
Abstract
Introduction
Several solutions are commonly used for root canal irrigation. Sodium hypochlorite (NaOCl) is often used, but it does not remove the smear layer and is very toxic to periapical tissues, especially when used at high concentrations. 4,5 Chlorhexidine gluconate (CHX) is an effective oral antimicrobial agent but it is not an effective tissue solvent, which means that debris can remain. 6 Demineralizing agents such as ethylenediaminetetraacetic acid (EDTA) have been recommended as adjuvants in root canal therapy. EDTA is highly biocompatible and shows high efficiency in removing the smear layer; however, it is not antibacterial. 7
The instrumentation of root canals causes the formation of a smear layer on the surface of root canal walls. 8 This residual smear layer is believed to prevent bacterial penetration and colonization of the dentinal tubules. 9 Recent studies report that removal of the smear layer may reduce the adhesion of some sealers and penetration of sealers into the dentinal tubules. 10,11 The presence of a smear layer negatively affects the adhesive properties of materials and in turn promotes bacterial penetration along different root canal fillings. 12
The primary goals of endodontic treatment should be to disinfect the root canal and to prevent re-infection. 13 Coronal leakage of the root filling, in which the opened root canal entrance, filled with gutta-percha, is exposed to oral flora, is one of the factors resulting in unsuccessful root canal treatments. In addition, bacteria play a significant role in endodontic treatment. Therefore, the long-term prognosis depends upon the quality of the final restoration. 14 A newer natural product has recently been introduced in dentistry as an anticaries and antiplaque agent, for pulp capping, 15 and for the prevention of oral diseases. 16 This is propolis, a flavonoid-rich resin made by the honeybee. The chemical composition of propolis is very complex, consisting of pollen, resins, waxes, and flavonoids, and its content varies widely, depending on location, climate, year, and season. 17,18
The use of lasers developed for dentistry has also been suggested in recent years as a way to reduce microleakage. 19 The insufficient bactericidal penetration of irrigation solutions means that microorganisms in the deep layers of dentin are unaffected. 20 Noninstrumentation techniques, such as laser technology, can cleanse all of the different infected parts of the root canal system. 21,22 The potassium-titanyl-phosphate (KTP) laser, which emits a 532 nm wavelength that is half the intensity of the Nd:YAG laser, has been introduced mainly for tooth-bleaching procedures in dentistry. 23,24 Previous studies have demonstrated that the KTP laser could achieve complete removal of the smear layer from root canal walls. Nevertheless, higher energy densities led to thermal damage. 23,25,26
The purpose of the present study was to compare the effects of propolis, KTP laser treatment, and different irrigation solutions on coronal bacterial leakage from root canals obturated with gutta-percha and AH-26 root canal sealer.
Materials and Methods
Preparation of teeth
A sample of 120 single-rooted human mandibular premolar teeth with single canals was used for the study. Teeth that were extracted for orthodontic or periodontal reasons were used. Teeth were inspected for cracks or resorption fields with a light microscope (Nikon SMZ 800, Nikon Corporation, Tokyo, Japan) at×5 magnification. The surfaces of each root were cleaned with a Gracey curette. After extraction, the teeth were stored in 0.9% physiological saline solution at +4 °C until required. The crowns were removed at the level of the cementoenamel junction with a low speed diamond disk to obtain specimens of similar lengths.
Preparation of propolis extract
Thirty grams of propolis (Trabzon Agricultural Development Cooperative) was dissolved in 60 mL dimethyl sulfoxide (DMSO) by mixing. To give the best results of the dissolution, the mixture was left in a magnetic mixer (Braun, Melsungen AG-Germany) for 24 h at 37 °C, and then coarse pieces were removed by filtration. Sterile saline was added to achieve a 20% concentration of propolis.
Canal instrumentation
The resulting root lengths of all specimens were between 12 and 18 mm. The pulp tissues were removed with barbed broaches. A #15 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was inserted into the root canal until it appeared at the apical foramen. The working length of each root canal was determined by subtracting 1.0 mm from this length. The anatomic diameter of the root canal at the apex was equivalent to that of a #15 file for all teeth used.
The root canals were prepared by Dentaport Root ZX (J. Morita Co., Kyoto, Japan) and ProTaper (Dentsply Maillefer, Ballaigues, Switzerland) rotary instruments using the crown-down technique according to the manufacturer's instructions. S1 files were used for two thirds of the working length, SX files were used until resistance was felt, and S1, S2, F1, F2, and F3 files were used to the working length. A #15 K-file was inserted at the working length between each file for the purpose of preventing apical blockage.
