
Abstract
Introduction
Photodynamic therapy (PDT) involves dynamic interaction between light, a photosensitizer (PS) and oxygen (present in and around cells). 4 –18 A PS is a chemical compound (usually a dye) that can be excited by the light of a specific wavelength. In the treatment of oral diseases such as chronic periodontitis, the PS is commonly injected into the target area (e.g., deep periodontal pocket in patients with chronic periodontitis); however, PSs may also be injected systemically and/or administered orally. 19 The PS accumulates in the targeted tissues and is exposed to light of a specific wavelength (most photosensitizers are activated by light wavelengths ranging between 630 and 700 nm). This reaction induces the production of reactive oxygen species (ROS) that causes oxidative damage to the target cells (such as tumor and bacterial cells). 20 In addition, incorporation of membrane disorganizing agents (such as ethylenediaminetetraacetic acid) in photosensitizers has been reported to enhance their migration into the cytoplasm of gram-negative bacteria. 21 These agents cause the displacement of magnesium and calcium ions that neutralize the superficial negative charges; this endorses an electrostatic repulsion, thereby destabilizing the bacterial cell wall structure. Damages to the cytoplasmatic membrane can involve leakage of cellular contents or inactivation of membrane transport systems and enzymes. 22 Therefore, the use of visible light with photosensitizers is a useful adjuvant to mechanical methods, as well as antibiotics, in reducing the numbers of oral bacteria. PSs commonly used in the treatment of periodontal disease, periimplantitis, and endodontic infections include methylene blue (MB) and toluidine blue (TBO). 7,8,23 –26
Studies 4 –7 have investigated the efficacy of PDT in killing oral bacteria. Fontana et al. 11 investigated the response of normal rat tongue mucosa to PDT following topical application of various PSs including hematoporphyrin derivative, MB and poly lactic-co-glycolic acid nanoparticles loaded with MB. The results demonstrated that these nanoparticles safely target oral pathogenic bacteria without jeopardizing the normal oral tissues. 11
As PDT exhibits antibacterial effects that make it a modern and effective means of treating inflammatory diseases, the purpose of the present article was to assess whether or not PDT enhanced standard antibacterial therapy in dentistry.
Review Procedure
Search strategy
To address the question “Does PDT enhance standard antibacterial therapy in dentistry?” MEDLINE®/PubMed databases were searched. The searches were repeated in the Google Scholar database to determine a variety of characteristics including format, date, medical subject headings where appropriate, uniqueness, duplications, and full-text availability from the author's institution. The databases were searched from 1987 up to and including July 2013, using the following terms in various combinations:
Inclusion and exclusion criteria
Original studies (clinical and experimental) published in the English language were included. Letters to the Editor, historic reviews, and unpublished data were excluded.
The pattern of the present comprehensive review study was customized to primarily summarize the pertinent information (Fig. 1).
