
Abstract
Introduction
PDT has been studied as a promising approach to eradicate oral pathogenic bacteria 6,7 that cause diseases such as periodontitis, 12 peri-implantitis, 13 and dental cavities. 14 The oral cavity has complex microflora, because of the different environments associated with different anatomical sites in both hard and soft tissues. An example is the presence of anaerobic microorganisms in the subgingival area caused by low oxygen supply. More than 1000 different species have been identified in the mouth, and most of them can be found attached to surfaces forming biofilms. 15,16
Dental prosthetic materials have developed greatly since the 1970s, and they aim to mimic dental hard tissues in order to repair the physiological and esthetic oral functions. All of these biomaterials as well as the natural tissues in the mouth, such as dental enamel and cementum are open environments for bacterial adherence and biofilm formation. In addition to the oral infections caused by biofilm bacteria, these pathogens also represent a threat for systemic infections as found in infective endocarditis (IE), which represents a major cost burden for healthcare services. 17 The American Heart Association (AHA) has identified risk factors for IE including the use of prosthetic cardiac valves or prosthetic materials used to repair cardiac valves, congenital heart disease, and cardiac transplantation, and the AHA has recommended antibiotic prophylaxis for all dental procedures that involve possible bleeding, as manipulation of gingival tissue or the periapical region of teeth and any type of perforation in the oral mucosa. Furthermore, in 1997, the AHA recognized that most cases of IE were not related to invasive procedures but were the result of frequent and transient bacteremia caused by routine daily activities, such as brushing and flossing teeth. 18
In view of the growing problem of bacterial resistance to conventional antimicrobials, the use of an alternative bactericidal approach to which bacteria are not likely to develop resistance would be valuable. The current treatment for dental plaque-related diseases in the oral cavity involves, first, the mechanical removal of all accessible contamination, and, second, the use of topical and/or systemic antimicrobial medications. 19 PDT may be a suitable antimicrobial approach that can overcome biofilm and antimicrobial-related resistance.
The aim of this study was to test PDT as an antimicrobial approach to disrupt biofilm formed on a dental hard tissue. We evaluated the effect of the phenothiazinium PS, methylene blue (MB), and a 660 nm diode laser on bacterial viability, and biofilm architecture as well as microorganism morphology. We used a mixed biofilm composed Enterococcus faecalis, a Gram-positive bacteria, and Pseudomonas aeruginosa, a Gram-negative bacteria, which are well known to have different sensitivities to PDT.
Materials and Methods
Biofilm growth and bacterial strain
P. aeruginosa (XEN5) that had been engineered to be stably bioluminescent by transformation with a transposon containing the entire Photorhabdus luminescens lux operon 20 was kindly donated by XenogenCorp. (Alameda, CA) and was used for real-time monitoring of bacterial reduction inside the root canal. E. faecalis (ATCC® 1494), both in a single species biofilm, and in a mixed biofilm with P. aeruginosa (XEN5) were used for scanning electron microscopy (SEM) analysis to evaluate the effects of PDT on biofilm architecture and cellular morphology.
The bacteria were grown in brain heart infusion (BHI) broth at 37°C with shaking (150 rpm) to form a stationary growth phase suspension of 1×10(9) cells/mL. Ten microliters of the microorganism suspension was poured inside the root canals of 10 human single-rooted anterior teeth, which had been previously endodontically prepared with rotatory instrumentation up to file # 30.4 (working length of ∼15 mm) and sterilized by autoclaving for 15 min at 121°C. After inoculation, each tooth was placed inside a 1.5 mL microcentrifuge tube that was subsequently sealed and kept upright and incubated, with the bacterial suspension, for 72 h at 37°C, with shaking to allow biofilm formation. To facilitate the biofilm formation, the BHI broth was changed every 24 h.