Experimental groups
The specimens were randomly divided into the following five groups of 20 teeth each:
Group l
After the use of each file, the root canal was irrigated with 1 mL of distilled water, and then a final irrigation was accomplished with 2 mL of 17% EDTA for 2 min each.
Group ll
After the use of each file, the root canal was irrigated with 1 mL of distilled water. At the end of the instrumentation, the roots were finally irrigated with a 2 mL rinse of 20% propolis solution for 2 min each.
Group lll
After the use of each file, the root canal was irrigated with 1 mL of 2.5% sodium hypochlorite. A total volume of 7 mL of 2.5% NaOCl was used for irrigating root canals for each tooth.
Group lV
After the use of each file, the root canal was irrigated with 1 mL of distilled water. At the end of the instrumentation, the roots were finally irrigated with a 2 mL rinse of 2% CHX for 2 min each.
Group V
After the use of each file, the root canal was irrigated with 1 mL of distilled water. The root canals were irradiated in pulse mode at 1.5 W, 250 mJ/cm2 with a KTP laser (SMARTLITE D, Deka, Calenzano Firenze, Italy). The 200-μm fiber optic tip was inserted into the root canal 1 mm shorter than the working length. The laser was applied and gently withdrawn, from the root apex to the coronal end, with a rotational movement for 2.5 sec four times with 30 sec recovery intervals in between each laser dose. After the root canals were dried, laser application was performed.
Control groups
The 20 teeth used as controls—10 positive and 10 negative controls—were irrigated with distilled water. In the negative control group, to confirm that there was no leakage except in the tooth, the coronal part of the tooth was also covered with nail varnish. In the positive control group, to show that there was leakage only with a root canal, the root canal was filled without root canal sealer, and the apical foramen was not covered with nail varnish.
Canal obturation
The root canals were blotted with paper points (Dentsply Maillefer). The AH-26 (Dentsply, DeTrey, Konstanz, Germany) root canal sealer was mixed according to the manufacturer's instructions. The canals were obturated with cold lateral compaction of gutta- percha and AH-26. Root filling material was removed at a depth of 1 mm under the level of the cementoenamel junction. The coronal orifice of each tooth was filled with a sterilized cotton pellet and temporary filling material (Fermin, Detax Dental, Karlsruhe, Germany).
All teeth were stored at 37 °C and 100% humidity for 1 week for the sealer to set.
Bacterial leakage experiment
The external surfaces of the specimens, except for the coronal opening and the apical 2 mm, were covered with three layers of nail varnish. Thereafter, the temporary filling material and cotton pellet were removed.
The teeth were inserted into 4 mm ends of cut off Eppendorf plastic tubes (Eppendorf-Elkay, Shrewsbury, MA), with the apical portion of the specimen protruding through the tube. The gap between the tube and specimen was tightly sealed with acrylic resin and cyanoacrylate glue. All specimens were then sterilized using ethylene oxide gas.
The specimens were suspended in sterilized flasks containing 3 mL of Brain Heart Infusion Broth (BHIB) to a level of 7–8 mm above the apical foramen of each root. Around the input of the flask, cyanoacrylate glue and acrylic resin were applied, except at the entrance of the Eppendorf tube. This two-chamber model was described by Torabinejad et al., 14 as modified by Imura et al. 27 (Fig. 1).

The two chamber bacterial leakage test model.
The upper chambers were inoculated with 0.5 mL of BHIB containing Enterococcus faecalis at 108 colony-forming units (CFU)/mL. All specimens were kept at 37°C and the bacterial broth in the upper chamber was replenished with fresh inoculated medium every 5 days, for a total of 30 days, to verify bacterial viability. The bottom chambers were checked daily for 1 month for the occurrence of turbidity, which would indicate bacterial growth. The day that the turbidity occurred in the bottom chamber was recorded and the turbid material was cultured on blood agar to confirm the growth of E. faecalis.
SEM evaluation
Additional teeth were prepared, one for each group, and were irrigated with the same solutions as described before, but the canals were not filled with gutta-percha. These teeth were separated longitudinally with diamond burs for examination with an SEM (LEO 440 Scanning Electron Microscope, UK), and photographed.
Statistical analysis
After daily decoding, the data were statistically evaluated with SPSS for Windows version 15.0 software using a χ2test. Statistical significance was set at p<0.05.
Results
At least 19 teeth were needed to give a 5% error level (α) and 80% power.
All teeth in the positive control group showed broth turbidity. Throughout the test period, the broth remained clear for all teeth in the negative control group.
In all specimens, when turbidity occurred, bacteriological tests confirmed that the microorganism in the lower chamber of the samples was E. faecalis.
No statistically significant differences were noted among the five groups (p>0.05). Of the KTP laser specimens, 5% did not show apical microleakage (Table 1). Leakage rate between the groups and leaking days were not statistically significant, either.