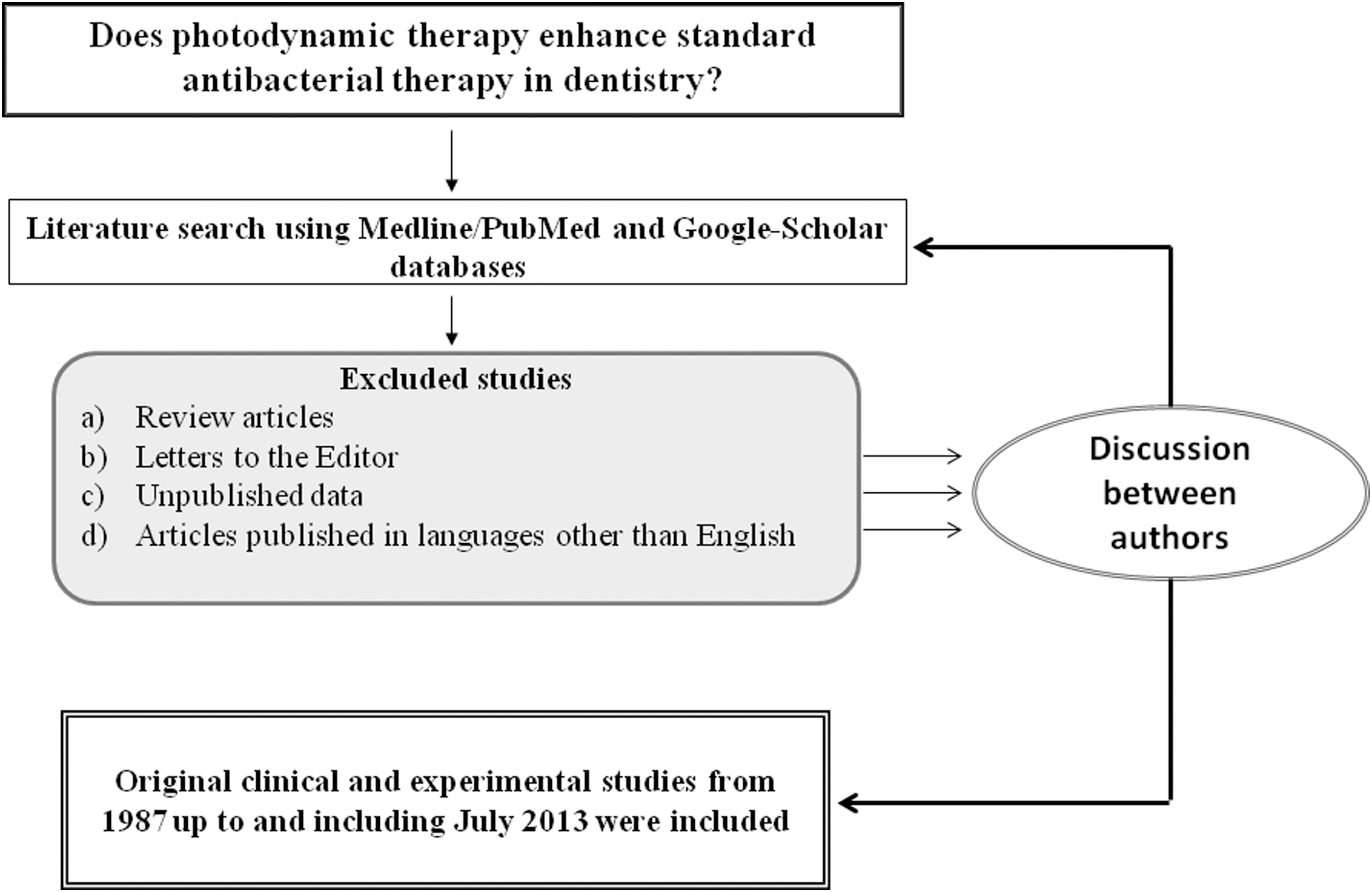
Literature search protocol.
