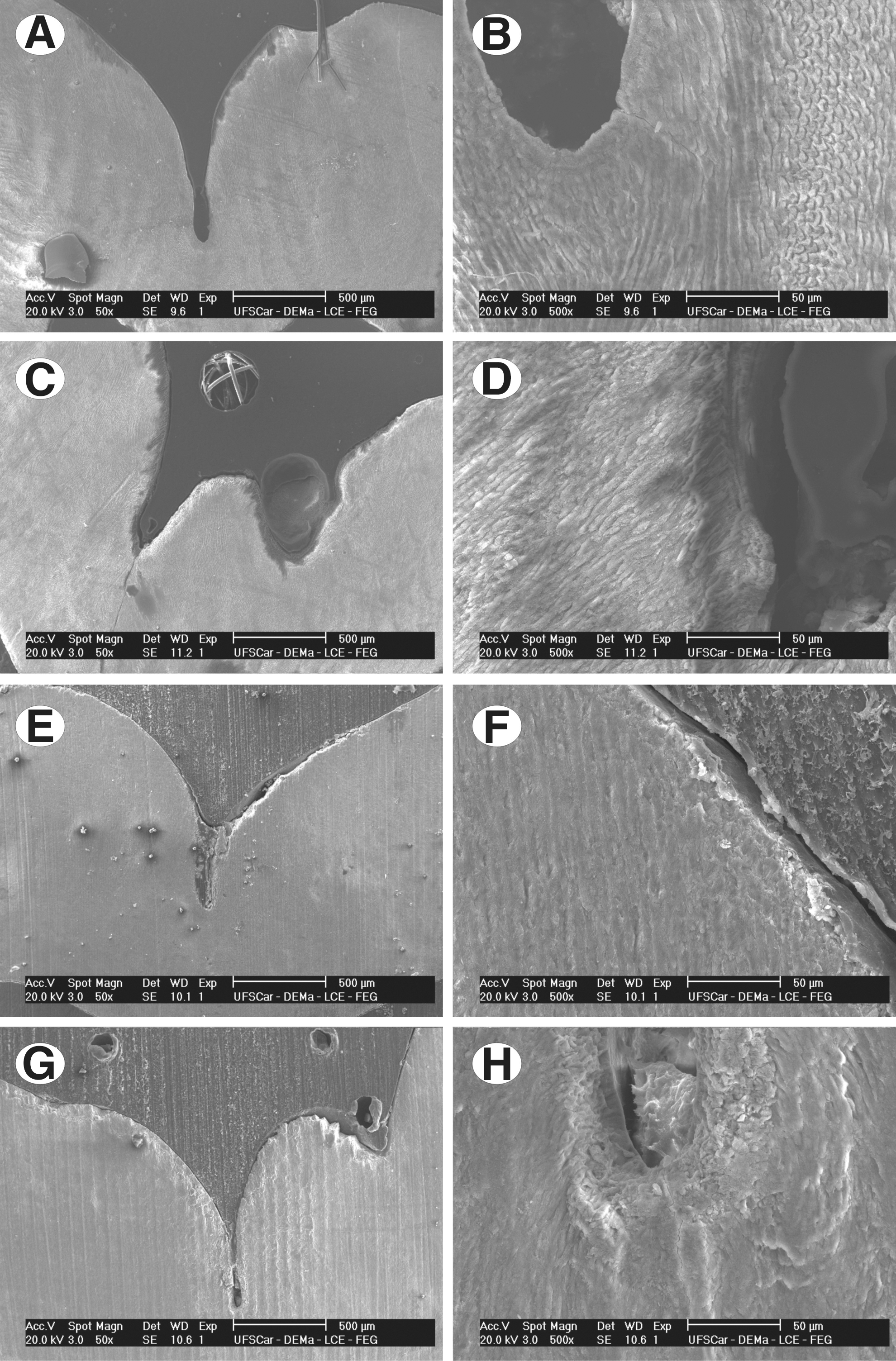
Photomicrograph representative of scanning electron microscopic (SEM) analysis.
When the Nd:YAG laser was used to irradiate the deep and narrow fissures, intense disorganization of the tissue at the bottom of the fissure was observed (Fig. 6).