CHX, chlorhexidine gluconate; NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid; KTP, potassium-titanyl-phosphate.
Discussion
The main goal of the experimental model was to completely isolate the coronal chamber from the apical chamber, thereby reducing the chance for cross contamination. Many studies have demonstrated that bacteria leak through the root fillings when root canals are exposed to the oral environment. 14,28,29 Bacterial microleakage testing methods have been reported to have advantages over other clinical tests. 30 In addition, bacterial byproducts cause periapical infections by stimulating the growth of bacterial cell wall products; therefore, bacterial microleakage tests are necessary in clinical situations because these tests are adaptable and give accurate information. 31
All teeth in the positive control group showed turbidity, which demonstrated that bacteria penetrated the total root canal length. Likewise, the negative control group had no turbidity of broth throughout the experimental period, which showed that there was no leakage in the complete system.
Persistent endodontic infections are frequently caused by E. faecalis. 32 This microorganism can survive long periods without nutrients 33 and is rarely found in primary infections, but is most often isolated in repeat treatment cases of apical periodontitis. 34 This microorganism was the most resistant to inter-appointment medicaments, including calcium hydroxide. 35 E. faecalis invades deep into the dentinal tubules, and can contain an aggregation of substances, including surface adhesins, sex factors, lipoteichoic acid, extracellular superoxide production, and hyaluronidase, as well as virulence factors such as cytolysin. These materials can protect the bacterium from the effects of calcium hydroxide and other endodontic materials. 36 E. faecalis colonizes human tooth root canals and forms a biofilm that exhibits resistance to the medicaments and irrigation solutions used for root canal treatment. Further development of treatment options is required in this direction. 37 Our preference was to study E. faecalis, because it is resistant to root canal treatment, it is easily produced in laboratory conditions, and it cultures well.
In the present study, all teeth showed bacterial penetration within the 30-day period except for one sample treated with KTP laser. The 30-day observation time was chosen based on a coronal microleakage study by Jacobovitz et al. and Shipper et al. 38,39
The smear layer is formed by the combination of parts of organic and inorganic components of dental structures that occurs during cutting, grinding, and filing operations on the surface of teeth. 8 Even though the smear layer is formed as a physical barrier against bacteria and their products, with plugs that prevent the penetration of bacteria and stop the invasion into the dentinal canals, bacteria could remain and proliferate in dentinal tubules after instrumentation. Our findings are consistent with previous research that showed no significant developments after removal of the smear layer. 40 –42 On the other hand, other studies have shown less bacterial leakage after removal of the smear layer. 43,44 These contradicting results might be because of the use of different sealers, root canal irrigants, and laboratory conditions.
Propolis is a multifunctional material that has many antibiotic, antifungal, antiviral, and non-allergenic properties. 45 Propolis in a solution form has never been tested for its capacity for removal of the smear layer. Özan et al. found that alcoholic extracts of propolis showed cytotoxicity against control cell lines, which is why we used the dimethyl sulfoxide as a solvent for propolis. 46 In the present study, all experimental groups showed bacterial microleakage with propolis, although some of the propolis remained in some areas, even after washing with distilled water (Fig. 2). Almost all of the dentinal tubules were closed with a smear layer. The large-particle structure of propolis in the root canals could have caused microleakage.
Residues of propolis on dentinal tubules.
Straight single-rooted teeth were used in our study, and the endodontic laser fiber may not have reached to the apical third in curved root canals because of its 200 μm diameter. Laser devices need to be further developed, because zipping and ledging are often reported when treating curved root canals. 47 A more homogeneous action of the laser beam on the surface of dentin might be obtained if both the end portion and the lateral parts of the fiberoptic cable are applied. For this reason, we applied the fiber tip in a circular motion, apically to the corona.