Growing a biofilm in root canal
After 72 h, bioluminescence imaging of each tooth (in the P. aeruginosa group) inside its transparent microcentrifuge tube was performed with a low-light intensified camera (Hamamatsu Photonics KK, Bridgewater, NJ). The use of this imaging system has been described in detail in previous work. 21 Briefly, bioluminescence signal was accumulated for 2 min at 35 sensitivity level and a maximum setting on the image intensifier control module. Using ARGUS software (Siemens Medical Solutions, Erlangen, Germany) the luminescence image was presented as a false-color image superimposed on top of the gray scale reference image. The image-processing component of the software gave mean pixel values from the luminescence images on defined areas covering each tooth on a 256 gray scale. For bioluminescence comparison, all images were recorded at same bit range. These images served to confirm the level of infection and to obtain the initial signal from the bacteria inside the root canals.
Antimicrobial photodynamic therapy
To estimate the effect of PDT on planktonic bacteria, suspensions of P. aeruginosa in stationary phase were diluted in phosphate-buffered saline (PBS) to a cell density of 109/mL, and 1 mL aliquots were added to wells of a 24 well plate and the relative light unit values were read in a luminescence plate reader (MicroBeta Trilux 1450, PerkinElmer Life And Analytical Sciences, Inc., Wellesley, MA). Bacteria were incubated with 1 mL of MB (Sigma-Aldrich, Milwaukee, MI) (60 μM dissolved in distilled water) for 10 min followed by illumination with 660 nm light from a diode laser (MMOptics, São Paulo, Brazil) for defined times corresponding to the delivery of 2.4, 4.8, 7.2, and 9.6 J of total energy.
At each stage, the luminescence values were measured. To evaluate the effect of PDT on biofilms grown on root canal dentine tissue, all liquid content inside the root canal was removed with a pipette, and the canals were filled with 10 μL of MB 60 μM and allowed to incubate for 2 min followed by a second bioluminescence imaging to quantify any dark toxicity of the PS. Thereafter, the illumination was performed with a 300 mm diameter fiber-coupled diode laser (MMOptics, São Paulo, Brazil). The diode laser delivered 660 nm light at a total power of 40 mW out of the fiber. The fiber was initially placed in the apical portion (bottom) of the root canal, and spiral movements, from apical to cervical, were manually performed to ensure the even diffusion of the light inside the canal lumen. These movements were repeated ∼10 times/min, and after each minute, a bioluminescence image was captured. The irradiation was performed for 4 min, total energy out of the fiber of 9.6 J (2.4 J/min) and bioluminescence imaging was performed after each minute until the end of the treatment. 1,3,5
SEM images
E. faecalis (ATCC 29212) and a mixed biofilm composed of E. faecalis and P. aeruginosas, simulating a situation in which Gram-positive and Gram-negative bacteria (known to be more resistant to PDT) were coexistent in a multi-species biofilm model. The growing conditions were the same as described previoiusly, with a 72 h culture time on the surface of bisected teeth (see subsequent description) and on a glass slide.
To grow the biofilm on dental tissue, an anterior single canal tooth was previously sectioned longitudinally in two halves (∼15 mm in length) and cleaned with 37% H3PO4 (FGM, Blumenau, SC Brazil) for 1 min plus 2.5% NaOCl (Biodinamica, Londrina, PR Brazil) for 5 min and sterilized by autoclaving (121°C for 15 min). The samples were then randomly divided into two groups. Group one received MB solution for 2 min and group two also received MB solution for 2 min plus 9.6 J (4 min), 660 nm light, from the same diode laser equipment, using the same parameters described. After that, the samples were washed with saline solution to remove the cells nonadherent to the biofilm, and then fixed for SEM. The species were incubated with increasing concentrations of ethanol for 30 min, dried at 37°C for 24 h, and placed on a mounting base. Finally, the samples were coated with gold and examined under a SEM.
The SEM images were analyzed using the software ImageJ (National Institute of Health, Bethesda, MD) to measure the cell diameter and biofilm area (in pixels) after MB incubation and after PDT. To calculate the cell diameter, 20 randomly selected cells were measured in each image. 22 The biofilm was measured selecting the total area of each image covered by the biomass on the initial image and after the PDT treatment; to confirm these data, the area uncovered by the biofilm was also compared on the initial and final images.