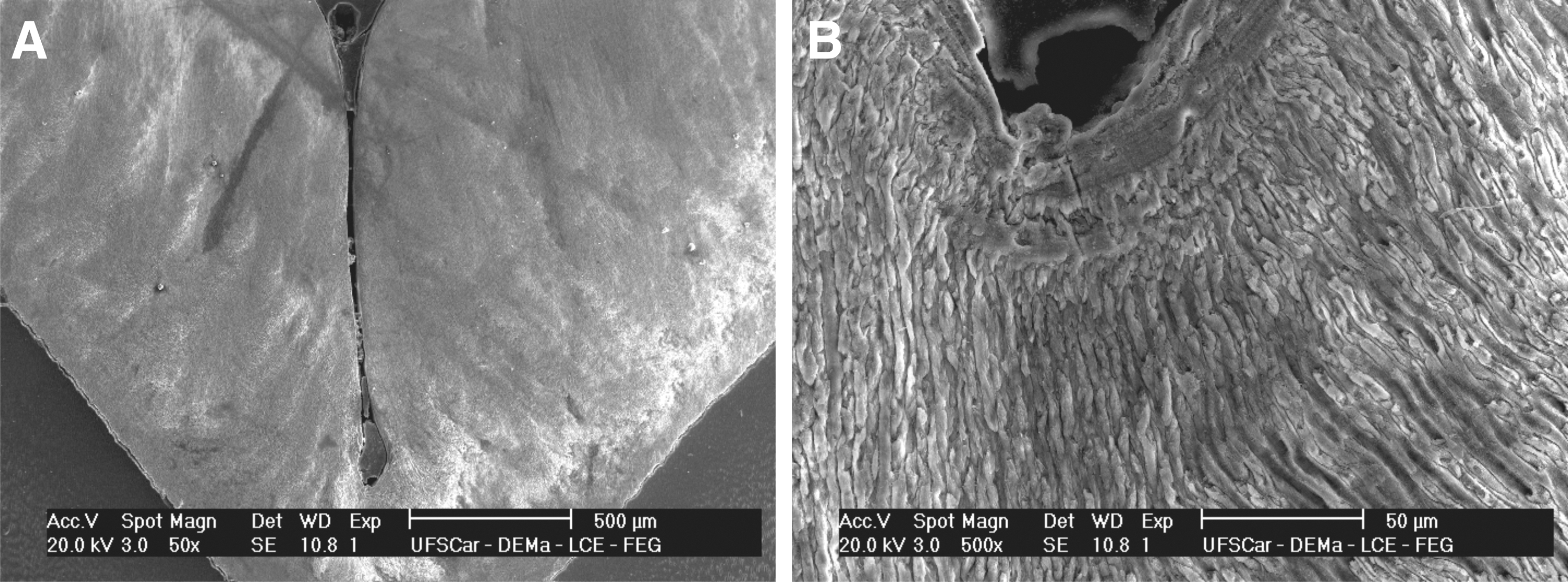
Fissure irradiated by Nd:YAG laser:
Discussion
For caries prevention on pits and fissures using low energy densities, this study tested three different types of lasers that emit in the infrared: (1) Er:YAG laser; (2) Nd:YAG laser; and (3) CO2 laser. The laser parameters used were an important factor of this study and aimed to promote chemical and structural alterations on the tooth surface without causing tissue ablation. It is difficult to compare the numerous reports of the effects of laser irradiation on human enamel because of the variety of lasers used, their different energy densities and wavelengths, and variations in the type of laser used. The selected parameters, for example, low energy densities, were based on previous studies 11,20,29,30 that demonstrated favorable outcomes of lased enamel in caries prevention.
High energy densities have also been used by past researchers in studies modifying the surface morphology of pits and fissures with laser irradiation. In an attempt to seal these areas, the high temperature increase promotes the fusion of the enamel followed by recrystallization. 31 –34 However, the areas of melting caused by laser irradiation are not homogeneous, 29 and Myaki et al. 33 observed in their study that the narrow and deep fissures did not have effective seals.
In addition, Fowler and Kuroda 35 reported changes in the enamel structure when it was subjected to temperature increases at specific bands. High temperatures promote microstructural surface changes such as melting with a glaze-like appearance, surface vaporization, carbonization of the collagen matrix, and re-solidified crystallization. These alterations could form new phases that are more soluble in acid. Therefore, although the researchers sealed the pits and fissures and obtained a beneficial change in relation to the surface morphology, an increase in the acid resistance of the surface enamel was not obtained.
Because of those factors, in the present study, the lasers were used in low energies to promote chemical and ultrastructural changes capable of increasing the resistance of the tissue to an acid dissolution. Some studies explored these changes on the smooth surface enamel, 18 –20 but only the CO2 11 and Nd:YAG 19 lasers were tested at low energies in the pits and fissures. Both in vitro studies concluded that the tested lasers have a potential clinical application for caries prevention of occlusal surfaces, obtaining a 30% higher acid resistance than that of the unlased controls. These past results are in agreement with the results of the present study, which found favorable results for the Nd:YAG and CO2 lasers for caries prevention in pits and fissures.