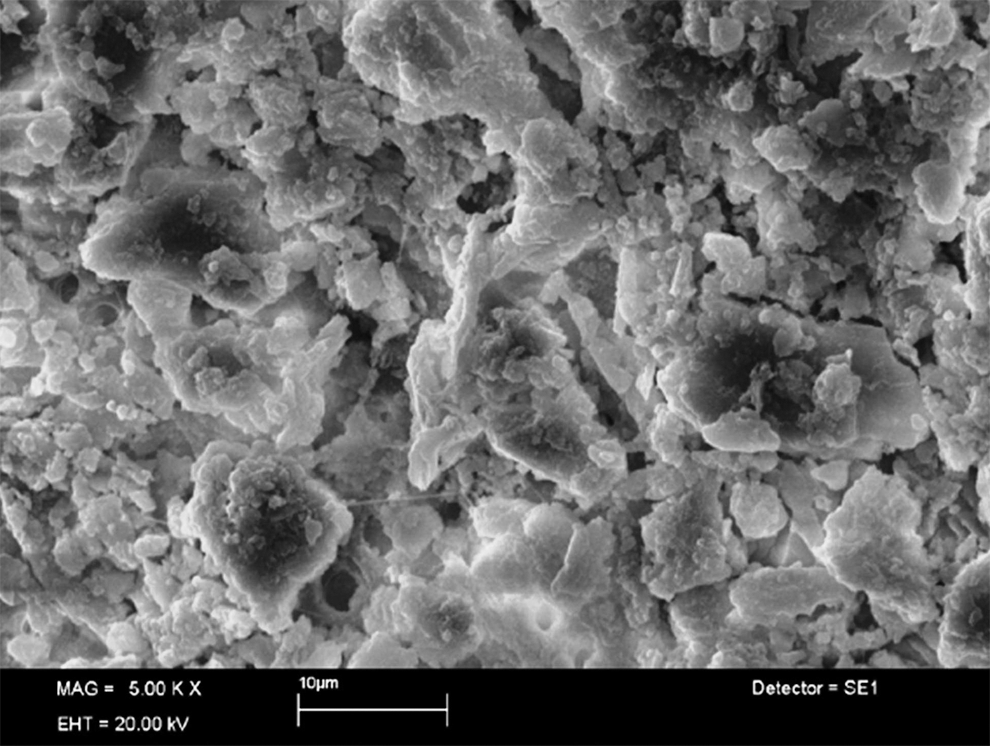
The root canals were irradiated with the KTP laser after irrigation with distilled water. The laser was applied within the safety limits and used 30 sec cooling intervals, as reported by Nammour et al. 48 The removal of the smear layer and debris from root canals by 532 nm wavelength KTP laser irradiation has been reported previously. 25 The SEM images in the present study demonstrated that the KTP laser almost completely removed the smear layer on all areas of the dentin surfaces. The orifices of the dentinal tubules were closed or narrowed because of the recrystallization that followed melting and solidification (Fig. 3). In contrast to the present study, Shoji et al. asserted that the melt areas of the dentin walls might provide for isolation of the bacteria, thereby preventing the proliferation of bacteria in the main canals. 49 However, in our study, only 5% of specimens did not show apical microleakage, and this value was not statistically significant.

The melted dentin blocked the dentinal tubules.
The significance of the irrigation solution in endodontic treatment is well acknowledged. 13 In this study, we aimed to compare the commonly used irrigation solutions and rarely used KTP laser system or propolis. NaOCl has been widely used in endodontic treatment to deliver all of the required debridement, disinfection, lubrication, and decomposition of tissues because of its capability to dissolve organic substance, together with its extensive antibacterial properties. For this reason, it is often suggested as the main endodontic irrigant. 5 Hayashi et al. 50 reported that EDTA generates morphological modifications in radicular dentin, such as demineralization. EDTA also chelates calcium ions, which are part of the dentine molecular complex. 44 No irrigation solution has yet been developed that is capable of concurrent demineralization of the smear layer and softening of organic matter. 51 Therefore, EDTA is recommended as a treatment for eradicating and preventing the formation of the smear layer related to root canal instrumentation. 13 CHX, a cationic bisguanide, has ideal antibacterial activity over the pH range from 5.5 to 7.0. 52 It is frequently used at concentrations between 0.2% and 2%, 13 and the most common preparation is CHX. 53 It is sometimes used as the main irrigant or as an alternative because of its variable antimicrobial activity. 13,54,55
Our literature search did not reveal any previous studies that compared the efficacy of KTP laser and propolis on smear layer prevention or removal. To the best of our knowledge, this is the first study of bacterial microleakage that compares propolis and KTP laser treatments; therefore, further investigation of this issue is needed.
Conclusions
All specimens exhibited bacterial leakage, except 5% of the KTP laser group.
The extent of microleakage of in the irrigation solution allowed us to draw the following conclusions: 1. The leakage among the five experimental groups showed no statistically significant differences. 2. Apical leakage did not affect root canals irradiated with KTP laser and filled with gutta-percha, compared with the other irrigation solutions. 3. KTP laser irradiation can be used to remove the smear layer, but removal of the smear layer does not reduce the penetration of bacteria through the root canal filling. 4. Root canals that were irradiated by KTP laser looked smooth and regular in SEM images. However, at the end of the experiment, all groups exhibited microleakage and no statistically significant difference was noted among the groups. 5. To prevent microleakage, coronal restoration should be done immediately after a root canal treatment.
Finally, the extent of bacterial microleakage will not change even if the smear layer is removed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.