Review of the Literature
Effect of PDT on periodontopathogenic bacteria
It is known that accumulation of bacteria in the oral biofilm and poor oral hygiene maintenance are significant risk factors of gingivitis and periodontitis. 27 –29 Conventionally, scaling and root planing (SRP) with adjunct plaque control regimes are used to manage periodontal inflammatory conditions. 30 Studies 4,31,32 have shown that periodontal bacteria are susceptible to PDT in planktonic cultures. Other experimental studies 33,34 have also demonstrated that light from a helium-neon (He-Ne) laser or a gallium-aluminum-arsenide laser, in combination with a PS, significantly reduces the viability of aerobic and anaerobic bacteria in subgingival plaque. In addition, bacteria causing periodontal disease can be killed through photosensitization with TBO and irradiation with a He-Ne soft laser. 33,34 Romanos and Brink 8 compared the antimicrobial effects of PDT with those of other laser wavelengths (980 nm diode and 1064 nm Nd:YAG) during periodontal therapy in 10 patients with chronic periodontitis. In this study, 8 sites with chronic periodontitis were divided into four groups on the basis of the adopted therapeutic strategy: In Group 1, 62 sites received SRP and irradiation from an Nd:YAG laser (with a wavelength of 1064 nm); in Group 2, 63 sites received SRP and irradiation from a diode laser (with a wavelength of 980 nm); and in Group 3, 63 sites received SRP and PDT using a wavelength of 670 nm. In Group 4 (control group), 64 sites underwent only SRP. During an observation period of 3 months, the examined periodontal sites showed significant bacterial reduction when PDT was used as an adjunct to SRP. 8 It is worth mentioning that in the study by Romanos and Brink, 8 PDT as an adjunct to mechanical debridement resulted in significant reduction in periodontal bacteria (Fusobacterium nucleatum) as compared with periodontally inflamed sites treated with high-level lasers as an adjunct to mechanical debridement. In an experimental study, Chan and Lai 35 showed that exposure to the 100 mW laser light eliminated ∼40% of periodontal bacteria; whereas nearly 95% of the periodontal pathogens were killed when exposed to 665 nm wavelength diode laser in the presence of MB. This study 35 concluded that mechanical debridement with adjunctive PDT (using a 665 nm wavelength diode laser for 60 sec in the presence of MB) significantly reduced the periodontopathogen count as compared with when mechanical debridement was used alone to control periodontal disease.
In a randomized clinical study, Braun et al. 36 investigated the effects of a single session of MB-mediated PDT and/or SRP on relative attachment level, probing depth (PD), gingival recession, and sulcus fluid flow rate in 20 patients with chronic periodontitis. Periodontal pockets were irrigated with MB (10 mg/mL) for 3 min, followed by exposure to light at 660 nm from a 100 mW diode laser for 1 min per tooth. The results demonstrated that sites treated with SRP with adjunct PDT showed significant reduction in clinical markers of periodontal disease, including PD and gingival bleeding, as compared with sites treated with SRP alone. 36
Effect of PDT on cariogenic bacteria
Dental caries is a disease of the mineralized tissues of teeth (namely, enamel, dentin, and cementum) caused by the action of cariogenic bacteria (including Streptococcus mutans, Streptococcus sobrinus, and Lactobacilli) on fermentable carbohydrates. If left uncontrolled, dental caries may cause demineralization of the mineral portions of teeth and disintegrate the organic matrix. Experimental studies 37 –39 have shown that PDT kills cariogenic bacteria in the planktonic and biofilm phases. PDT has also been reported to effectively reduce the number of bacteria in supragingival plaque samples obtained from human subjects. 40 In an experimental study, Mang et al. 4 tested the ability of PDT to treat localized infections of S. mutans in biofilm communities. In this study, 4 porfimer sodium was used as a PS and laser irradiation was performed at 630 nm and 100 mW/cm2. The results demonstrated that PDT using porfimer sodium and 630 nm laser light was effective in significantly reducing the viability of S. mutans biofilms. 