
Abstract
Introduction
The skin is the body's external boundary in animals and humans. Among other things, the skin serves as a barrier against physical and chemical intrusions. 6 The skin also represents a barrier to applied physical energy from electrophysical agents (EPAs), which represent one of the four treatment pillars of physical therapy. 7
EPAs are used to treat tissue such as muscles, tendons, ligaments, and joint capsules. This makes the skin barrier of particular interest for research on EPAs. Variation characteristics in the biophysical ability to penetrate skin have direct implications for the dosing of LLLT in clinical settings. EPA therapy dosing has historically been based on clinical experience, rather than solid scientific evidence from basic research. 8
The skin's photoprotective properties, during epidermal light reflectance and melanocytes light absorption, avoid tissue injury caused by radiation from sunlight. 9,10 . The skin penetration characteristics of ultraviolet and visible light, are fairly well mapped in biophysical and dermatological literature. However, this literature provides only limited data about the penetration ability of the most commonly used infrared and near-infrared LLLT wavelengths in clinical settings.
Biophysically, the ability of lasers to penetrate tissue is dependent upon the laser's wavelength. Light with a wavelength range of 700–1000 nm is infrared and invisible, and penetrates tissue better than light in the red wavelengths (600–700 nm). 11 Clinically, laser irradiation in skin flaps has shown that penetration increases linearly with wavelengths from 450 nm to 1030 nm. 12 This was further supported by results from a study of two different red laser wavelengths in human skin flaps, which showed that a wavelength of 675 nm penetrated better than did a wavelength of 632.8 nm. 13 Other studies have reported similar findings with wavelength-dependent penetration in animal tissue. 14 These results correlate well with another study showing that a greater amount of energy penetrated rabbit skin with a wavelength of 904 nm, than with a red wavelength of 632.8 nm. 15
In a systematic review of LLLT studies on lateral epicondyle tendinopathies, Bjordal et al. 3 found effective doses from superpulsed 904 nm lasers to be significantly lower than effective doses from 632.8 nm lasers. Guidelines from World Association for Laser Therapy (WALT) have also differentiated between wavelengths. Typically, WALT recommends doses that are twice as high for lasers within the 780–860 nm wavelength range, than for lasers with a wavelength of 904 nm. 16 WALT guidelines doses are derived from some 160 published randomized controlled LLLT trials. The difference in energy dose can only partly be explained by wavelength, which typically accounts for <20% of the penetration difference. 12 However, a satisfactory causal understanding of the need for differentiated dosing is still lacking. An aspect other than wavelength dependency is the mode of operating the laser. GaAs lasers with 904 nm wavelength operate with strong, short pulses (peak power 10–100 W) in a superpulsed mode with nanosecond or picosecond pulse durations, whereas 780–860 nm GaAlAs lasers typically operate in a continuous mode or with chopped pulses (peak power <0.5 W). This feature has not been extensively addressed in the LLLT literature, and few studies have compared continuous with pulsed and superpulsed irradiation. In a recent article, Hamblin et al. 17 searched the literature for possible differences in therapeutic effects between those of continuous and pulsed laser irradiation. Their conclusion was that pulsed irradiation mode seems to be superior to continuous mode. However, this result could also be caused by differences in laser parameters other than irradiation modes, as no head-to-head comparisons were performed with equal doses. Moriyama et al. 18 compared superpulsed with continuous irradiation mode from 905 nm lasers in acute knee inflammation in mice induced by Zymosan-A, and found more pronounced upregulation of inducible nitric oxide synthase (iNOS) from superpulsed irradiation mode. They suggested that inflammatory pathway responses were activated by different mechanisms in superpulsed and continuous irradiation modes.
The few existing LLLT studies that deal with penetration issues have focused either on energy loss 19,20 or on penetration depth. 13,15 In LLLT treatment, an irradiation dose is typically administered during periods lasting from 20 to 30 sec up to a few minutes. No studies have yet investigated the time-profiles for skin penetration of energy from LLLT devices. With this perspective, we decided to perform a study with two commonly used lasers in LLLT.
Aim
The aim of this study was to investigate the rat skin penetration abilities of two commercially available LLLT lasers during 150 sec of exposure.
Materials and Methods
Materials
Thirty-four matured male Sprague–Dawley rats weighing 250–300 g were housed with 3–4 animals together in individually ventilated cages. Light cycles were kept at 12+/12− h, with water and food ad libitum. The animals were then euthanized and 62 skin flaps (n=62) overlaying the gastrocnemius muscles on the hind legs were successfully dissected free and irradiated within 3 min after euthanization. Six skin flaps were discarded because of human errors in the dissection procedure.