Past in situ studies of occlusal surfaces are scarce, but the methodology used in the present work was able to replicate real mouth conditions, and the caries lesions observed in the control group characteristically showed an outer layer that was relatively intact and porous with a mineral-rich area and some subsurface damage caused by the demineralization process from the dental biofilm (body of lesion). 36
Therefore, the formation of artificial caries obtained by the in situ methods provided a significant control area, allowing an assessment of the effectiveness of the methods used. High microhardness values were observed for the groups irradiated with the CO2 and Nd:YAG lasers (an increase in acid resistance on the pit and fissure surfaces). Mineral density differences were observed at different distances from the surfaces up to a distance of 50 μm, from which there were no more differences. These data likely result from the depth reached by demineralization. However, using PLM, similar results in the demineralized area were observed for all of the groups. This result could have been caused by the great variability of the volunteers, but it may also have been the result of the intense cariogenic challenge of correlating the effect of the other factors of caries disease in the control group.
Many past studies 37 –40 explored the effect of the CO2 laser on the enamel surface, and showed that with CO2 laser, pretreatment inhibited enamel demineralization by 17–98%, depending upon the laser beam type, the wavelength, the operational mode, and the energy output. These studies attribute the effectiveness of this method to energy absorption of the enamel during irradiation, which may promote alterations capable of decreasing tissue solubility. This theory is based on the fact that the CO2 laser wavelength is compatible with the absorption peak of carbonated hydroxyapatite, which is the major component of dental enamel (85%). 41 However, the Nd:YAG laser also presented favorable results for caries prevention in pits and fissures, but its wavelength is not close to the absorption bands of the components of dental hard tissues. It is believed that in contact mode, irradiation through a quartz fiber could cause heating at the surface that causes alterations and decreases enamel solubility. Despite the differences in methodology, the results of the present study are in agreement with other studies that used the same wavelength, employing low energy densities. 18 –20 Although the Nd:YAG irradiation showed positive results on the enamel surface, caries inhibition was observed only on the first course when this laser was used on narrow and deep fissures, because contact between the quartz fiber and the deep wall of the fissure was impossible, unlike the samples irradiated by the CO2 laser, which interacts via the light beam and possibly reached the bottom of the fissure even when it was narrow and deep.
Considering the parameters used in this study, an explanation for the obtained results could relate release of the carbonate present in the enamel when the tissue was heated. 42,43 In addition, the temperatures reached would also promote the condensation of acid ions and result in a structure that is more resistant to acid dissolution. 35
Carbonate can replace hydroxyl or phosphate/phosphate acid during crystal development. It has also been suggested that the centers of the crystals may be less well ordered, so that they accommodate carbonate as a result of screw dislocations in the direction of the c-axis substitutions. This happens because of a poorer fit of carbonate in the lattice, which generates a less stable and more acid-soluble apatite phase. 44 Robinson 44 has demonstrated a product from the enamel that is more soluble as compared than that generated from stoichiometric apatite. Carbonate substitution is probably the major reason for this finding. Moreover, classic research 45,46 reported a highly selective loss of magnesium and carbonate, which in the translucent zone, is considered to be the first discernible change in caries. This would be consistent with the notion that carbonate is associated with a more soluble mineral.
There may be an unintended benefit of the interaction between the laser irradiation and the organic matrix. 20,47,48 Dental caries involve two processes: the dissolution of the enamel structures and the diffusion of molecules and ions in and out of the enamel. 49,50 Therefore, the reduction of diffusion could be caused by the partial denaturation of the organic matrix blocking the diffusion pathways. Because the temperature necessary to induce protein decomposition is ∼350–400°C, a low energy density (0.3 J/cm2) may heat the enamel to a temperature <400°C. 37 Although the present study did not assess the organic matrix, the literature reveals that the parameters used may induce protein decomposition. At higher temperatures, the enamel diffusion channels are occupied by a macromolecular network of organic material, which may play a role in controlling enamel diffusion. 47
Although the Er:YAG laser has shown promising results by increasing the enamel acid resistance on smooth surfaces in previous studies, 16,20,30 the same behavior was not confirmed in the present study for the Er:YAG laser on occlusal surfaces. The explanation for this finding may be the use of cooling during group irradiation. 16,30 The irregularity of the occlusal surface could promote water buildup at the bottom of the fissures, and the necessary heating temperature was not reached for the chemical and ultrastructural alterations to occur at the surface. Therefore, the effectiveness and safety of the Er:YAG for caries prevention and tissue ablation is directly related to the adequate setting of the working patterns, including an optimum amount of water used during irradiation. 51
Given the results obtained and considering the methodologies used, the present study suggests that the CO2 and Nd:YAG lasers were able to increase the enamel acid resistance in pits and fissures. However, it is also clear that the effectiveness of this method and the other methods of caries prevention depend on the control of other factors related to caries disease; therefore, future clinical longitudinal studies should be conducted to verify the efficiency of this treatment.
Footnotes
Acknowledgments
The authors are grateful to Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP) (grants 06/ 05750-4) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (grant 483962/2007-4) for financial support.
Author Disclosure Statement
No competing financial interests exist.