4 Likewise, in an experimental study, Ishiyama et al. 5 assessed the efficacy of various PSs (rose bengal, erythrosine, and phloxine) incorporated in plaque-disclosing agents in killing cariogenic bacteria using PDT. Wavelengths of laser light used for excitation of the three PSs were spectrophotometrically determined, and it was established that wavelengths of 530–550 nm are suitable to excite all of the aforementioned PSs. The results showed that PDT using rose bengal showed the highest bactericidal activity against S. mutans (followed by erythrosine and phloxine) when irradiated by the laser light with a wavelength of 532 nm for 60 sec. 5 With reference to the Ishiyama study, 5 had the bactericidal effect of laser-irradiated PSs been entirely dependent upon the amount of photogenerated singlet oxygen, phloxine would have shown the highest bactericidal activity; however, rose bengal (but not phloxine) showed the highest bactericidal activity compared with other PSs. This suggests that other factors are involved in the overall bactericidal activity. In this study, 5 rose bengal incorporated efficiently into the bacterial cells as compared with the other PSs used. This seems to be a possible factor that gave rose bengal the highest bactericidal efficacy as compared with erythrosine and phloxine. In another in vitro study, Metcalf et al. 40 reported that erythrosine-mediated PDT (using white light irradiation for 5 continuous min) enhanced the killing of S. mutans in oral biofilm samples. Likewise, Vahabi et al. 41 evaluated in vitro the antimicrobial effects of TBO and Radachlorin®, in combination with a diode laser, on the viability of S. mutans. Bacterial suspensions of S. mutans were exposed to 0.1% TBO associated with a 633 nm diode laser (20 mW, continuous mode, 150 sec). The results showed that potential S. mutans cell killing was observed following photosensitization with TBO. 41 Guglielmi et al. 42 also reported that PDT using a 660 nm diode laser, and MB, played an essential role in killing cariogenic bacteria, including the S. mutans and Lactobacilli species. It is, therefore, evident that PDT is an effective means of eliminating cariogenic bacteria (in particular S. mutans) even when the bacteria are embedded in an extracellular matrix; however, further research is warranted to assess the bactericidal efficacy of PDT with reference to their ability to incorporate into the bacterial cells walls.
Effect of PDT on the treatment of infected root canals
Endodontic infections are caused by the proliferation of bacteria that penetrate the pulp chamber and the root canal system. Antimicrobial PDT has been reported to be an effective adjunct to conventional endodontic disinfection treatment because of its ability to eliminate bacteria that remain in root canals, even after irrigation with sodium hypochlorite (NaOCl).
43
In an in vitro study, Ng et al.
44
investigated the antimicrobial effects of PDT on infected human teeth. In this study,
44
52 freshly extracted teeth with pulp necrosis and associated periradicular radiolucencies were obtained from 34 subjects. Twenty-six teeth with 49 canals received chemomechanical debridement (CMD) with 6% NaOCl, and 26 teeth with 52 canals received CMD and PDT, using 50 μg/mL MB followed by exposure to a 665 nm laser light. The contents of root canals were sampled by flushing the canals at baseline and after CMD alone or after CMD and PDT, and were cultured on blood agar. The results demonstrated that PDT with CMD significantly reduced residual bacteria within the root canal system as compared with when CMD was used alone.
44
Endodontic infections with Enterococcus fecalis have also been associated with endodontic failures. In an in vitro study by Pagonis et al.
24
E. faecalis species were sensitized in the planktonic phase and in experimentally infected root canals of human extracted teeth with MB-loaded nanoparticles for 10 min, followed by exposure to light at 665 nm. The results demonstrated that the nanoparticles were concentrated on the bacterial cell walls and that PDT significantly reduced the E. fecalis counts.
24
Xu et al.
45
tested the hypothesis that PDT doses that can be used for eliminating root canal microorganisms in vivo do not induce cytotoxic effects on normal human gingival fibroblasts in culture. In this study,
45
cells were incubated in 50 μg/mL MB and exposed to 665 nm light for 10 min. The laser power density and energy fluence were set at 40 mW/cm2 and 12 J/cm2. The results demonstrated that synergism of 50 μg/mL MB and red light did not have any significant cytotoxic effects on the viability and mitochondrial activity of human gingival fibroblasts. However, cells in the control group (treated with NaOCl alone) inhibited mitochondrial activity and reduced cell viability up to 100%. Results by Xu et al.