Instruments
The laser MOP was measured with an Optical Power Meter System (Thorlabs Instruments, U.K.). The Optical Power Meter System consists of a PM100 Display unit with sample rate of 6 Hz and accuracy of±1%, and a S121B silicon sensor. The S121B sensor input had an aperture with diameter of O=9.5 mm with an optical power range 500 nW–500 mW and an accuracy of±5% (manufacturer's specification).
Two commercially available therapeutic lasers were used for laser irradiation: (1) 810 nm wavelength laser (Thor-DD, U.K.), operated in a continuous mode with MOP of 200 mW, spot size 0.0314 cm2, and power density of 6.37 W/cm2 (manufacturer's specification); and (2) 904 nm wavelength laser (Irradia, Sweden) operated in a superpulsed mode: Peak power 20 W, superpulsed width 100 ns (10−9 sec) with a frequency of 6 kHz; and 60 mW MOP, spot size 0.0364 cm2, and power density 1.67 W/cm2 (manufacturer's specification).
Experimental procedure, part 1
Step one: energy output measured directly
The two lasers were tested for MOP during 150 sec of exposure with no obstacles between the laser source and the Optical Power Meter.
Step two: energy output measured after penetrating a plastic film
The two lasers were tested for MOP during 150 sec of exposure with a transparent plastic film between the laser source and the Optical Power Meter.
Step three: energy output measured after penetrating freshly harvested rat skin flaps. with the probe in skin contact
The animal was put into gas anesthesia (isoflurane, Isoba), and then given 0.4 mL intraperitoneal anesthesia (Mebumal 50 mg/mL). Hair was shaved from both hind legs.
Experimental procedure, part 2
Animals were then euthanized by cardiac arrest from a 1 mL saturated potassium chloride solution.
The skin overlaying the gastrocnemius muscle was then dissected free: distally from calcaneus, anteriolateral and anteriomedial of the edge of the gastrocnemius muscle, and proximal to the gastrocnemius muscle (Fig. 1).

A skin flap, consisting of skin overlaying the gastrocnemius muscle.
The Optical Power Meter System was tuned to the same wavelengths as the respective test lasers.
All skin flaps were then irradiated in a sequential manner with increasing exposure times for each laser.
For every skin flap the measurement procedure started with registering the lasers' MOP directly into the Optical Power Meter. A plastic film was then placed over the sensor. The skin flap was then placed on the plastic film and the laser MOP was registered. During the exposure, the laser probe was in full skin contact for 150 sec. The laser probe was held in skin contact with slight pressure necessary to maintain the probe in a fixed position. The therapist sought to apply the same amount of pressure for all skin flaps. Laser penetration through the skin plus plastic film was registered at seven time points; immediately after being activated, after 10 sec, after 30 sec, and then every 30 sec up to 150 sec.
Step four (same procedure as in step three, but with the probe not in skin contact)
The laser probe was now kept ∼1 mm from the skin during LLLT irradiation.
Main outcome measure
The power was measured in mW without obstacles after penetration through air, plastic film, and rat skin flap, and as a percentage of the measured nominal MOP.
Statistical analysis
Statistical differences were calculated by Statistical Package for the Social Sciences (SPSS, v.19) using repeated measures ANOVA, generalized estimating equations(GEE), for the whole sequence (measurements at 10 sec are omitted in these calculations). Microsoft Excel (Microsoft Office Excel 2007) was used for statistical descriptive analysis, Student's t-test p-value significant differences, and graphs.
Ethical approval
This study was approved by the local animal laboratory committee at the University of Bergen, Norway (Appl. No. 20102676).
Results
Step one (no obstacle, through air only)
The MOP from both lasers were stable during 150 sec of exposure. The 904 nm laser increased MOP by 0.3 mW (SEM±0.4), whereas the 810 nm laser reduced MOP by 9.8 mW (SEM±1.9) by the end of 150 sec of exposure (Table 1). The statistic GEE estimated a slope of 0.25 mW per 30 sec (95%CI: 0.07 to 0.42, p<0.01) for the 904 nm laser; and a slope of −1.14 mW per 30 sec (95%CI: −1.44 to −0.84, p<0.01) for the 810 nm laser.
The mean energy output from two commercial LLLT-lasers, during 150 sec of irradiation: direct into an Optical Power Meter, through plastic film, and through plastic film plus skin (with the LLLT-probe in skin contact and not in skin contact).
LLLT, low-level laser therapy; MOP, mean output powers.