The measures from cell diameter and biofilm areas were tested for significant differences by using analysis of variance (ANOVA) followed by Tukey tests. p<0.05 was considered statistically significant. Statistical comparisons between means were performed with software Origin, version 8.5 (OriginLab, Northampton, MA).
Results
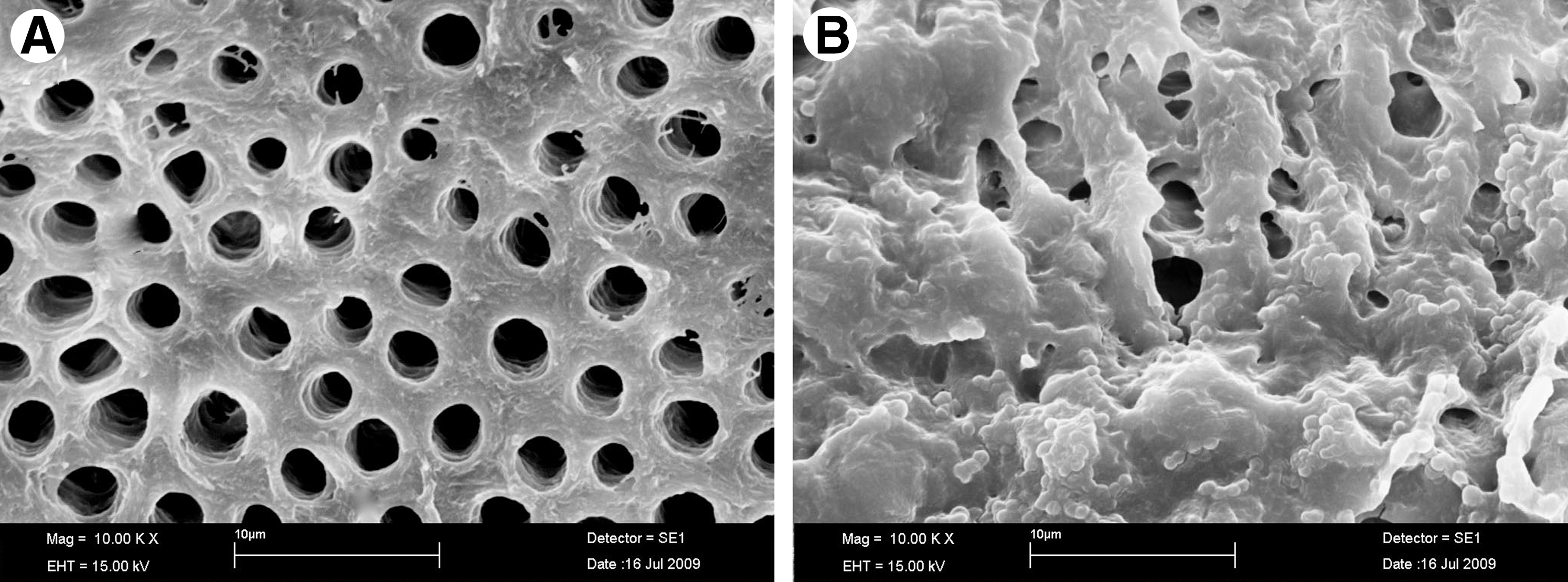
The addition of 10 μL of a suspension containing 109 cells of P. aeruginosa into the root canals followed by 3-day incubation at 37°C reliably and reproducibly produced a bioluminescent biofilm that could be imaged through the entire width of the tooth. There were minor variations from tooth to tooth in the pattern of the detected luminescence, which was probably the result of differences in the geometry of the root canal system. The presence of a microbial biofilm rather than planktonic bacteria was demonstrated by the failure of irrigation with saline to significantly diminish the luminescence signal (data not shown). Also, the images (Fig. 1) comparing a clean dentine surface and a 3-day incubated surface with E. faecalis clearly demonstrated the biofilm formation.