45
reflect that PDT is significantly less cytotoxic to mammalian cells than NaOCl, which is commonly used in clinical endodontic practice. An explanation in this regard may be that the polycationic conjugate between poly
Ex vivo studies 17,43,46,47 have shown that PDT significantly eliminated gram-positive bacteria; however, in an in vivo study, Garcez et al. 14 reported that PDT was an efficient treatment toward eliminating gram-negative and multidrug resistant microorganisms such as Enterococcus sp, Prevotella sp, Actinomyces sp, Peptostreptococcus sp, Streptococcus sp, Fusobacterium sp, Porphyromonas sp, Enterobacter sp, and Propionibacterium sp. A possible explanation in this regard may be derived from the fact that the PS (PEI-ce6) used in the in vivo study, 14 had a high efficacy in killing gram-negative bacteria compared with other PSs such as TBO. 48 Lauro et al. 49 attempted to induce resistance in bacteria against PDT in the generation of any PDT-resistant bacterial sp, but all attempts failed. This suggests that bacteria find it demanding to develop defenses against ROS generated during PDT. Most of the studies by Garcez et al. 14,15,17 showed that PDT, when used as an adjunct to CMD, is more efficient in eliminating bacteria from infected root canals than when CMD is used alone. However, it has also been reported that choice of root canal irrigant selected for conventional root debridement (prior to PDT) also influences the overall bactericidal efficacy of the treatment. 18,50 Spectroscopy results 18 have suggested that the amount of MB is higher inside the microbial cells when hydrogen peroxide (H2O2) is used either before or simultaneously with PDT, which leads to ROS formation inside microbial cells thereby confirming that ROS production is higher in the presence of H2O2. It is possible that the reaction between photoexcited MB and H2O2 results in a higher production of either hydroxyl or, more likely, hydroperoxide radicals, and that these ROS could attack the microorganisms more strongly than when PDT is performed without using H2O2. Further studies are warranted to verify this hypothesis.
Effect of PDT in endodontic treatment of deciduous teeth
To our knowledge from indexed literature, the effect of PDT on endodontic treatment of primary teeth has not been intensely investigated. Pinheiro et al. 51 quantified viable bacteria in deciduous teeth with necrotic pulp before and after instrumentation and after the use PDT. In this study, 51 10 radicular canal cultures were made. The first culture was made immediately after access and location of the radicular canal, whereas the second and third cultures were made after the conclusion of chemical-mechanical instrumentation and PDT, respectively. PDT was performed using TBO (0.005% mg/L) and a 660 nm low-intensity diode laser (4 J/cm2 energy, 100 mW) application for 40 sec. The results demonstrated that instrumentation resulted in an 82.59% reduction of viable bacteria, whereas after PDT, 98.37% of bacterial reduction was observed and the difference between both treatments was statistically significant. 51 This study 51 concluded that mechanical/chemical instrumentation with adjunct PDT is effective for bacteria reduction in deciduous teeth with necrotic pulps as compared with when instrumentation is performed alone. It is tempting to speculate that chemical-mechanical instrumentation followed by PDT plays an essential role in microbial reduction, as the canal instrumentation helps remove the smear layer and radicular dentin debris, leading to dentin tubules opening, which in turn increases the dye permeability in the radicular dentin. This seems to augments the overall bactericidal efficacy of the entire treatment. As the role of PDT in pediatric dentistry has not been extensively researched, further studies are warranted to assess the effects of PDT for bacterial reduction in carious deciduous teeth.