Step two (through plastic film)
The plastic film reduced MOP by 3.6%, or 2.3 mW (SEM±1.2), on average from the 904 nm laser; and by 6.6%, or 12.7 mW (SEM±1.0), on average from the 810 nm laser (Table 1). The statistic GEE estimated a slope of 0.16 mW per 30 sec (95%CI: −0.10 to 0.42, p=0.23) for the 904 nm laser; and a slope of −1.00 mW per 30 sec (95%CI: −1.49 to −0.52, p<0.01) for the 810 nm laser.
Step three (through skin, probe in skin contact)
The two lasers had statistically different skin penetration abilities. The percentage of energy penetrating skin from the 810 nm laser was stable at ∼ 20% of MOP (ranging from 19.5% [SEM±0.6] to 20.4% [SEM±0.6]) during the exposure period (Table 1). The statistic GEE estimated slope was −0.26% of MOP per 30 sec (95%CI: −0.35 to −0.17, p<0.01), whereas the percentage of energy penetrating skin from the 904 nm laser increased almost linearly during the exposure period, from 38.7% of MOP (SEM±1.4) to 58% of MOP (SEM±3.5) (Table 1). The statistic GEE estimated slope was 2.29% per 30 sec (95%CI: 1.69 to 2.88, p<0.01) for the 904 nm laser.
Comparing the percentage of MOP penetrating skin from the two lasers, there were significant (t-test, p<0.01) differences at all measured time points (Table 1 and Fig. 2).
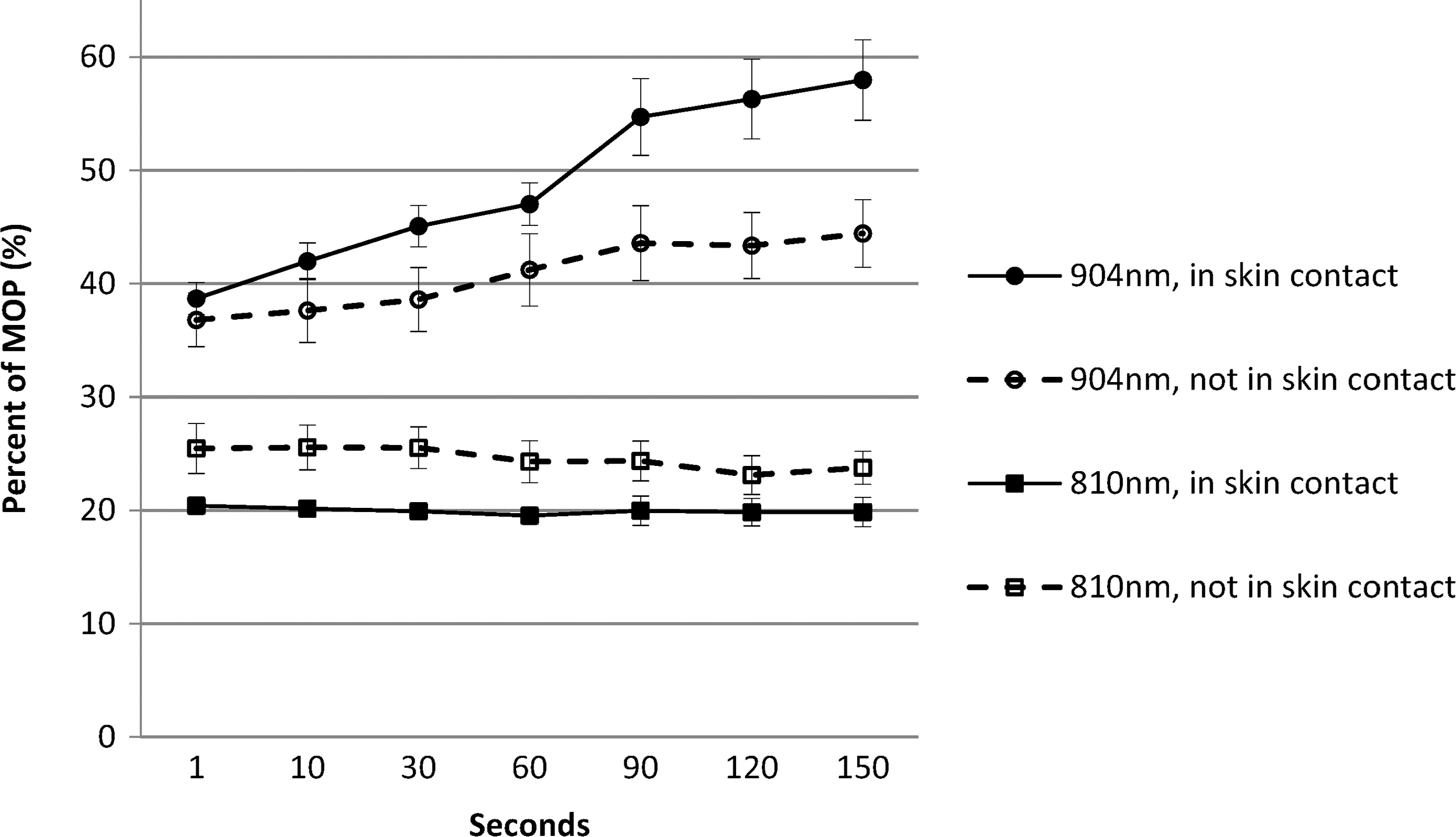
Percentage of mean output powers (MOP) (±SEM) penetrating skin during 150 sec of irradiation, from the 904 nm (60 mW, superpulsed) laser and the 810 nm (200 mW, continuous) laser. Data are represented with the laser probe in skin contact and not in skin contact.