Our results showed only a slight reduction in bioluminescence signal from the bacteria in the root canal biofilm after 2 min of incubation with MB solution in the absence of light, because of its low inherent toxicity (0.1 log). By contrast, after illumination, the reduction of the signal was dramatic. Representative bioluminescent images from before and after irradiation, for all energies tested over the biofilm incubated with MB, are presented in Fig. 2 (panel A–F). When the effects of PDT on planktonic bacteria and on biofilms were compared (Fig. 3), the results showed that the energy necessary to achieve reduction of bioluminescence signal in planktonic bacteria was lower than that required to achieve the same results on biofilm (p=0.03).

Representative bioluminescence images captured of teeth infected with 3 day Pseudomonas. aeruginosa biofilms. The teeth received either:
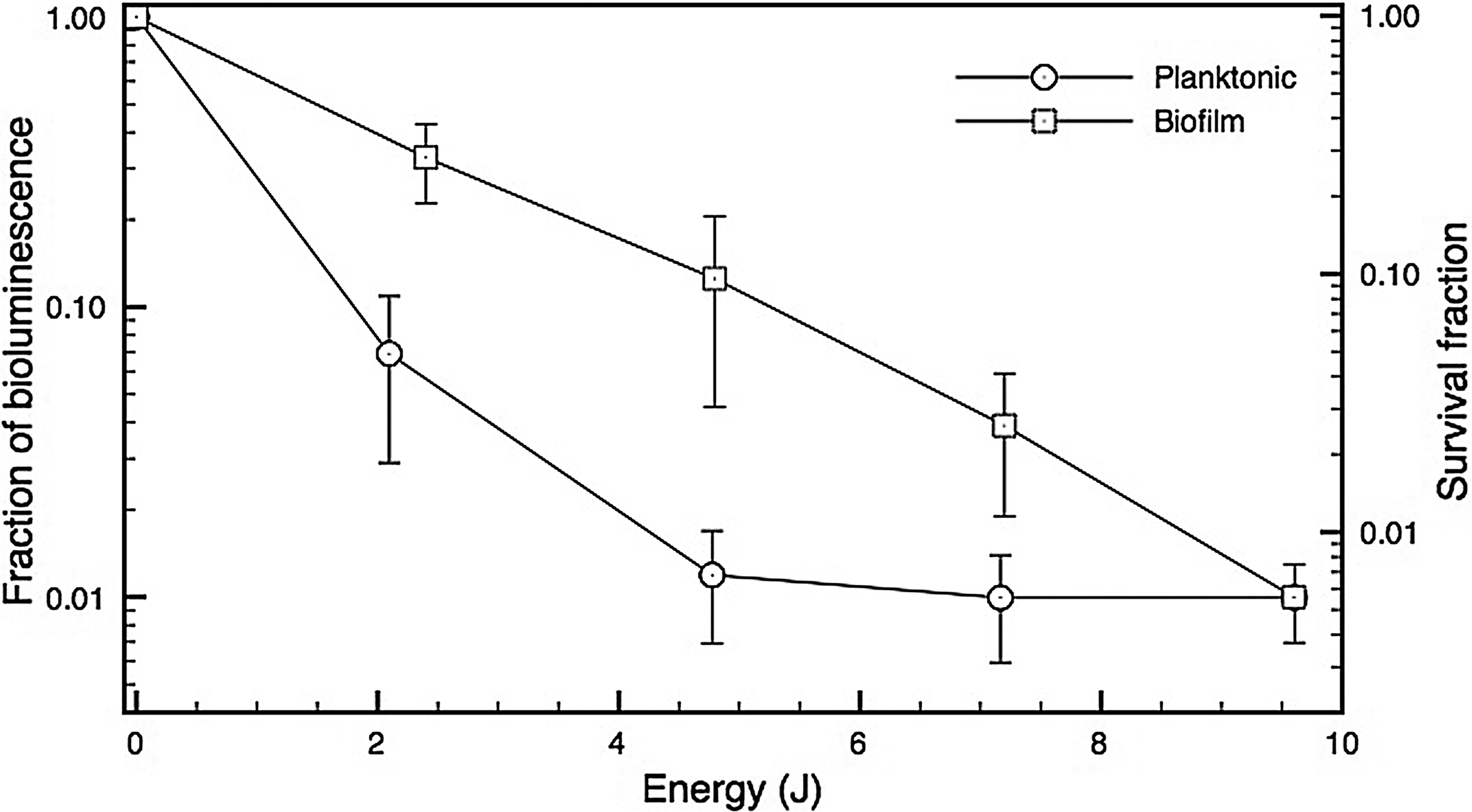
Comparative loss of bacterial viability as measured by fraction of bioluminescence signal remaining after incubation with 60 μM methylene blue (MB) for 2 min and after photodynamic therapy (PDT) using 660-nm light on a Pseudomonas. aeruginosa suspension or intracanal biofilm.