Effect of PDT on the treatment of peri-implantitis (PI)
PI is an inflammatory condition that jeopardizes the alveolar bone and soft tissues around implants and (if left untreated) may result in implant failure. 52 The incidence of PI has been reported to be five times greater in patients with chronic periodontitis than in patients who are free of periodontitis. 53 Dental plaque is considered to be the most important factor in the pathogenesis of PI, and greater proportions of periodontal pathogens have been found in infected and failing implants than in successful implants. 54 A limited number of studies 55,56 have reported the effects of antimicrobial PDT as an adjunct to the treatment of PI. Results from experimental studies 56,57 have reported that PDT eliminates Fusobacterium and Prevotella species and β hemolytic Streptococci in dogs with ligature-induced PI. Likewise, a clinical study 55 showed that PDT partially (yet significantly), reduced the colonization of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, and Prevotella intermedia around implant surfaces. In a randomized control trial, Schär et al. 7 showed that nonsurgical mechanical debridement of PI sites with adjunctive use of PDT was more effective in eliminating periimplant inflammation than when mechanical debridement was used alone. However, an in vitro study 6 showed the complete elimination of P. gingivalis from titanium plates following application of PDT. In a recent 1 year follow-up randomized control trial, Bassetti et al. 59 compared the effects of local drug delivery (LDD) using minocycline microspheres or adjunctive PDT in the treatment of PI. One year follow-up results showed no statistically significant differences between groups with respect to the red complex bacteria (P. gingivalis, Treponema denticola, and Tannerella forsythia). These results reflect that optimum plaque control plays a pivotal role in the treatment of PI. 59 Further studies are warranted to assess the role of PDT in the treatment of PI.
Limitations
It is well known that periodontal disease is worse in patients with systemic conditions (poorly-controlled diabetes mellitus [DM] and prediabetes) than in systemically healthy individuals. 27,28,60 It is tempting to speculate that conventional periodontal therapy with adjunct PDT significantly reduces supra- and subgingival bacterial counts in immunocompromised individuals. Al-Zahrani et al. 61 conducted a short-term clinical study to assess the effect of the adjunctive use of PDT on periodontal status and glycemic control of patients with type 2 DM and moderate to severe chronic periodontitis. PDT was performed using a formulation consisting of 0.01% MB and irradiation with a 670-nm non-thermal diode laser. The results demonstrated no significant differences in periodontal parameters among the three study groups: SRP only, SRP+systemic doxycycline, and SRP+PDT. 61 Al-Zahrani et al. 61 concluded that PDT does not benefit conventional nonsurgical periodontal therapy in patients with diabetes. This may possibly be attributed to the massive inflammatory response induced by hyperglycemia that may have nullified the benefits of SRP with adjunct PDT on periodontal wound healing. It is, however, notable that the results reported by Al-Zahrani et al. 61 were short-term outcomes. Whether or not PDT in patients with well-controlled DM can reduce oral bacteria to the same extent as in medically healthy individuals with periodontitis warrants further in vivo investigations. Another factor that may limit the benefits of PDT in terms of reducing bacterial load is habitual use of tobacco products. It has been reported that habitual tobacco smoking has detrimental effects on periodontal healing following treatment. 62 Al-Zahrani and Austah 63 conducted a split-mouth, single-masked randomized controlled clinical trial to assess the efficacy of PDT when used as an adjunctive treatment to SRP for treating chronic periodontitis in smokers. In this study, 63 54 teeth with PD>5 mm at one or more periodontal sites in 20 smokers diagnosed with chronic periodontitis were selected. In each patient, at least one tooth was randomly assigned to SRP+PDT (test group) and the contralateral tooth was assigned to SRP only (control group). In each group, plaque index (PI), bleeding on probing (BOP), PD, gingival recession, and clinical attachment loss (CAL) were recorded at baseline and at 12 weeks follow-up. The results demonstrated that PDT, when used as an adjunct to SRP, significantly reduces PI, PD, and CAL. 63 However, in this study, 63 the efficacy of PDT with adjunct SRP to kill periodontopathogenic bacteria remained undetermined. Further studies are warranted to assess the antibacterial efficacy of PDT in tobacco consumers.
Conclusions
Within the limits of the present literature review, it is concluded that PDT, when used as an adjunct to conventional oral disinfection protocols, enhances standard antibacterial therapy in dentistry.
Footnotes
Acknowledgments
The authors thank the College of Dentistry Research Center and Deanship of Scientific Research at King Saud University, Saudi Arabia for funding this research project (Project # FR 0060).
Author Disclosure Statement
No competing financial interests exist.