Step four (through skin, probe not in skin contact)
Both lasers showed the same trends of energy penetrating skin as was the case with the laser probes in skin contact. There were significant (t-test, p<0.01) differences in percentage of MOP penetrating skin from the two lasers at all measured time points (Table 1), even though the slope of increased penetration during processing time from the 904 nm laser was smaller than with the probe in skin contact. The statistic GEE estimates a slope of 1.42% of MOP per 30 sec (95%CI: 0.82 to 2.03, p<0.01) with the probe not in skin contact. In percentages, the amount of energy penetrating skin increased from 36.8% (SEM±2.4) to 44.4% (SEM±3.0) during exposure (Table 1 and Fig. 2).
In skin contact versus not in skin contact and probe's shape
For the 810 nm laser, the amount of energy penetrating the skin was slightly higher during irradiation than with the probe in skin contact: The percentage of MOP was ∼24% (ranging from 23.1% [SEM±1.7] to 25.5% [SEM±2.2]) during the exposure period with the probe not in skin contact (Table 1 and Fig. 2).
The statistic GEE estimated slope was −0.42% of MOP per 30 sec (95%CI: −1.27 to 0.43, p=0.33).
Irradiation with the laser probe in skin contact versus not in skin contact resulted in a change in skin penetration for both lasers. This change was most likely not attributed to laser parameters, but to the different physical shape of the two probe tips. The 904 nm laser probe has a protruding convex lens, which squeezes the skin when the probe is in skin contact. This will cause better penetration with full skin contact than with no skin contact. On the other hand, the 810 nm laser probe has a recessed flat window. Here, the metallic ring surrounding the lens will push skin underneath the lens, which leads to less penetration with the probe in skin contact than not in skin contact (Fig. 3).

Laser probe tip, the 904 nm laser with a protruding lens (left), and the 810 nm laser with a folded up lens (right).
Discussion
The skin barrier has been a major obstacle for EPAs since they were introduced in the treatment of tissue pathology. 21 Questions such as how deep can different energy forms penetrate into the body, and what happens in terms of energy loss in this process has intrigued researchers for decades. LLLT has poor penetration ability when compared with other energy forms such as electromagnetic and ultrasound radiation. Nonetheless, it is important to emphasize that the current study demonstrates that between 20 and 58% of the energy delivered to the skin surface is penetrating the rat skin barrier during LLLT irradiation. The important conclusion is therefore that this residual energy should be more than enough to reach the dose threshold for stimulating physiological and tissue repair processes.
The first two steps of the experimental procedure developed as expected, showing that both lasers delivered stable MOP, and that energy loss in a plastic film was negligible and stable. The time-profiles for skin penetration, during 150 sec of exposure, were, however, distinctly different for the two lasers. For the 810 nm continuous laser, the penetration ability stayed at the same level during 150 sec of exposure, whereas the penetration from the 904 nm superpulsed laser increased in an almost linear manner during 150 sec of exposure. The higher skin penetration ability of the 904 nm superpulsed laser increased from +18% initially to +28% at 150 sec of exposure. This time-profile of increased skin penetration ability during exposure time has, to our knowledge, never been demonstrated before. The pronounced differences cannot be explained by different wavelengths alone. According to studies investigating the ability of different wavelengths in light to penetrate skin, a difference of 10 22 to 15%, 23 could be expected between the wavelengths 800 nm and 900 nm. This leads us to speculate that the irradiation mode is the most likely source for the observed differences in skin penetration. It has previously been suggested that strong pulses may cause a photobleaching effect in the skin barrier over time. 24
In the research for identification of possible LLLT dose-response patterns, we suggested already in 2001 that the different laser wavelengths and irradiation modes should be classified in different categories. 25 At that time, the differentiation was governed more by minimizing uncertainty than by solid evidence for these possible differences.