The SEM analysis with E. faecalis 3 day biofilms showed a significant reduction of surface biofilm after PDT. Cellular aggregates surrounded by extracellular matrix could be observed in the biofilms produced by E. faecalis incubated with MB in the dark (Fig. 4, panels A and B). These biofilms are very similar to those of untreated controls (data not shown). PDT promoted disruption of the biofilm as can be seen in panels C and D. The presence of adherent bacteria and extracellular matrix were markedly reduced, and very few aggregated colonies were observed in the biofilm after PDT. As expected for E. faecalis, most of the remaining bacteria were presented as single cells or organized in short chains. There were changes on bacterial morphology (cocci shaped, size or chain aggregation) and the biofilm area was significantly reduced by 88.7% (initial area of 694 Mpx. and final area of 282 Mpx. – p<0.02 compared with the SEM image of biofilm after MB dark incubation [measured by the ImageJ software]).
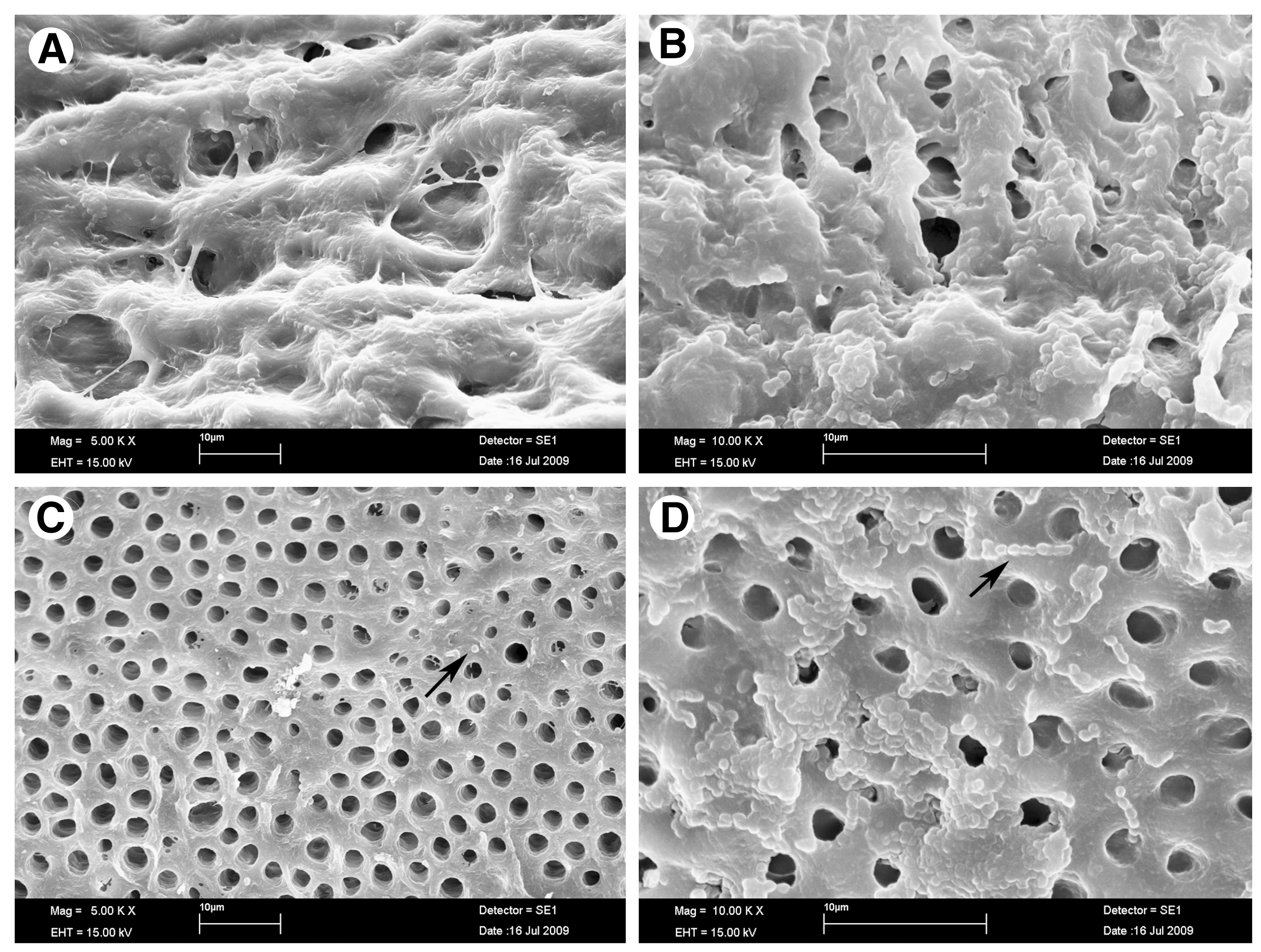
Scanning electron microscopic (SEM) image of a 3 day old biofilm of Enterococcus faecalis incubated with 60 μM of methylene blue (MB) for 2 min (
In the mixed biofilms, as expected, the reduction of E. faecalis (Gram+ bacteria) was higher than that observed for P. aeruginosa (Gram- bacteria), but it was possible to observe a definite alteration that was caused by PDT, resulting in disruption of the biofilm. There was a reduction of 59.3% in the area covered by the biofilm (initial area of 50 Mpx. and final image of 20.5 Mpx. – p=0.016) compared with the initial biofilm image on Fig. 5A, and additional changes in cell morphology could be observed (indicating probable membrane disruption); the alterations included loss of cocci or bacilli shape, and the presence of grooves on the cell surface. Features could be seen that suggested the presence of cell membrane shriveling, and draining of the intracellular components (Fig. 5A and B).

Scanning electron microscopic (SEM) images of a 3 day biofilm of Enterococcus. faecalis and Pseudomonas aeruginosa
Discussion