Our current findings contributes to a plausible explanation for different effective doses from 904 nm and 780–860 nm lasers, found in clinical studies and reflected in WALT guidelines.
16
It can be illustrated by an example with two 60 mW MOP lasers, that WALT recommendations of twice as high doses for 810 nm lasers than for 904 nm lasers, as they result in approximately equal amount of energy penetrating the skin. A dose of 4 J from an 810 nm, 60 mW, continuous laser, takes 67 sec to deliver. The skin penetration rate with the probe in skin contact is 20%. The cumulated amount of energy penetrating skin is 0.8 J (=20%×0.06 W×67 sec). The delivering of a 2 J dose from a 904 nm, 60 mW, superpulsed laser, takes 33 sec. With the probe in skin contact, skin penetration increase linearly from 38 to 45% during 30 sec of exposure (percentages are in accordance with Table 1). The amount of energy penetrating skin cumulates to 0.82 J
In line with our currently demonstrated skin penetration profile, Castano et al. 26 found long processing time from superpulsed 810 nm lasers to be more effective than short processing time in inflammatory rat knee arthritis. In Castano's study, all other irradiation parameters were held equal.
In a study with LLLT intervention in induced arthritis in mouse knees, Moriyama et al. 18 found irradiation mode to activate iNOS expression differently. They suggested different mechanisms in activating the inflammatory pathway response as an explanation to the significant differences found between superpulsed and continuous irradiation mode from 905 nm lasers. In perspective of our current findings, the amount of energy penetrating skin from superpulsed lasers is more than double the amount of energy from continuous lasers, during 200 sec of exposure. These circumstances could as well be part of the given reason.
This skin penetration profile, with a linear increase in amount of energy passing skin during an irradiated dose from the superpulsed laser, points out processing time as an interesting parameter in LLLT with superpulsed lasers.
In most clinical studies on animals, LLLT irradiation is initiated hours after an injury or injection. In Moriyama's study with increased inflammatory reactions in mouse knees after LLLT, the treatment from a superpulsed laser was 15 min after induced inflammation. Similarly, we found increased edema in rat Achilles tendon treated with 3 J from a superpulsed laser within 30 min after a blunt trauma. 27 Whether these increased inflammatory reactions are caused by too early irradiation after induced injury, or whether the amount of energy penetrating the skin gave a too high dose, is unclear. We need further research on initiation of irradiation and influence of irradiation mode to answer those questions.
Conclusions
In clinical practice, the different skin penetration profiles for superpulsed and continuous lasers will have some clinical implications. In addition to different optimal doses as reflected in WALT guidelines, the penetration profile influences skin temperature during LLLT treatment. We found lower thermal effects in dark skin from 904 nm superpulsed laser than from 810 nm continuous laser in one of our earlier studys. 28 This difference in thermal effects from these two lasers can be explained by skin penetration profile. The percentage of energy absorbed in skin during processing time is decreased for superpulsed lasers, whereas it is constant for continuous lasers. In addition, 904 nm superpulsed lasers have better skin penetration initially than do 810 nm continuous lasers (Fig. 2).
Other critical features with the lasers, which are outside the scope of this study, are to what degree output power (peak value), power density (mW/cm2), and spot size (cm2) influence skin penetration.
Other important questions, are “What happens to the skin during LLLT irradiation?” and “Are results from lasers' rat skin penetration applicable to humans?” Few LLLT-studies are concerned with sequelae in the skin during irradiation aiming at tissues beneath the skin. This might be because of the absence of side effects such as skin damage or ablation from LLLT treatment. 3 To the latter issue, the photoacceptor processes from irradiation by near infrared light are believed to be the same in all mammalian cells, catalyzed by cytochrome c oxidase. 29 Stratum corneum and skin thickness in both rats 30 and humans 31 differs with body site. Most irradiation of the skin is absorbed or scattered in stratum corneum of epidermis, 32 and there is considerable similarity in this skin layer thickness between rats 30 and humans. 31 On the other hand, within the research areas of photodynamic therapy and drug metabolisms, the degree of skin permeability and percutaneous absorption differs between rats and humans. 33 –36 Further histology investigations after single and repeated LLLT irradiation of rat and human skin flaps are recommended to elucidate if the observed changes over time in 904 nm penetration are irreversible or permanent.
Footnotes
Author Disclosure Statement
No competing financial interests exist.