In this study, we examined biofilms formed by two bacteria (a Gram+ cocci E. faecalis and a Gram- bacilli P. aeruginosa) employing SEM and real-time bioluminescent imaging. We tested a photochemical strategy (methylene blue PDT) aiming to disrupt biofilm and reduce bacterial numbers. The results demonstrated that both species of bacteria could be reduced by PDT with MB and a 660 nm low-power diode laser in the two models used, the single and the mixed biofilm environment.
E. faecalis is a Gram-positive microorganism commonly detected in asymptomatic, persistent endodontic infections. Its prevalence in such infections ranges from 24% to 77%. 5 These data can be explained by various survival and virulence factors found in E. faecalis, including its ability to compete with other microorganisms, invade dentinal tubules, form biofilm, and resist nutritional deprivation. 23 P. aeruginosa was selected for this investigation based on its strong bioluminescence activity added to its propensity to form biofilms, and also there is pre-existing data classifying this microorganism 24 as an endodontic infectious species. Their morphology (Gram- rods 2–3 mm in length) is highly similar to other Gram-negative rods commonly found in endodontic infections. 25 Because bioluminescence imaging is a nondestructive method, the comparative evaluation of more than one procedure is possible. Sequential images could be obtained for each tooth, avoiding conventional methods that could interfere with biofilm structure. 1
The purpose of this study was to test PDT as an alternative approach against biofilm formed on dental hard tissue. The bacterial reduction showed energy-dose dependence; as the light energy increased, the bioluminescence signal decreased in both planktonic suspension and biofilm. Usually to describe the light irradiation parameters on PDT, the literature uses fluence (power×time/area) instead of total energy. In this study, we opted to use total energy (power×time), as it is difficult to calculate the area of a root canal, and the use of an optical fiber with spiral movements did not allow irradiation of the entire canal walls, but only a small area on each movement.
The bacterial reduction showed that the photosensitivity of planktonic bacteria was higher than bacteria in a biofilm. The energy used for inactivation of biofilm was higher than that required to inactivate planktonic bacterial suspension. According to Sharma et al., this difference could be for several reasons: cells in biofilm differ from their planktonic counterparts in a number of ways, such as cell wall composition, rate of growth, and presence of a self-produced extracellular polymeric matrix composed mainly of a large polysaccharide referred to as polysaccharide intercellular adhesins (PIA), which may hinder the uptake of the PS and also obstruct the penetration of light, thereby reducing the efficiency of the photodynamic process.
The SEM analysis showed large cellular aggregates enclosed by an extracellular matrix in all the biofilms treated with MB in dark conditions (Fig. 4 A and B). The images of the biofilm (E. faecalis) after PDT show a reduction in the number of adherent bacteria grouped in very few aggregated colonies; most of them were single cells or organized in short chains. The images were very similar to the biofilm images obtained by Di Poto et al. 26 and Sharma et al. 27 even though, in these studies, the authors had worked with staphylococcal biofilms. The significant reduction of the Gram-positive E. faecalis biofilm (89%) was higher than the reduction obtained with the Gram-negative P. aeruginosa. It is well known that Gram-positive bacteria are more easily killed by PDT than Gram negative species, most likely because of the difference in membrane structure between the two classes. 7
Our results with the bioluminescent Gram-negative bacteria biofilm reduction are lower than those reported by Sharma et al. 27 and Zanin et al. 19 who used, respectively, staphylococcal and streptococcal biofilms (Gram+ bacteria), and in addition to morphological differences among the species, this fact could be the result of different experimental conditions, the diverse nature of the biofilm, and/or substrate interaction. The results with mixed biofilm confirm this statement, as it is possible to see on Fig. 5.
The most common substrate for biofilm study is polystyrene as the material comprising 96 or 24 well plates, but other biomaterials have been employed such as anionic hydrogel copolymers used to build intraocular lenses. 28 In this study, we used dentine from human root canal surface as a substrate. The organic substrate makes it possible to obtain a more adherent biofilm, and therefore enhance the PDT challenge. It also mimics the clinical condition in a more realistic manner, and experiments conducted on polycarbonate or glass substrate may not provide a true indication of the biofilm–substrate interaction. 29
Dentin is a tissue composed of an organic fraction, which is mainly collagen, and an inorganic fraction, essentially carbonated hydroxyapatite. Certain bacteria can attach to dentin collagen through the expression of surface adhesins, and then go on to form biofilms. 30 PDT has shown to be a suitable approach to disrupt and inactivate biofilms adherent to biological tissue, if the target can be reached by the light and the PS. The PDT effect seems to act on both cells, promoting killing and membrane changes, and also on the extracellular matrix, disturbing the microbiological environment and facilitating the elimination of the remaining structures by irrigation.
Therefore, the use of PDT against oral infections could be an interesting approach for the treatment of diseases related to biofilm presence, such as dental caries, periodontal pockets, and root canal infections.
Conclusions
In this article, we examined the effects of PDT with MB and a 660 nm diode laser on biofilms grown on dental tissue. PDT successfully reduced the survival of P. aeruginosa and E. faecalis cells in biofilms. The bacterial reduction showed energy dependence, and the energy used for inactivation of biofilm was higher than that required for planktonic suspension. The photodynamic effect seemed to act both on cells, promoting killing and membrane alterations, and on the extracellular matrix, disrupting biofilm structure.
Footnotes
Acknowledgments
Dr. Hamblin was supported by United States National Institutes of Health (US NIH) grant R01AI050875. M.S. Ribeiro thanks FAPESP (Fundação de Amparo e Pesquisa do Estado de São Paulo) and CNPq (Conselho Nacional de Pesquisa e Desenvolvimento) for financial support.
Author Disclosure Statement
No competing financial interests exist.